

Abstract
Purpose
To estimate Swedish experience-based value sets for EQ-5D health states using general population health survey data.
Methods
Approximately 45,000 individuals valued their current health status by means of time trade off (TTO) and visual analogue scale (VAS) methods and answered the EQ-5D questionnaire, making it possible to model the association between the experience-based TTO and VAS values and the EQ-5D dimensions and severity levels. The association between TTO and VAS values and the different severity levels of respondents’ answers on a self-rated health (SRH) question was assessed.
Results
Almost all dimensions (except usual activity) and severity levels had less impact on TTO valuations compared with the UK study based on hypothetical values. Anxiety/depression had the greatest impact on both TTO and VAS values. TTO and VAS values were consistently related to SRH. The inclusion of age, sex, education and socioeconomic group affected the main effect coefficients and the explanatory power modestly.
Conclusions
A value set for EQ-5D health states based on Swedish valuations has been lacking. Several authors have recently advocated the normative standpoint of using experience-based values. Guidelines of economic evaluation for reimbursement decisions in Sweden recommend the use of experience-based values for QALY calculations. Our results that anxiety/depression had the greatest impact on both TTO and VAS values underline the importance of mental health for individuals’ overall HRQoL. Using population surveys is in line with recent thinking on valuing health states and could reduce some of the focusing effects potentially appearing in hypothetical valuation studies.
Electronic supplementary material
The online version of this article (doi:10.1007/s11136-013-0496-4) contains supplementary material, which is available to authorized users.
Keywords: EQ-5D, Experience-based value set, General population, Self-rated health, Time trade off, Visual analogue scale
Introduction
EQ-5D is a generic health-related quality of life (HRQoL) instrument from which a single-index value of the respondent’s health status can be derived, based on a health profile consisting of five dimensions with three severity levels [1]. EQ-5D is commonly used to estimate the quality-of-life component in quality-adjusted life years (QALYs) in the economic evaluation of health technologies, and also as a health care performance indicator and in the measurement of population health in surveys [2–6]. In determining values for the 243 health states defined by the EQ-5D, referred to as a value set, methods of valuation as well as the source of the valuations must be considered [7–10]. Although EQ-5D has been widely adopted in Sweden for economic evaluation, no value set based on a Swedish population has yet been developed.
A value set can be obtained using different methods for the valuation of health states: the time trade off (TTO), the standard gamble (SG), the rating scale (RS) and the discrete choice (DC) method [4, 11]. A central question is whether the valuations should be based on preferences from individuals who are actually in the health state, i.e., experience-based values, or from individuals to whom the health states are described, i.e., hypothetical values [8, 12–22]. The former is often denoted patient or individual values, and the latter social values (a sample of the general public has valued imagined health states). Experience-based values refer to the value of the individual’s currently experienced health state. However, in the valuation process, also imagined states are involved: worst and best, full health and dead.
A country-specific value set for EQ-5D health states was first generated in the UK [23] based on hypothetical values derived from a sample of the general population using the TTO method [9]. Country-specific value sets based on VAS data for hypothetical health states [9], a regional value set based on aggregated VAS data from six European countries [24] and a TTO value set from a Hispanic population in the US [25] have also been generated. Cross-country value set comparison studies suggest that there might be substantial differences in values across countries [9, 26–32].
Hypothetical values have been supported by the arguments that health policies and interventions affect us all (as tax payers and potential patients) and that the adaptation to a health state should not be reflected in valuations [33]. In contrast, advantages of using experience-based values based on preferences from the best informed [12, 14–16, 34–36] imply that adaptation will be reflected in the valuations [37–39]. Experience-based values tend to be higher than hypothetical values [8, 22, 39].
An experience-based VAS value set for EQ-5D has been developed for the German population [35]. Experience-based TTO values for EQ-5D health states have also been investigated [16] as well as experience-based VAS values [34, 36].
The National Institute for Health and Clinical Excellence (NICE) in England and Wales recommends using the UK EQ-5D ‘social tariff’ based on hypothetical values for QALY weightings [40]. In Sweden, the Dental and Pharmaceutical Benefits Agency (TLV) states that QALY weightings can be based either on direct or indirect measurements (‘where a health classification system such as EQ-5D is linked to QALY weightings’) and that ‘QALY weightings based on appraisals of persons in the health condition in question are preferred before weightings calculated from an average of a populations estimating a condition depicted for it (e.g., the ‘social tariff’ from EQ-5D)’ [41]. Thus, TLV prefers experience-based rather than hypothetical values [41].
This study attempted to estimate Swedish experience-based value sets for EQ-5D health states using general population health survey data. In the surveys, respondents valued their current health status by means of the TTO and VAS methods and answered the EQ-5D questionnaire, making it possible to model the association between the experience-based TTO and VAS values and the dimensions and severity levels of the EQ-5D instrument. For validation purposes, the association between TTO and VAS values and different severity levels of respondents’ answers on a self-rated health (SRH) question was investigated. Supplementary detail on data and variables as well as results is found in Online Resource (11136_2013_496_MOESM1_ESM.pdf).
Data and variables
Material/study population
In this study, we use large cross-sectional population-based health surveys from two areas in Sweden representing one-third of the Swedish population. The surveys (the Public Health Survey in Scania Region 2004 and the Public Health Survey in Stockholm County 2006) included the same questions. The analysis was carried out on a pooled data set.
In Sweden, a majority of the population live in urban areas. The socio-demographic composition of Scania Region resembles to a greater extent Sweden as a whole than does Stockholm County (Online Resource Table S1), where a smaller proportion live outside urban areas, and the mean age is lower; the educational and income levels are higher.
Self-administered postal questionnaires, with three reminders, were sent out to representative samples stratified by sex and geographic area. The EQ-5D self-report descriptive system, a visual analogue scale (EQ VAS), a time trade off (TTO) question and a SRH question were included in the surveys along with questions on living habits and conditions.
Data consisted of responses from 51,254 individuals, aged 18–80 years. See Online Resource for details.
The anonymised data are based on information from individuals who agreed to participate (informed consent), and respondents cannot be traced. Ethical approval was granted by the Regional Ethical Review Board, Stockholm (Dnr: 2011/582-31/5).
The EQ-5D descriptive system
With the EQ-5D descriptive system, respondents classify their own health status into five dimensions: mobility; self-care; usual activities; pain/discomfort; anxiety/depression, within three levels of severity: no problems; moderate problems; severe problems, defining 243 health states (profiles) [1].
The EQ VAS
On the EQ VAS, respondents rate their own overall health status on a vertical VAS (100 = best imaginable health; 0 = worst imaginable health).
The TTO question
The TTO question consisted of a horizontal line, representing 0–10 years, where every year was marked and labelled 0, 1, 2, …, 10 years [42]. Every half year was marked, but not labelled. A similar TTO question has been employed in other studies [13, 16, 43, 44].
The SRH question
The SRH question was phrased ‘In your opinion, how is your health status? Is it very good, good, fair, bad, very bad’?
Methods
We performed regression analysis on the individual data of all respondents with TTO and VAS values as the dependent variables. The variables and the definition of models are presented in Table 1. See Online Resource for analyses stratified by survey and test for parameter homogeneity across surveys.
Table 1.
Definition of variables and models
| Variable | Definition |
|---|---|
| MO2 | 1 if mobility at level 2; 0 otherwise |
| MO3 | 1 if mobility at level 3; 0 otherwise |
| MO23 | 1 if mobility at level 2 or 3; 0 otherwise |
| SC2 | 1 if self-care at level 2; 0 otherwise |
| SC3 | 1 if self-care at level 3; 0 otherwise |
| SC23 | 1 if self-care at level 2 or 3; 0 otherwise |
| UA2 | 1 if usual activities at level 2; 0 otherwise |
| UA3 | 1 if usual activities at level 3; 0 otherwise |
| PD2 | 1 if pain/discomfort at level 2; 0 otherwise |
| PD3 | 1 if pain/discomfort at level 3; 0 otherwise |
| AD2 | 1 if anxiety/depression at level 2; 0 otherwise |
| AD3 | 1 if anxiety/depression at level 3; 0 otherwise |
| N3 | 1 if any dimension at level 3; 0 otherwise |
| SRH2 | 1 if SRH is good health; 0 otherwise |
| SRH3 | 1 if SRH is fair health; 0 otherwise |
| SRH4 | 1 if SRH is bad health; 0 otherwise |
| SRH5 | 1 if SRH is very bad; 0 otherwise |
| TTO models on EQ-5D | f (x) |
|---|---|
| Model 1 | f (MO2 MO3 SC2 SC3 UA2 UA3 PD2 PD3 AD2 AD3) |
| Model 2 | f (MO2 MO3 SC2 SC3 UA2 UA3 PD2 PD3 AD2 AD3 N3) |
| Model 3 | f (MO2 MO3 SC23 UA2 UA3 PD2 PD3 AD2 AD3) |
| Model 4 | f (MO2 MO3 SC23 UA2 UA3 PD2 PD3 AD2 AD3 N3) |
| Model 5 | f (MO2 MO3 SC23 UA2 UA3 PD2 PD3 AD2 AD3 N3 age) |
| Model 6 | f (MO2 MO3 SC23 UA2 UA3 PD2 PD3 AD2 AD3 N3 age sex) |
| Model 7 | f (MO2 MO3 SC23 UA2 UA3 PD2 PD3 AD2 AD3 N3 age sex educational level socioeconomic group) |
| VAS models on EQ-5D | f (x) |
|---|---|
| Model 1 | f (MO2 MO3 SC2 SC3 UA2 UA3 PD2 PD3 AD2 AD3) |
| Model 2 | f (MO2 MO3 SC2 SC3 UA2 UA3 PD2 PD3 AD2 AD3 N3) |
| Model 3 | f (MO23 SC23 UA2 UA3 PD2 PD3 AD2 AD3) |
| Model 4 | f (MO23 SC23 UA2 UA3 PD2 PD3 AD2 AD3 N3) |
| Model 5 | f (MO23 SC23 UA2 UA3 PD2 PD3 AD2 AD3 N3 age) |
| Model 6 | f (MO23 SC23 UA2 UA3 PD2 PD3 AD2 AD3 N3 age sex) |
| Model 7 | f (MO23 SC23 UA2 UA3 PD2 PD3 AD2 AD3 N3 age sex educational level socioeconomic group) |
| TTO and VAS models on SRH | f (x) |
|---|---|
| Model 1 | f (SRH2 SRH3 SRH4 SRH5) |
| Model 2 | f (SRH2 SRH3 SRH4 SRH5 age) |
| Model 3 | f (SRH2 SRH3 SRH4 SRH5 age sex) |
| Model 4 | f (SRH2 SRH3 SRH4 SRH5 age sex educational level socioeconomic group) |
TTO time trade off, VAS visual analogue scale, SRH self-rated health
The individual TTO value was calculated by dividing the response to the TTO question by 10. The trade off was between x years in full health versus 10 years in the respondent’s current health state; shorter time implied worse health state. The individual VAS value was given by the numeric value on the VAS between 0 and 100. The VAS values were not rescaled to be anchored on dead and full health and could hence not directly be used in QALY calculations.
A set of ten dummy variables was representing the main effect within each of the five EQ-5D dimensions (Model 1) [23]. The dummy variables for level 2 represents the main effect of movement from level 1 (no problems) to level 2 (moderate problems), and the dummy variables for level 3 represents the main effect of movement from level 1 (no problems) to level 3 (severe problems) (Table 1).
Interaction variables were tested: first order interaction effects between the five EQ-5D dimensions; if levels 2 or 3 in any of the dimensions (N2 and N3, respectively); the number and the square of the number of dimensions on levels 2 or 3; whether there are two or more, three or more, four or more, or five dimensions on levels 2 or 3.
We expected consistent ordering between the levels, i.e., that all coefficients should have a negative sign and that the coefficient for severe problems should be greater in absolute terms than the coefficients for moderate problems. However, in the TTO analyses for the self-care dimension, the coefficient for severe problems was smaller than the coefficient for moderate problems, and this could not be handled by entering interaction or other nonlinear variables in any of the models. Therefore, we merged levels 2 and 3 into one category and entered a dummy variable (SC23) representing any move from level 1 (no problems) in the self-care dimension. In the VAS analyses, a similar inconsistency was observed for the self-care and mobility dimensions, and additional dummy variables (SC23 and MO23) were entered. None of the interaction coefficients were significant, except the N3 variable, and were not entered in the final model.
We estimated ordinary least squares (OLS) regressions with the ten dummy variables for the dimensions (Model 1) and with the N3 variable (Model 2). We merged levels 2 and 3 for self-care or mobility (Model 3) and included the N3 variable (Model 4), respectively, in the TTO and VAS regressions.
Statistical tests were employed to evaluate the models’ goodness-of-fit: the estimated values predicted by the models were compared with the observed values by calculating Spearman’s correlation coefficients and the mean absolute difference (MAD). The higher correlations, the better the model fit and the smaller MAD, the better the model fit.
The final choice of model specification (Model 4) for the estimation of TTO and VAS value sets was based on the following criteria: the ordinal nature of the severity levels within each dimension should be reflected (consistency); how well the model explains the differences between estimated and observed health state values (goodness-of-fit); the simplicity of the model (parsimony); and that non-experts can understand the modelling (transparency) [45].
To estimate the robustness of the final model, a split sample test was employed, where the total sample was randomly divided into two groups of equal size [23]. Estimations from one group were used to predict the values in the other group.
In addition, we investigated the effect of age (Model 5), sex (Model 6), education and socioeconomic group (Model 7) on valuation of health states (Table 1) (see Online Resource for classification).
Furthermore, we explored the effect of SRH on TTO and VAS values, respectively (Table 1). Dummy variables were created representing the severity levels (reference group very good health) (Model 1). The dummy variables represent the effect of movement from very good health to good, fair, bad and very bad health, respectively. We estimated the regression models with and without the above-described socio-demographic dummy variables (Models 2–4).
Since there were indications of heteroscedasticity, robust estimates were employed [46]. A 5 % significance level was used. All analyses were carried out in SAS Version 9.2 [47].
Results
Of the 243 possible health states of the EQ-5D descriptive system, 148 health states were reported and valued. Socio-demographic characteristics and self-reported health measures for the pooled data are presented in Table 2. See Online Resource Table S2 for characteristics by survey.
Table 2.
Characteristics of the respondents, pooled data
| Variable | 18–80 years | |
|---|---|---|
| (n = 49,169) | ||
| % | n | |
| Women | 56.3 | 27,700 |
| Mean age (years) | 46.2 | 49,169 |
| Age group | ||
| 18–24 years | 9.1 | 4,483 |
| 25–34 years | 16.8 | 8,239 |
| 35–44 years | 20.9 | 10,295 |
| 45–54 years | 19.9 | 9,804 |
| 55–64 years | 22.6 | 11,108 |
| 65–74 years | 7.5 | 3,692 |
| 75–80 years | 3.2 | 1,548 |
| Educational level | ||
| Low | 17.1 | 8,414 |
| Medium | 42.1 | 20,703 |
| High | 37.0 | 18,172 |
| Missing | 3.8 | 1,880 |
| Socioeconomic group | ||
| Unskilled manual | 17.9 | 8,788 |
| Skilled manual | 12.1 | 5,949 |
| Lower non-manual | 10.9 | 5,362 |
| Intermediate non-manual | 18.7 | 9,186 |
| Higher non-manual | 13.7 | 6,751 |
| Self-employed and farmers | 4.0 | 1,989 |
| Other | 22.7 | 11,144 |
| Less than good SRH | 27.7 | 13,593 |
| Mobility | ||
| Moderate problems (level 2) | 9.8 | 4,840 |
| Severe problems (level 3) | 0.1 | 50 |
| Self-care | ||
| Moderate problems (level 2) | 1.2 | 600 |
| Severe problems (level 3) | 0.4 | 198 |
| Usual activities | ||
| Moderate problems (level 2) | 7.7 | 3,785 |
| Severe problems (level 3) | 1.1 | 536 |
| Pain/discomfort | ||
| Moderate problems (level 2) | 45.1 | 22,185 |
| Severe problems (level 3) | 4.1 | 2,038 |
| Anxiety/depression | ||
| Moderate problems (level 2) | 30.8 | 15,126 |
| Severe problems (level 3) | 2.7 | 1,322 |
| Problems in at least one EQ-5D dimension | 60.2 | 29,618 |
| Problems on level 3 | 6.7 | 3,287 |
| TTO (mean) | 0.91 | 45,477 |
| EQ VAS (mean) | 79.5 | 41,761 |
TTO time trade off, VAS visual analogue scale, SRH self-rated health
Regression analysis on TTO values for EQ-5D dimensions
The results of the regression analysis on individual TTO values for EQ-5D dimensions are presented in Table 3.
Table 3.
Regression analysis on TTO values, EQ-5D dimensions
| Variable | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Estimate | p value | Estimate | p value | Estimate | p value | Estimate | p value | Estimate | p value | Estimate | p value | Estimate | p value | |
| Intercept | 0.9692 | <0.0001 | 0.9693 | <0.0001 | 0.9693 | <0.0001 | 0.9694 | <0.0001 | 0.9606 | <0.0001 | 0.9527 | <0.0001 | 0.9480 | <0.0001 |
| Mobility | ||||||||||||||
| Level 2 | −0.0665 | <0.0001 | −0.0660 | <0.0001 | −0.0668 | <0.0001 | −0.0666 | <0.0001 | −0.0638 | <0.0001 | −0.0634 | <0.0001 | −0.0623 | <0.0001 |
| Level 3 | −0.1464 | <0.0001 | −0.1500 | 0.0006 | −0.1298 | 0.0025 | −0.1247 | 0.0032 | −0.1234 | 0.0038 | −0.1218 | 0.0043 | −0.1217 | 0.0043 |
| Self-care | ||||||||||||||
| Level 2 | −0.0490 | <0.0001 | −0.0477 | 0.0002 | – | – | – | – | – | – | – | – | – | – |
| Level 3 | 0.0068 | 0.7308 | 0.0445 | 0.0481 | – | – | – | – | – | – | – | – | – | – |
| Level 2 and 3 | – | – | – | – | −0.0350 | 0.0015 | −0.0276 | 0.0161 | −0.0254 | 0.0273 | −0.0242 | 0.0350 | −0.0233 | 0.0425 |
| Usual activities | ||||||||||||||
| Level 2 | −0.1014 | <0.0001 | −0.0994 | <0.0001 | −0.1022 | <0.0001 | −0.1012 | <0.0001 | −0.1031 | <0.0001 | −0.1036 | <0.0001 | −0.1029 | <0.0001 |
| Level 3 | −0.1483 | <0.0001 | −0.1331 | <0.0001 | −0.1469 | <0.0001 | −0.1355 | <0.0001 | −0.1364 | <0.0001 | −0.1363 | <0.0001 | −0.1359 | <0.0001 |
| Pain/discomfort | ||||||||||||||
| Level 2 | −0.0347 | <0.0001 | −0.0346 | <0.0001 | −0.0347 | <0.0001 | −0.0345 | <0.0001 | −0.0348 | <0.0001 | −0.0355 | <0.0001 | −0.0337 | <0.0001 |
| Level 3 | −0.1236 | <0.0001 | −0.0759 | <0.0001 | −0.1242 | <0.0001 | −0.0904 | <0.0001 | −0.0926 | <0.0001 | −0.0935 | <0.0001 | −0.0911 | <0.0001 |
| Anxiety/depression | ||||||||||||||
| Level 2 | −0.0555 | <0.0001 | −0.0550 | <0.0001 | −0.0555 | <0.0001 | −0.0552 | <0.0001 | −0.0551 | <0.0001 | −0.0566 | <0.0001 | −0.0562 | <0.0001 |
| Level 3 | −0.2393 | <0.0001 | −0.1948 | <0.0001 | −0.2393 | <0.0001 | −0.2077 | <0.0001 | −0.2084 | <0.0001 | −0.2092 | <0.0001 | −0.2083 | <0.0001 |
| N3 | – | – | −0.0607 | <0.0001 | – | – | −0.0433 | 0.0017 | −0.0427 | 0.0020 | −0.0433 | 0.0017 | −0.0429 | 0.0018 |
| Age group a | ||||||||||||||
| 25–34 | – | – | – | – | – | – | – | – | 0.0097 | 0.0010 | 0.0096 | 0.0012 | 0.0030 | 0.3305 |
| 35–44 | – | – | – | – | – | – | – | – | 0.0080 | 0.0063 | 0.0084 | 0.0040 | 0.0008 | 0.7880 |
| 45–54 | – | – | – | – | – | – | – | – | 0.0135 | <0.0001 | 0.0144 | <0.0001 | 0.0071 | 0.0217 |
| 55–64 | – | – | – | – | – | – | – | – | 0.0158 | <0.0001 | 0.0170 | <0.0001 | 0.0096 | 0.0013 |
| 65–74 | – | – | – | – | – | – | – | – | 0.0038 | 0.2996 | 0.0051 | 0.1588 | 0.0007 | 0.8557 |
| 75–80 | – | – | – | – | – | – | – | – | −0.0413 | <0.0001 | −0.0397 | <0.0001 | −0.0329 | <0.0001 |
| Sex b | – | – | – | – | – | – | – | – | – | – | 0.0144 | <0.0001 | 0.0137 | <0.0001 |
| Educational level c | ||||||||||||||
| Medium | – | – | – | – | – | – | – | – | – | – | – | – | 0.0020 | 0.3889 |
| High | – | – | – | – | – | – | – | – | – | – | – | – | 0.0045 | 0.0825 |
| Missing | – | – | – | – | – | – | – | – | – | – | – | – | −0.0115 | 0.0818 |
| Socioeconomic group d | ||||||||||||||
| Skilled manual | – | – | – | – | – | – | – | – | – | – | – | – | 0.0065 | 0.0229 |
| Lower non-manual | – | – | – | – | – | – | – | – | – | – | – | – | 0.0120 | <0.0001 |
| Intermed non-manual | – | – | – | – | – | – | – | – | – | – | – | – | 0.0132 | <0.0001 |
| Higher non-manual | – | – | – | – | – | – | – | – | – | – | – | – | 0.0161 | <0.0001 |
| Self-employed | – | – | – | – | – | – | – | – | – | – | – | – | 0.0166 | <0.0001 |
| Other | – | – | – | – | – | – | – | – | – | – | – | – | 0.0010 | 0.6975 |
| Observations | 45.477 | 45.477 | 45.477 | 45.477 | 45.477 | 45.477 | 45.477 | |||||||
| Adjusted R 2 | 0.2385 | 0.2393 | 0.2383 | 0.2387 | 0.2415 | 0.2431 | 0.2446 | |||||||
| F statisticse, f | F (1,41185) = 108.39* | F (1,41184) = 106.78* | F (1,41186) = 106.95* | F (1,41185) = 105.43* | F (1,41185) = 105.43* | F (1,41185) = 105.43* | F (1,41185) = 105.43* | |||||||
| F statisticse, g | F (19,41197) = 4.20* | F (10,41175) = 12.42* | F (28,41157) = 6.72* | |||||||||||
| F statisticse, h | F (10,41175) = 6.21* | F (11,41173) = 5.54* | F (9,41177) = 6.72* | F (10,41175) = 5.88* | F (29,41167) = 5.94* | F (10,41165) = 5.90* | F (10,41147) = 6.11* | |||||||
TTO time trade off
* p = 0.001
aReference group: 18–24 years
bReference group: men
cReference group: low educational level
dReference group: unskilled manual workers
eAge restricted to 18–64 years
f F test of equal intercepts in the two surveys
g F test of equal parameters of all non-dimensional regressors in the two surveys
h F test of equal parameters of all dimensional regressors in the two surveys
Model 1 includes the main effect within each of the five dimensions with dummy variables entered for moderate and severe levels. The TTO results were consistent that the values were lower, the more severe the health state, except for self-care where the coefficient for level 3 was not lower compared to level 2. The N3 variable had a negative sign and was significant (Model 2). Entering the SC23 variable (merged levels 2 and 3 for self-care) resulted in all coefficients for all dimensions becoming statistically significant irrespective of the exclusion (Model 3) or inclusion (Model 4) of the N3 variable.
For health states with ten or more observations, the Spearman’s correlation coefficients were greater and the MAD smaller, compared with states with five or more observations (Table 4). For health states with five or more observations, the correlation coefficient was greater and the MAD was smaller in Model 4 compared to Model 3. For health states with ten or more observations, the correlation coefficient was greater and the MAD was smaller in Model 3. However, the differences between all models were small. The adjusted R 2 was similar for all four models (around 0.24) (Table 3).
Table 4.
Correlation and mean absolute difference (MAD), TTO values, EQ-5D
| Number of health states | TTO | |||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |||||
| Correlation | MAD | Correlation | MAD | Correlation | MAD | Correlation | MAD | |
| n ≥ 5 | 0.833 | 0.0552 | 0.849 | 0.0506 | 0.824 | 0.0560 | 0.830 | 0.0539 |
| n ≥ 10 | 0.936 | 0.0389 | 0.934 | 0.0385 | 0.933 | 0.0404 | 0.928 | 0.0408 |
TTO time trade off
Figure 1 shows the estimated TTO values predicted by the different OLS models compared to the observed mean TTO values for health states with five or more observations.
Fig. 1.
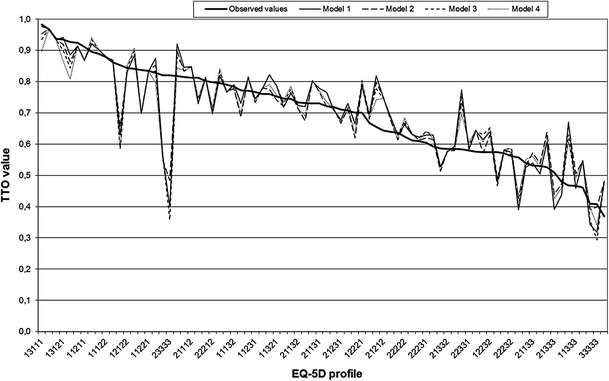
Estimated TTO values predicted by different OLS models compared to the observed mean TTO values for health states with five or more observations (n = 80)
The consistency criteria together with the goodness-of-fit analyses and the fact that the N3 variable was significant resulted in Model 4 being the best-fitting model for the data. Severe problems with anxiety/depression had the greatest effect (0.208), followed by severe problems with usual activities (0.136), mobility (0.125) and pain/discomfort (0.090) (Table 3). For moderate problems, the greatest coefficient was seen for usual activities (0.101) followed by mobility (0.067), anxiety/depression (0.055) and pain/discomfort (0.035). The merged coefficient for self-care (0.028) was interpreted as any move away from no problems. The difference between the predicted and the observed mean values exceeded 0.1 for 15 % of the health states with five or more observations.
The coefficients for age were significantly positive for nearly all age groups and negative for the oldest (Model 5). The coefficient for sex was significant with higher TTO values for women (Model 6), while the coefficients for educational level were not significant (Model 7). The coefficients for socioeconomic groups were positive and significant. Including age, sex, education and socioeconomic group affected the main effect coefficients modestly and increased the adjusted R 2 from 0.239 to 0.245.
A Swedish TTO value set, based on Model 4, for the 243 EQ-5D health states, is presented in Online Resource Table S3.
Regression analysis on VAS values for EQ-5D dimensions
Corresponding results of the regression analysis on individual VAS values for EQ-5D dimensions and model comparison are presented in Online Resource Tables S4–S5 and Figure S1.
A Swedish VAS value set, based on Model 4, for the 243 health states, is presented in Online Resource Table S3.
Comparison of TTO and VAS values for Models 2 and 4 is presented in Online Resource Table S6 (pooled data) and Table S7 (by survey).
Regression analysis on TTO values and VAS values for SRH
Corresponding results of the regression analysis on individual TTO and VAS values for SRH levels are presented in Online Resource Table S8.
The TTO and VAS values for the different severity levels for SRH are presented in Online Resource Table S9.
Comparison of TTO and VAS values for SRH levels is presented in Online Resource Table S10 (pooled data) and Table S11 (by survey).
Discussion
Although tentative valuation studies have been performed previously in Sweden [13, 48], this is the first attempt to estimate a Swedish value set for EQ-5D health states. In two large cross-sectional population-based surveys, individuals described their current health status in the EQ-5D descriptive system and valued their health status using TTO and VAS. In line with recent studies [16, 34, 35], statistical modelling was used to model the association between the experience-based values and the dimensions and severity levels of the EQ-5D descriptive system. The preferred OLS models included an N3 variable and discriminated consistently between severity levels in the five dimensions except for self-care for both TTO and VAS, and mobility for VAS. Other studies have also encountered inconsistencies with coefficients having the wrong sign or being non-significant; several studies also appeared to encounter similar issues with self-care [35, 49–51], possibly due to the low prevalence of any problems on the self-care dimension. Age could also be a factor as problems with self-care are more prevalent among older respondents, who may be more prone to misunderstand the valuation task [52].
To handle the inconsistencies, we merged levels 2 and 3 resulting in a significant coefficient for self-care in the TTO regression. In the VAS regression, the re-specification resulted in a significant coefficient for mobility, but not for self-care (although this coefficient was kept as it had the correct sign). With this approach, the N3 variable still distinguishes between moderate and severe problems within self-care and mobility for health states where no other dimension is at the severe level as this coefficient is applied only once if any dimension is at the severe level. Inconsistent coefficients have sometimes been omitted altogether [35, 50, 52], implying that health states are assigned the same value in the value set, whereas other have kept insignificant (but logically plausible) coefficients [23, 51]. As inconsistencies occur in both experience-based studies and studies based on hypothetical values, other explanations than sources of valuations are likely. The MAD for our TTO and VAS models were smaller compared with other studies [53].
Although caution is warranted in comparing different studies [32], our TTO value set shows a general trend towards higher values compared with the UK TTO value set [23]. Almost all dimensions and severity levels in our study have less impact on TTO valuations (except usual activity) compared with the UK study. In particular, the differences appear more pronounced for severe health states as indicated by the much smaller coefficients for level 3 and N3 in our study; a similar trend was observed when comparing our results to Danish hypothetical TTO values [53]. Previous studies have shown that experience-based values tend to be higher than hypothetical values, in particular for severe health states [13, 22, 36, 39, 54, 55]. The relative importance of the health dimensions also appears to differ between experience-based and hypothetical values; problems in the mood dimension seem to be valued worse when values are experience-based [8, 12, 14].
Our study sample has strengths and weaknesses. The size of our study sample provides a strong foundation for the statistical modelling. Approximately 45,000 individuals provided valuations of about 60 % of the EQ-5D health states, and 80 of the health states were valued by five or more individuals. A potential limitation is that two cross-sectional population-based health surveys from different areas of Sweden were used in the absence of a national sample of Sweden. However, our large sample represents one-third of the Swedish population and is broadly representative of the Swedish population in terms of basic characteristics, suggesting that the results may be generalizable to Sweden as a whole. Although the inclusion of age, sex, education and socioeconomic group affected the main effect coefficients and the explanatory power modestly, the analyses revealed some interesting findings. TTO values were significantly positive for nearly all age groups and had a negative sign for the oldest indicating that age might be a further health indicator in addition to the five dimensions. TTO values were higher for women, while the coefficients for education did not reveal any significant differences. The coefficients for socioeconomic groups were positive and significant. Heterogeneity across surveys was observed. In the 2004 survey, anxiety/depression had greater impact and the N3 coefficient was greater; in the 2006 survey, usual activities had greater impact, on both TTO and VAS values. This may reflect the socio-demographic composition of the samples. Further research should investigate differences in valuation due to socio-demographic or other possible unobserved variables. The relatively high non-response rate for VAS in the 2004 survey is a matter of concern to which we have no explanation. However, the non-responders to VAS were similar to other non-responders.
The VAS scale was anchored between worst and best imaginable health which did not allow for anchoring between 0 (dead) and 1 (full health). Hence, these raw and estimated VAS values do not correspond to the 0–1 scale requirement for QALY calculations. We did not rescale the VAS values due to the ambiguity of where on the scale dead should be placed [56, 57]. If the VAS values should be used for QALY calculations, rescaling is necessary [24].
The observed and the predicted mean TTO value for the health state 11111 is 0.97. It is logical that this value is somewhat below 1, as individuals may have health problems in dimensions not covered by the EQ-5D. They may also have some health problems in the five dimensions that are not sufficiently severe to tick the ‘moderate problems box’ (with only three categories in a dimension, individuals will have to pick the category perceived as closest to their health state). It is in principle possible to rescale the predicted TTO values so that the health state 11111 is defined as 1. However, we do not recommend such rescaling as it would convert responses to a scale that differs from directly measured TTO values (and the two would thus not be directly comparable).
Our study also showed that TTO and VAS valuations were consistently related to SRH. In studies employing SRH as a measure of health status, our results can be used to apply cardinality on the ordinal responses to the SRH question [58–60].
Several authors have recently advocated the normative standpoint of using experience-based values [15, 34–36, 61, 62]. The experience-based values in our study are from population surveys, which is in line with recent thinking on valuing health states [12, 15] and could reduce some of the focusing effects that are likely to appear in hypothetical valuation studies [14, 15]. In a general population health survey, respondents may be more focused on their overall perceptions of their health status (and thus the valuation of the EQ-5D health state) without framing this perception into a particular disease condition or the actual dimensions and levels of the EQ-5D descriptive system. Our study also takes into consideration one argument for using so called social values; namely that health policies and intervention affect us all (as tax payers and potential patients), and therefore, values should be representative of the Swedish population, i.e., not representing a narrowly defined group of patients.
The normative question on whose values to use, or what value set, may have implications for economic evaluation and ultimately resource allocation [12, 39]. In our study, anxiety/depression has the greatest impact on both TTO and VAS values, as suggested in other studies [12, 14] followed by usual activities. The results underline the importance of mental health for individuals’ overall HRQoL. For TTO values, mobility has greater impact than pain/discomfort, whereas the opposite was seen for VAS values. If values are based on preferences for hypothetical health states, an intervention may seemingly lead to a greater gain than if values based on self-perceived health states are used, due to the lower values which are usually assigned when considering hypothetical health states. Whether this is an overestimation of the gain depends on whose preferences are considered most appropriate. The relative influence of HRQoL on QALY calculations is also affected by whose values are used.
Visual analogue scale (VAS) is not a choice-based method and the values were not anchored between dead and full health. Furthermore, there was an additional inconsistency (mobility) in the VAS model implying that more health states are not distinguished with the VAS value set. We therefore prefer the TTO value set. However, presentation of two value sets enables users to make their own judgement regarding which value set to use.
Swedish authors recommended the use of experience-based values in 1996 [18], and the Swedish reimbursement authority [41] recommended the use of experience-based values in 2003. Despite this fact, the UK TTO value set is predominantly used in Sweden. This may partly be due to lack of alternative value sets, and therefore, the results reported in this work represents a step towards value sets for EQ-5D health states that are based on Swedish experience-based values. The practical and normative implications of implementing the Swedish value sets in studies and subsequent health care decisions may warrant further discussion and investigation.
Furthermore, testing the performance of the value sets by assessing how the predicted values correspond to directly measured values in other populations is an interesting area for further research.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Acknowledgments
We would like to thank Stockholm County Council for providing data from the Public Health Survey 2006 and Region Scania for providing data from the Public Health Survey 2004, especially Per-Olof Östergren, Maria Rosvall and Mathias Grahn. All valuable discussions in the Equity and Health Policy Research Group at Karolinska Institutet are gratefully acknowledged. Kristina Burström and Sun Sun are employed by Stockholm County Council, data were collected within the scope of their follow-up activity, and the County Council have had no influence on the analyses or on the interpretation of findings. The authors have no conflict of interest to declare. We would also like to thank the anonymous reviewers and the editor for their valuable comments and constructive suggestions.
References
- 1.Rabin R, de Charro F. EQ-5D: A measure of health status from the EuroQol group. Annals of Medicine. 2001;33(5):337–343. doi: 10.3109/07853890109002087. [DOI] [PubMed] [Google Scholar]
- 2.Burström K, Johannesson M, Diderichsen F. The value of the change in health in Sweden 1980/81 to 1996/97. Health Economics. 2003;12(8):637–654. doi: 10.1002/hec.754. [DOI] [PubMed] [Google Scholar]
- 3.Devlin NJ, Parkin D, Browne J. Patient-reported outcome measures in the NHS: new methods for analysing and reporting EQ-5D data. Health Economics. 2010;19(8):886–905. doi: 10.1002/hec.1608. [DOI] [PubMed] [Google Scholar]
- 4.Drummond MF, Sculpher MJ, Torrance GW, O’Brien BJ, Stoddart GL. Methods for the economic evaluation of health care programmes. 3. New York: Oxford Medical Publications; 2005. [Google Scholar]
- 5.Broome J. QALYs. Journal of Public Economics. 1993;50:149–167. doi: 10.1016/0047-2727(93)90047-W. [DOI] [Google Scholar]
- 6.Williams A. Economics of coronary artery bypass grafting. British Medical Journal. 1985;291(6491):326–329. doi: 10.1136/bmj.291.6491.326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Dolan P. The measurement for health-related quality-of-life for use in resource allocation decisions in health care. In: Culyer AJ, Newhouse J, editors. Handbook of health economics. Amsterdam: North-Holland; 2000. pp. 1723–1760. [Google Scholar]
- 8.Mann R, Brazier J, Tsuchiya A. A comparison of patient and general population weightings of EQ-5D dimensions. Health Economics. 2009;18(3):363–372. doi: 10.1002/hec.1362. [DOI] [PubMed] [Google Scholar]
- 9.Szende A, Oppe M, Devlin N, editors. EQ-5D value sets: Inventory, comparative review and user guide. Dordrecht: Springer; 2007. [Google Scholar]
- 10.Ubel PA, Loewenstein G, Hershey J, Baron J, Mohr T, Asch D, et al. Do nonpatients underestimate the quality of life associated with chronic health conditions because of a focusing illusion? Medical Decision Making. 2001;21(3):190–199. doi: 10.1177/02729890122062488. [DOI] [PubMed] [Google Scholar]
- 11.Stolk EA, Oppe M, Scalone L, Krabbe PFM. Discrete choice modeling for the quantification of health states: The case of the EQ-5D. Value in Health. 2010;13(8):1005–1013. doi: 10.1111/j.1524-4733.2010.00783.x. [DOI] [PubMed] [Google Scholar]
- 12.Brazier J, Akehurst R, Brennan A, Dolan P, Claxton K, McCabe C, et al. Should patients have a great role in valuing health states? Applied Health Economics and Health Policy. 2005;4(4):201–208. doi: 10.2165/00148365-200504040-00002. [DOI] [PubMed] [Google Scholar]
- 13.Burström K, Johannesson M, Diderichsen F. A comparison of individual and social time trade-off values for health states in the general population. Health Policy. 2006;76(3):359–370. doi: 10.1016/j.healthpol.2005.06.011. [DOI] [PubMed] [Google Scholar]
- 14.Dolan P. Developing methods that really do value the ‘Q’ in the QALY. Health Economics, Policy and Law. 2008;3:69–77. doi: 10.1017/S1744133107004355. [DOI] [PubMed] [Google Scholar]
- 15.Dolan P, Kahneman D. Interpretations of utility and their implications for the valuation of health. The Economic Journal. 2008;118:215–234. doi: 10.1111/j.1468-0297.2007.02110.x. [DOI] [Google Scholar]
- 16.Dolan P. Thinking about it: Thoughts about health and valuing QALYs. Health Economics. 2011;20(12):1407–1416. doi: 10.1002/hec.1679. [DOI] [PubMed] [Google Scholar]
- 17.Insinga RP, Fryback DG. Understanding differences between self-ratings and populations ratings for health in the EuroQOL. (2003) Quality of Life Research. 2003;12(6):611–619. doi: 10.1023/A:1025170308141. [DOI] [PubMed] [Google Scholar]
- 18.Johannesson M, Jonsson B, Karlsson G. Outcome measurement in economic evaluation. Health Economics. 1996;5(4):279–296. doi: 10.1002/(SICI)1099-1050(199607)5:4<279::AID-HEC218>3.0.CO;2-J. [DOI] [PubMed] [Google Scholar]
- 19.Krabbe PFM, Tromp N, Ruers TJM, van Riel PLCM. Are patients’ judgements of health status really different from the general population? Health and Quality of Life Outcomes. 2011;9:31. doi: 10.1186/1477-7525-9-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.McNamee P. What difference does it make? The calculation of QALY gains from health profiles using patient and general population values. Health Policy. 2007;84(2–3):321–331. doi: 10.1016/j.healthpol.2007.05.004. [DOI] [PubMed] [Google Scholar]
- 21.McPherson K, Myers J, Talor WJ, McNaughton HK, Weatherall M. Self-valuation and societal valuations of health state differ with disease severity in chronic and disabling conditions. Medical Care. 2004;42(11):1143–1151. doi: 10.1097/00005650-200411000-00014. [DOI] [PubMed] [Google Scholar]
- 22.de Wit GA, Busschbach JJ, de Charro FT. Sensitivity and perspective in valuation of health status: Whose values count? Health Economics. 2000;9(2):109–126. doi: 10.1002/(SICI)1099-1050(200003)9:2<109::AID-HEC503>3.0.CO;2-L. [DOI] [PubMed] [Google Scholar]
- 23.Dolan P. Modeling valuations for EuroQol health states. Medical Care. 1997;35(11):1095–1108. doi: 10.1097/00005650-199711000-00002. [DOI] [PubMed] [Google Scholar]
- 24.Greiner W, Weijnen T, Nieuwenhuizen M, Oppe S, Busschbach J, Buxton M, et al. A single European currency for EQ-5D health states. European Journal of Health Economics. 2003;4(3):222–231. doi: 10.1007/s10198-003-0182-5. [DOI] [PubMed] [Google Scholar]
- 25.Zarate V, Kind P, Chuang LH. Hispanic valuation of the EQ-5D health states: a social value set for Latin Americans. Value in Health. 2008;11(7):1170–1177. doi: 10.1111/j.1524-4733.2008.00349.x. [DOI] [PubMed] [Google Scholar]
- 26.Badia X, Roset M, Herdman M, Kind P. A comparison of United Kingdom and Spanish general population time trade-off values for EQ-5D health states. Medical Decision Making. 2001;21(1):7–16. doi: 10.1177/0272989X0102100102. [DOI] [PubMed] [Google Scholar]
- 27.Bailey H, Kind P. Preliminary findings of an investigation into the relationship between national culture and EQ-5D value sets. Quality of Life Research. 2010;19(8):1145–1154. doi: 10.1007/s11136-010-9678-5. [DOI] [PubMed] [Google Scholar]
- 28.Busschbach JJ, Weijnen T, Nieuwenhuizen M, Oppe S, Badia X, Dolan P, et al. A comparison of EQ-5D time trade-off values obtained in Germany, the United Kingdom and Spain. In: Brooks R, Rabin R, de Charro F, et al., editors. The measurement and valuation of health status using EQ-5D: A European perspective. Dordrecht: Kluwer Academic; 2003. pp. 143–165. [Google Scholar]
- 29.Johnson JA, Luo N, Shaw JW, Kind P, Coons SJ. Valuations of EQ-5D health states. Are the United States and United Kingdom different? Medical Care. 2005;43(3):221–228. doi: 10.1097/00005650-200503000-00004. [DOI] [PubMed] [Google Scholar]
- 30.Kharroubi SA, O’Hagan A, Brazier JE. A comparison of United States and United Kingdom EQ-5D health state valuations using a nonparametric Bayesian method. Statistics in Medicine. 2010;29(15):1622–1634. doi: 10.1002/sim.3874. [DOI] [PubMed] [Google Scholar]
- 31.Nan L, Johnson JA, Shaw J, Coons SJ. A comparison of EQ-5D index scores derived from the US and UK population-based scoring functions. Medical Decision Making. 2007;27(3):321–326. doi: 10.1177/0272989X07300603. [DOI] [PubMed] [Google Scholar]
- 32.Norman R, Cronin P, Viney R, King M, Street D. International comparison in valuing EQ-5D health states: A review and analysis. Value in Health. 2009;12(8):1194–1200. doi: 10.1111/j.1524-4733.2009.00581.x. [DOI] [PubMed] [Google Scholar]
- 33.Gold MR, Siegel JE, Russell LB, Weinstein MC. Cost-effectiveness in health and medicine. New York: Oxford University Press; 1996. [Google Scholar]
- 34.Kind, P. (2009). Valuing EQ-5D health states—a VAStly simpler solution? In J. Busschbach, R. Rabin, & F. De Charro (Eds.), 24th scientific plenary meeting of the EuroQoL group—Proceedings, 2009 Sept 13–15; Kijkduin-The Hague, The Netherlands (pp. 319–337). Rotterdam: EuroQoL Group Executive Office.
- 35.Leidl R, Reitmeir P. A value set for the EQ-5D based on experienced health states. Development and testing for the German population. Pharmacoeconomics. 2011;29(6):521–534. doi: 10.2165/11538380-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 36.Rand-Hendriksen K, Augestad LA, Kristiansen IS, Stavem K. Comparison of hypothetical and experienced EQ-5D valuations: Relative weights of five dimensions. Quality of Life Research. 2012;21(6):1005–1012. doi: 10.1007/s11136-011-0016-3. [DOI] [PubMed] [Google Scholar]
- 37.Groot W. Adaptation and scale of reference bias in self-assessments of quality of life. Journal of Health Economics. 2000;19(3):403–420. doi: 10.1016/S0167-6296(99)00037-5. [DOI] [PubMed] [Google Scholar]
- 38.Menzel P, Dolan P, Richardson P, Olsen JA. The role of adaptation to disability and disease in health state valuation: A preliminary normative analysis. Social Science and Medicine. 2002;55(12):2149–2158. doi: 10.1016/S0277-9536(01)00358-6. [DOI] [PubMed] [Google Scholar]
- 39.Ubel PA, Loewenstein G, Jepson C. Whose quality of life? A commentary exploring discrepancy between health state evaluations of patients and the general public. Quality of Life Research. 2003;12(6):599–607. doi: 10.1023/A:1025119931010. [DOI] [PubMed] [Google Scholar]
- 40.National Institute for Health and Clinical Excellence (NICE). (2008). Guide to the methods of technology appraisal. London: National Institute for Health and Clinical Excellence: London, 23 June 2008. http://www.nice.org.uk/media/B52/A7/TAMethodsGuideUpdatedJune2008.pdf. Accessed 14 December 2012.
- 41.The Dental and Pharmaceutical Benefits Agency (TLV). (2003). General guidelines for economic evaluations from the Pharmaceutical Benefits Board (LFNAR 2003:2). Stockholm: The Dental and Pharmaceutical Benefits Agency. http://www.tlv.se/Upload/English/Guidelines-for-economic-evaluations-LFNAR-2003-2.pdf. Accessed 14 December 2012.
- 42.Torrance GW. Measurement of health state utilities for economic appraisal: A review. Journal of Health Economics. 1986;5(1):1–30. doi: 10.1016/0167-6296(86)90020-2. [DOI] [PubMed] [Google Scholar]
- 43.Bardage C, Isacson D, Ring L, Bingefors K. A Swedish population-based study on the relationship between the SF-36 and health utilities to measure health in hypertension. Blood Pressure. 2003;12(4):203–210. doi: 10.1080/08037050310002083. [DOI] [PubMed] [Google Scholar]
- 44.Lundberg L, Johannesson M, Isacson DGL, Borgquist L. Health-state utilities in a general population in relation to age, gender and socioeconomic factors. European Journal of Public Health. 1999;9(3):211–217. doi: 10.1093/eurpub/9.3.211. [DOI] [Google Scholar]
- 45.Williams, A. (1995). The measurement and valuation of health: A chronicle. Centre for Health Economics Discussion paper 136. York: University of York.
- 46.White A. A heteroscedasticity consistent covariance matrix estimator and a direct test of heteroscedasticity. Econometrica. 1980;48:817–838. doi: 10.2307/1912934. [DOI] [Google Scholar]
- 47.SAS Institute Inc. (2006). Base SAS®9.2. Procedures Guide (Second Ed, Vols. 1, 2, 3 and 4. Cary, NC: SAS Institute Inc.
- 48.Björk S, Norinder A. The weighting exercise for the Swedish version of the EuroQol. Health Economics. 1999;8(2):117–126. doi: 10.1002/(SICI)1099-1050(199903)8:2<117::AID-HEC402>3.0.CO;2-A. [DOI] [PubMed] [Google Scholar]
- 49.Greiner W, Claes C, Busschbach JJV, Graf van der Schulenburg JM. Validating the EQ-5D with time trade-off for the German population. European Journal of Health Economics. 2005;6(2):124–130. doi: 10.1007/s10198-004-0264-z. [DOI] [PubMed] [Google Scholar]
- 50.Lamers LM, McDonnell J, Stalmeier PFM, Krabbe PFM, Busschbach JJV. The Dutch tariff: results and arguments for an effective design for national EQ-5D valuation studies. Health Economics. 2006;15(10):1121–1132. doi: 10.1002/hec.1124. [DOI] [PubMed] [Google Scholar]
- 51.Tongsiri S, Cairns J. Estimating population-based values for EQ-5D health states in Thailand. Value in Health. 2011;14(8):1142–1145. doi: 10.1016/j.jval.2011.06.005. [DOI] [PubMed] [Google Scholar]
- 52.Badia X, Roset M, Herdman M. Inkonsistent responses in the three preference-elicitation methods for health states. Social Science and Medicine. 1999;49:943–950. doi: 10.1016/S0277-9536(99)00182-3. [DOI] [PubMed] [Google Scholar]
- 53.Wittrup-Jensen KU, Lauridsen J, Gudex C, Pedersen KM. Generation of a Danish TTO value set for EQ-5D health states. Scandinavian Journal of Public Health. 2009;37(5):459–466. doi: 10.1177/1403494809105287. [DOI] [PubMed] [Google Scholar]
- 54.Polsky D, Wilke RJ, Scott K, Schulman KA, Glick H. A comparison of scoring weights for EuroQol derived from patients and the general public. Health Economics. 2001;10(1):27–37. doi: 10.1002/1099-1050(200101)10:1<27::AID-HEC561>3.0.CO;2-R. [DOI] [PubMed] [Google Scholar]
- 55.Zethraeus N, Johannesson M. A comparison of patient and social tariff values derived from the time trade-off method. Health Economics. 1999;8(6):541–545. doi: 10.1002/(SICI)1099-1050(199909)8:6<541::AID-HEC464>3.0.CO;2-8. [DOI] [PubMed] [Google Scholar]
- 56.Björk, S., & Althin, R. (1991). Health states considered worse than being dead. In S. Björk (Ed.), EuroQol Conference Proceedings, IHE Working paper, 1991 Sept, Lund, Sweden (pp. 83–86). Lund: The Swedish Institute for Health Economics (IHE).
- 57.Macran S, Kind P. ‘Death’ and the valuation of health-related quality of life. Medical Care. 2001;39(3):217–227. doi: 10.1097/00005650-200103000-00003. [DOI] [PubMed] [Google Scholar]
- 58.Burström K, Johannesson M, Diderichsen F. Swedish population health-related quality of life using the EQ-5D. Quality of Life Research. 2001;10(7):621–635. doi: 10.1023/A:1013171831202. [DOI] [PubMed] [Google Scholar]
- 59.van Doorslaer E, Jones AM. Inequalities in self-reported health: Validation of a new approach to measurement. Journal of Health Economics. 2003;22(1):61–87. doi: 10.1016/S0167-6296(02)00080-2. [DOI] [PubMed] [Google Scholar]
- 60.Lundberg L, Johannesson M, Isacson DGL, Borgquist L. The relationship between health state utilities and the SF-36 in a general population. Medical Decision Making. 1999;19(2):128–140. doi: 10.1177/0272989X9901900203. [DOI] [PubMed] [Google Scholar]
- 61.Dolan P. NICE should value real experiences over hypothetical opinions. Nature. 2009;462(7269):35. doi: 10.1038/462035a. [DOI] [PubMed] [Google Scholar]
- 62.Leidl R, Reitmeir P, König HH, Stark R. The performance of a value set for the EQ-5D based on experienced health states in patients with inflammatory bowel disease. Value in Health. 2012;15(1):151–157. doi: 10.1016/j.jval.2011.08.004. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.