

Abstract
Objective
The aims of our study were to measure the learning style preferences of chiropractic students and to assess whether they differ across the 5 years of chiropractic study.
Methods
A total of 407 (41.4% females) full-degree, undergraduate, and postgraduate students enrolled in an Australian chiropractic program agreed to participate in a cross-sectional survey comprised of basic demographic information and the Visual, Aural, Read/Write, Kinesthetic (VARK) questionnaire, which identifies learning preferences on four different subscales: visual, aural, reading/writing, and kinesthetic. Multivariate analysis of variance and the χ2 test were used to check for differences in continuous (VARK scores) and categorical (VARK category preference) outcome variables.
Results
The majority of chiropractic students (56.0%) were found to be multimodal learners. Compared to the other learning styles preferences, kinesthetic learning was preferred by a significantly greater proportion of students (65.4%, p < .001) and received a significantly greater mean VARK score (5.66 ± 2.47, p < .001).
Conclusions
To the best of our knowledge, this is the first time chiropractic students have been shown to be largely multimodal learners with a preference for kinesthetic learning. While this knowledge may be beneficial in the structuring of future curricula, more thorough research must be conducted to show any beneficial relationship between learning style preferences and teaching methods.
Key Indexing Terms: Chiropractic, Education, Learning
INTRODUCTION
Learning style is described as the habitual manner in which a student gathers, processes, interprets, organizes, and thinks about material or gains skills.1,2 It is postulated that the compatibility between a student's learning style and the delivery of information is conducive for understanding, processing, and retaining information.3,4
The tools used to measure learning styles are based on four major models: personality (how the personality affects learning), information processing (which predominant sensory modality is used to take in and process information), social interaction (how the student interacts socially), and instructional preferences (how knowledge is best acquired).1 Within these broad models, many tests are available to measure learning style; for example, the inventory of learning styles by Entwistle,5 the Kolb Learning Style Inventory (LSI),6 the Learning Preferences Inventory (LPI),7 the Honey and Mumford Learning Style Questionnaire (LSQ),8 the Learning and Study Strategies Inventory (LASSI),9 and the Learning Styles Profiler (LSP),10 to name but a few.
The Visual, Aural, Read/Write, Kinesthetic (VARK) inventory, which is a tool based on the information-processing model, generates a profile of how an individual prefers to take in information, thereby providing a basis for assisting students to reflect on learning modal preferences.11,12 It was developed from the literature on neurolinguistic programming by Neil Fleming, an educator based at Lincoln University in New Zealand, and Charles Bonwell, a US teaching consultant (see the report of Fleming and Mills11). VARK is an acronym for four modalities that people use to perceive information: “Visual,” which shows a liking for information in graphs, charts and flow diagrams and symbol usage; “Aural,” which is a need to learn by ear and in social groups; “Read/Write,” which is a need to access information from written material; and “Kinesthetic,” which is preference for learning via senses, such as touch, hearing, smell, taste, and sight. Individuals with a preference for the latter category prefer concrete real world applications to understand material, including quite conceptual and abstract information, and, thus, respond to problem solving teaching.13
There is very limited research that specifically addresses chiropractic students and their learning styles. Moreover, these studies invariably have used LASSI with the intention of elucidating the potential relationship between learning styles and exam outcomes.14–16 Our objective was different, however, in profiling learning preferences with a view to informing teaching methods in the chiropractic curriculum. Therefore, we wanted to use a metric that would allow us to compare the learning styles of our chiropractic students to the literature on medical and allied students. Furthermore, we also were interested in elucidating whether there were any differences in learning preference among students at the different stages in our chiropractic program. The VARK inventory was considered to serve our purposes, because it is free to use (with permission from its copyright holder), quick and easy to administer, and affords many opportunities for comparison, since it has been used widely.
The primary purposes of this study were to measure the learning styles of chiropractic students and to assess whether the learning styles differ over the five-year course of chiropractic study. The secondary purpose was to compare the learning styles of chiropractic students to those of students in other medical and allied professions. The objective was to use this information to inform teaching methods in chiropractic curricula.
METHODS
Study Population and Sample
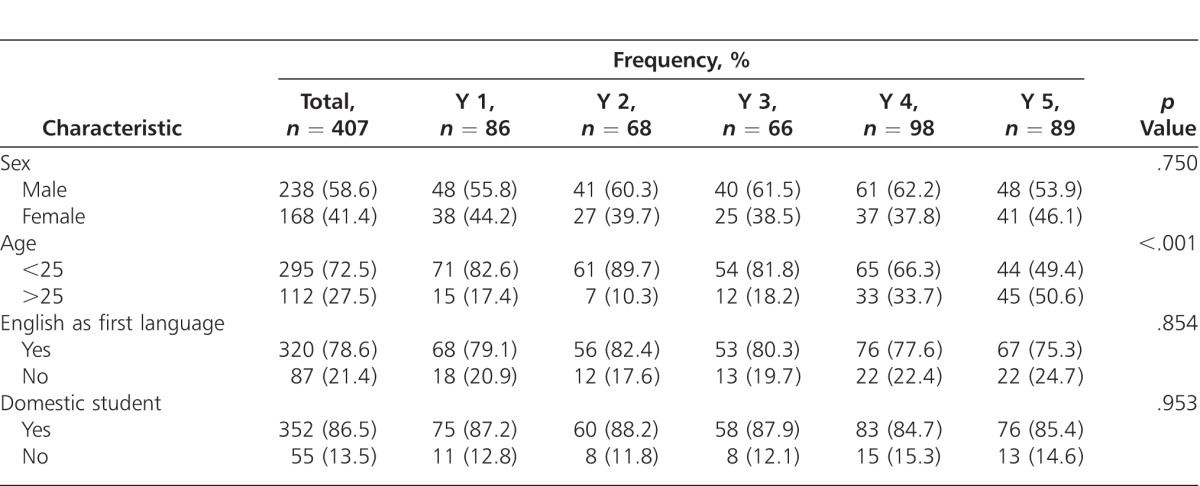
The chiropractic program at Macquarie University is divided into three years of full-time study at undergraduate level (years 1–3), for which the students are conferred the degree of bachelor of chiropractic science, and two years of full-time study at the postgraduate level (years 4 and 5), for which the students are conferred the degree of master of chiropractic, which qualifies them to practice as registered chiropractors. Unlike in North America, Australasian institutions do not confer doctor of chiropractic degrees. In addition to its undergraduate and postgraduate chiropractic degrees, Macquarie University offers a qualifying course (graduate diploma) designed to transition students with a related undergraduate degree into the postgraduate chiropractic course. Full-degree undergraduate and postgraduate students, but not qualifying course students, enrolled in the chiropractic program at Macquarie University in 2012 were invited to participate in this study. Of the 614 enrolled undergraduate and postgraduate students, a total of 407 students (41.4% females) agreed to complete the survey; thus, the response rate was 66.3%. Table 1 provides an overview of the frequency distribution of demographic variables by year of study. Naturally, the proportion of students 25 years of age and older increased significantly throughout the 5 years of study (p < .001). There were no significant differences in the other demographic variables across the five years of study.
Table 1.
Overview of the Frequency Distribution (%) of Demographic Characteristics by Year of Study
Survey Instrument
The survey instrument comprised two sections: basic demographic information, such as sex, age, whether English was their first language, and whether they were enrolled as domestic or international students; and the VARK questionnaire, version 7.1,17 which consists of 16 items, each comprising a statement with four different options. For each item, the students were asked to select the option that best represented their preference. They were free to choose more than one option if they wanted to, or leave blank any question that did not apply to them. The VARK questionnaire responses were scored by the researchers according to the accompanying VARK questionnaire scoring chart. The scoring procedure generates a sum ranging from 0 to 16 (a greater score indicates a greater preference) for each of the four VARK categories (ie, Visual, Aural, Read/write, and Kinesthetic). An algorithm translates VARK category scores to VARK category preferences. Respondents may have a single (unimodal) preference profile, or a multimodal preference profile, which comprises those with a preference for two modes (bimodal), three modes (trimodal), or all four modes (panmodal). The validity and reliability of the VARK questionnaire has been tested, and is considered adequate for its intended purposes.18 Permission to use the VARK questionnaire, version 7.1 was obtained from its copyright holder.
Data Collection
The anonymous survey was administered in class at the beginning of Semester 2, and written informed consent was obtained from all volunteer participants. It took less than 10 minutes to complete the survey. All data were collected on hard copy and subsequently entered into an electronic spread sheet. Approval to conduct this study was obtained from the Macquarie University Human Research Ethics Committee.
Data Analysis
Cross-tabulations were used to describe the frequency distributions of demographic characteristics by year of study, and the Pearson's χ2 test was used to check for group differences. De-identified VARK category scores were processed by the VARK website administrator to ascertain the VARK category preferences and modal status of each survey respondent. Overall VARK category scores and VARK category preferences/modal status were presented as means with standard deviations (SD) and frequencies (%), respectively. An ANOVA was used to test for differences in overall VARK category scores, while the Pearson's χ2 test was used check for differences in overall VARK category preferences and modal status.
Differences in VARK category scores across the five years of study were tested first simultaneously using a multivariate analysis of variance (MANOVA), and subsequent univariate analyses (ANOVA) were undertaken if the MANOVA indicated statistical significance (p < .05). Pairwise comparisons using t-tests with Bonferroni adjustments were used to determine which years were significantly different from one another with respect to a specific dependent variable (ie, a single VARK category score). Cross-tabulations were used to describe the frequency distributions of VARK category preferences and modal status across the five years of study, and the Pearson's χ2 test was used to test for group differences. All statistical analyses were performed using the R statistical package, version 2.15.2 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Overall, the majority (n = 228, 56.0%) of chiropractic students were found to be multimodal learners. A significantly greater (p < .001) number of students indicated they had a preference for “Kinesthetic” learning (n = 266, 65.4%) compared to “Visual” (n = 206, 50.6%), “Aural” (n = 214, 52.6%), and “Read/Write” (n = 210, 51.6%). Figure 1 shows box plots of the VARK category scores. Of the four VARK categories, “Kinesthetic” received a significantly greater (p < .001) mean VARK category score (5.66 ± 2.47).
Figure 1.

Boxplots of VARK category scores for the entire cohort and for each year of study.
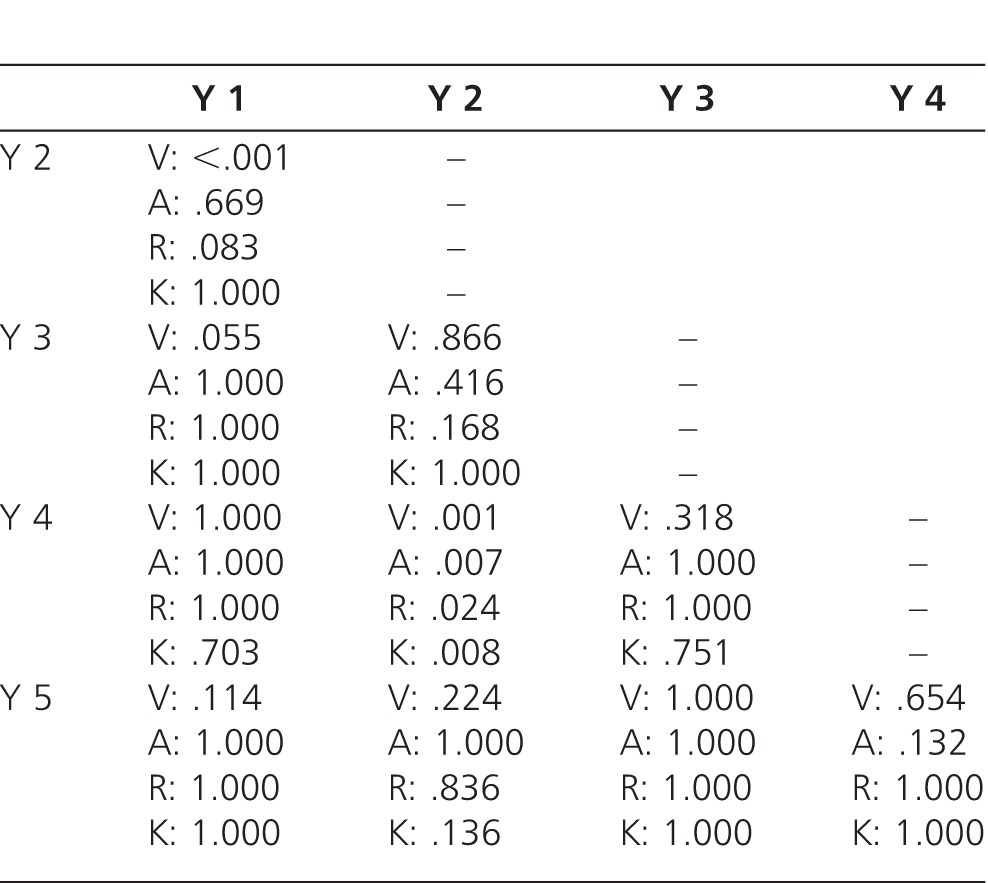
Table 2 provides an overview of the mean VARK category scores, and the frequency distributions of VARK category preference and modal status by year of study. Across the 5 years of study, there were no significant differences in the proportions of multimodal learners (p = .508); however, there were marginally significant differences in the number of students indicating a preference for “Visual” (p = .036) and “Read/Write” (p = .040). Figure 1 shows box plots of the VARK category scores by year of study. Of the four VARK categories, “Kinesthetic” received by and large a significantly greater mean score within each year of study. See Table 3 for a summary of p values from the pairwise comparisons of VARK category scores within each year of study. The MANOVA showed that there was a significant difference in VARK category scores across the years (p < .001), and the subsequent univariate ANOVAs revealed significant differences in mean scores for all VARK category scores (“Visual,” p < .001; “Aural,” p = .011; “Read/Write,” p = .025; and “Kinesthetic,” p = .015). Pairwise comparisons revealed that the significant MANOVA and ANOVA findings by and large could be attributed to significant differences between years 2 and 4. See Table 4 for a summary of p values from the pairwise comparisons of VARK category scores across the years of study.
Table 2.
Overview of Mean VARK Category Scores with Standard Deviations (SD), and Frequencies (%) of VARK Category Preferences and Modal Status by Year of Study
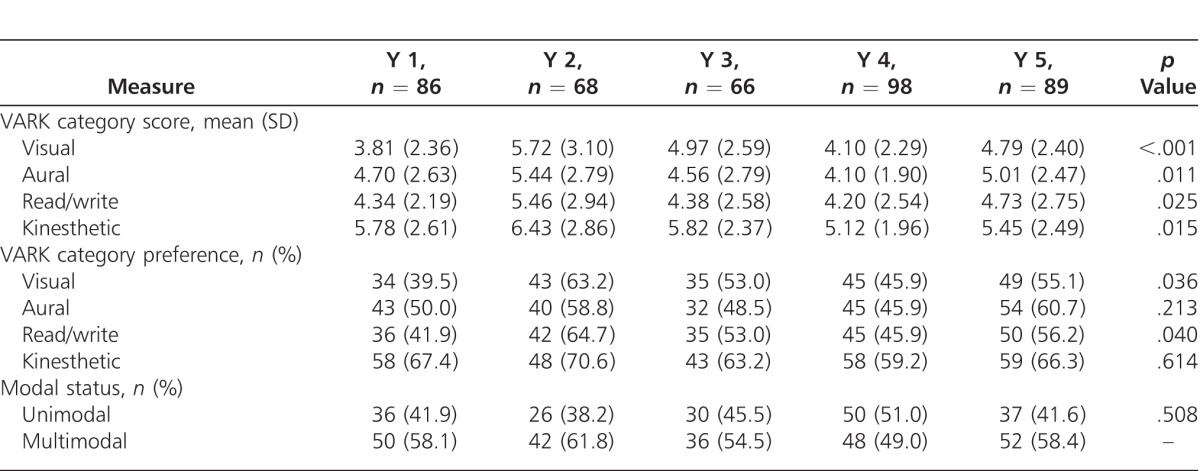
Table 3.
p Values From Pairwise Comparisons of VARK Category Scores Within Each Year of Study
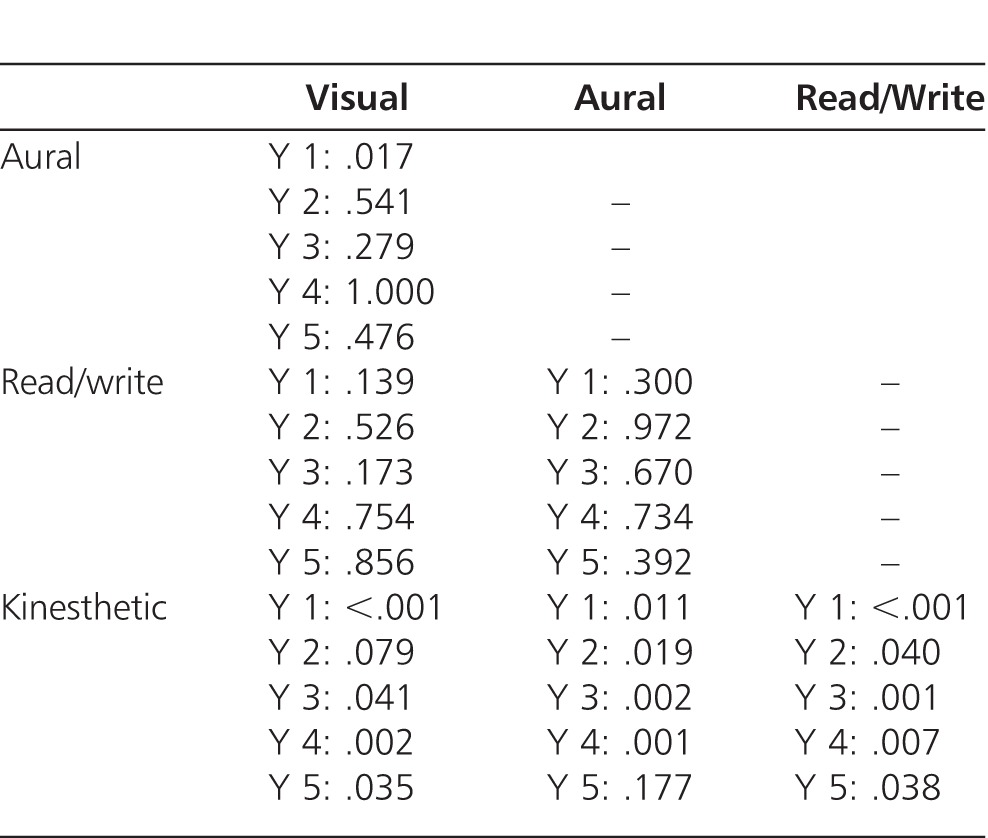
Table 4.
p Values From Pairwise Comparisons With Bonferroni Adjustment of VARK Category Scores Across the Five Years of Study
Because the proportion of students aged 25 years and older increased significantly throughout the five years of study, a post hoc MANOVA was undertaken to test simultaneously for differences in all VARK category scores by age group (under 25 vs 25 years and above). No differences were detected between the two age groups (p = .447), and, thus, subsequent ANOVAs of pairwise comparisons were undertaken.
DISCUSSION
The outcome of this study indicated not only that a higher percentage of our chiropractic students appear to have a kinesthetic learning preference, but also that this does not change over the course of study. It also indicated that they are highly multimodal in their approach to study, and this also does not change over the course of study. In actuality, the preference for kinesthetic learning is found in the general public, but reaches statistical significance in the student cohort under investigation in our study. According to the VARK website, of the 45,826 respondents, 27.8% are kinesthetic, 27.4% read/write, 24.5% aural, and 20.5% visual.19 For more details, see data presented in Table 5 in the Research and Statistics section of the VARK website.19
Some speculation is required as to why kinesthetic learning is preferred by chiropractic students. One obvious suggestion would be that chiropractic is a very hands-on profession, which would appeal to kinesthetic learners, who, thus, would then remain motivated throughout their training. However, there are plausible alternate explanations. For example, the latest understanding of brain function is that multiple sensory inputs are integrated in the brain in any learning process and, so, the kinesthetic modality of learning sits very comfortably with this.20 Kinesthetic preference is learning via the senses, which includes touch, hearing, smell, taste, and sight. In fact, the idea that students can be classified according to the one sensory modality they use to learn and that they then should be taught according to their preferred learning style is considered a neuromyth by some, for this very reason.20,21 In addition to this, if students are multimodal in their approach to learning, the instructional strategy would be to provide a variety of learning experiences and assignments, rather than trying to teach in response to the predominant modality. Providing appropriate teaching modes with good effect in response to learning preference is a matter of great debate and requires further justification through appropriate research.22
The plausibility of the argument laid out thus far is complicated by the results of other studies. Several studies have investigated the VARK student preferences in medical and allied students, with mixed outcomes.23–29 For example, in a study on 228 dental students (mean age of 23.5 years), there was a strong preference for visual learning (4.1) and read/write styles (4.0), indicating the use of lecture slides, diagrams, notes, and presentations.23 Aural was only 3.2 and kinesthetic 1.7 in their student preferences. This is contrary to our findings. However, as with our students, 56% of their students were multimodal, which also was similar to the 58% found by Fleming19 in the respondents on the VARK database. In another study on Jordanian third year nursing students undertaking a maternal health course (97% were approximately 21 years old), Read/Write was preferred at 4.2 ± 1.8 with Kinesthetic second at 3.9 ± 1.6.24 It is difficult to account for these differences, which may relate to age, culture, or what is being studied, but there seems to be no clear consistency.
Some studies seem more in line with our findings. Turner et al25 identified the learning preferences of pediatric residents using VARK and the Kolb LSI. They showed a significant preference for kinesthetic learning (p < .01), which also was represented as an interactive learning style preference on the Kolb inventory (p < .01). Of the 50 residents, 90% were Kinesthetic, 76% Read/Write, 66% Aural, and 62% Visual, and 80% were multimodal. Meehan-Andrews26 also found the majority of first year nursing students were Kinesthetic, and 84% preferred a multimodal learning style, which included the Kinesthetic mode. This correlated with a majority (85.8%) of students who felt practical classes were useful at least most of the time. However, the majority of their students found three teaching strategies (lectures, tutorials, and practical classes) useful to their learning, which does suggest that they are not “one trick ponies” and relates back to the high percentage of their students who had a multimodal learning style. James et al27 repeated the findings by Meehan-Andrews26 in first year nursing students, with kinesthetic preferences highest at 7.34 ± 2.67, differing significantly from the other modes (p < .001) and aural lowest at 6.30 ± 2.66.
Very limited research specifically addresses chiropractic students and their learning styles. Currently, to our knowledge there are no studies that use the VARK questionnaire to analyze learning styles in the teaching of chiropractic. A few studies use LASSI to address learning style in chiropractic students.14–16 The LASSI tests skill (information processing, selecting main ideas, and test strategies), will (anxiety, attitude, and motivation), and self-regulation (concentration, self-testing, study aids, and time management).15 A pilot study by Schutz and Gallagher14 investigated the relationship between academic performance and LASSI scores. They found that the group of chiropractic students with the higher grade point average (GPA) scored higher on the LASSI also, indicating better attitudes to learning. Similarly, Pringle and Lee,16 who administered the LASSI to trimester-6 students at Texas Chiropractic College after completion of Part 1 of the National Chiropractic Board of Examiners (NBCE) exams, found a correlation between the exam scores and LASSI scores. Shutz et al15 conducted a similar study that showed some of the LASSI subtests were statistically significant predictors of NBCE exam results. However, as was mentioned in the introduction, there is limited utility in comparing these findings with our own, because we are looking at different criteria in the measurement of learning style and without the intention of comparing this to exam outcomes.
The justification for using these results to modify how the curriculum should be taught is fraught with difficulty. Coffield et al30 conducted a systematic and critical review of 13 learning style inventories. Their overriding conclusion about these and others like them is that they are simple self-report tests, and so we should be careful not to expect too much of them. Notwithstanding the problem of self-reporting (inability to view oneself objectively and wanting to give socially desirable responses, for example) some questionnaires force respondents to agree or disagree with items that can act to constrain them into a predetermined format, and in addition there is difficulty in understanding the meaning intended by the original author of the questionnaire or, for that matter, of the respondent. They advise against basing pedagogic interventions on these learning style instruments. There are investigators who go further than Coffield et al30 and, in their review and meta-analysis of studies on the structural relevance of learning styles, have concluded there is insufficient evidence to use learning style assessment in educational practice, largely because its validity has not been tested adequately.31–34
However, it would be remiss not to speculate on the suitability of the course as it now is in the light of these findings. As Murphy et al23 have pointed out, the single most commonly used teaching modality is the lecture. This is a passive process that promotes rote learning, and is possibly more suitable for students with an aural preference. Testament to the ineffectiveness of this mode of delivery is the low attendance at lectures, although students do have the option to listen to the lectures online. Kinesthetic learners, one would think, are more suited to practical classes and tutorials, but these also are methods of delivery in the chiropractic course. In addition, given that many students are multimodal, and also that within each cohort there is a mix of preferences, it would seem that the varying learning preferences are being met.
To the best of our knowledge, this study is unique in using the VARK questionnaire to evaluate the learning preferences of chiropractic students. The results of this study revealed that a preference for the kinesthetic learning was seen in each of all five year groups. There are many possible reasons for the apparent lack of evolution of this preference, including the multimodal learning style of students, and how closely the kinesthetic style, as defined by its authors, fits our present understanding of the way the brain works. It also is likely that this result relates to teaching and assessment modalities in this course, which are varied and appeal to all categories of this model. It may well reflect the flexibility of the students and the course.
Limitations
The generalizability of the findings in this review may be limited because the study sample is comprised of chiropractic students from a single institution. For instance, it is conceivable that the learning style preferences of chiropractic students in other geographic or cultural settings may differ from that which has been reported in this study. Although the findings in this cross- sectional study suggested there are no important differences in learning style preferences across the five years of chiropractic study, the study design precludes any conclusions about whether the learning style preferences of individual chiropractic students actually change over the course of their studies. A prospective, longitudinal study design would be necessary to answer such questions conclusively.
CONCLUSION
The major finding from this study is that there is a high prevalence for a multimodal learning approach with an emphasis on a kinesthetic style of learning in chiropractic students across the five years of study. To the best of our knowledge, this is the first time this outcome has been shown in chiropractic students, and it adds to a body of research on the learning preferences of medical and allied professions that is quite contradictory. While this information may be beneficial in the structuring of future curriculum and execution of course outlines, more thorough research must be conducted to gain a greater insight into the relationship between learning style preferences and teaching methods.
ACKNOWLEDGMENTS
The authors thank Neil Fleming for processing the modal responses of the students, and express gratitude to the unit convenors in the chiropractic program at our institution for allowing time to conduct the research in their classes, and the students for participating in this study.
CONFLICTS OF INTEREST
The authors have no conflicts of interests to declare.
Footnotes
This article was received August 12, 2013, revised October 6, 2013, and accepted October 12, 2013.
REFERENCES
- 1.Marcy V. Adult learning styles: how the VARK© learning style inventory can be used to improve student learning. Perspect Physician Assist Educ. 2001;12(2):117–120. [Google Scholar]
- 2.Sadler-Smith E. “Learning styles” and instructional design. Innov Educ Train Int. 1996;33(4):185–193. [Google Scholar]
- 3.Fang AL. Utilization of learning styles in dental curriculum development. N Y State Dent J. 2002;68(8):34–38. [PubMed] [Google Scholar]
- 4.Zapalska AM, Dabb H. Learning styles. J Teach Int Bus. 2002;13:77–97. [Google Scholar]
- 5.Entwhistle NJ. Styles of Learning and Teaching: An Integrated Outline of Educational Psychology for Students, Teachers and Lecturers. New York, NY: John Wiley & Sons;; 1981. [Google Scholar]
- 6.Lynch TG, Woelf NN, Steele DJ, et al. Learning style influences student examination performance. Am J Surg. 1998;176(1):62–66. doi: 10.1016/s0002-9610(98)00107-x. [DOI] [PubMed] [Google Scholar]
- 7.Rezler A, Rezmovic V. The Learning Preference Inventory. J Allied Health. 1981;10:28–34. [PubMed] [Google Scholar]
- 8.Lesmes-Anel J, Robinson G, Moody S. Learning preferences and learning styles: a study of Wessex general practice registrars. Br J Gen Pract. 2001;51(468):559–564. [PMC free article] [PubMed] [Google Scholar]
- 9.Weinstein CE, Schulte A, Palmer DR. In: The Learning and Study Strategies Inventory. Publishing; H, editor. Clearwater, FL: H: 1987. [Google Scholar]
- 10.O'Connor PJ, Jackson CJ. The factor structure and validity of the Learning Styles Profiler (LSP) Eur J Psychol Assess. 2008;24(2):117–123. [Google Scholar]
- 11.Fleming ND, Mills C. Not another inventory, rather a catalyst for reflection. To Improve Acad Resource Fac Instructional Organ Dev. 1992;11:137–149. [Google Scholar]
- 12.VARK a guide to learning styles. 2013 Frequently asked questions. Available from: http://www.vark-learn.com/english/page.asp?p=faq. Christchurch, New Zealand: Neil Fleming; c2001–2013. Cited August 1. [Google Scholar]
- 13.Fleming ND. I'm different; not dumb. Modes of presentation (VARK) in the tertiary classroom. Zelmer ACL, Zelmer A, Chiou A, editors. Higher Education: Blending Tradition and Technology. Proceedings of the 1995 Annual Conference of the Higher Education and Research Development Society of Australasia (HERDSA) Sydney, Australia: Higher Education and Research Development Society of Australasia; 1995:308–313. In: eds. [Google Scholar]
- 14.Schutz CM, Gallagher BS, Tepe RE. Differences in Learning and Study Strategies Inventory scores between chiropractic students with lower and higher grade point averages. J Chiropr Educ. 2011;25(1):5–10. doi: 10.7899/1042-5055-25.1.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Schutz CM, Dalton L, Tepe RE. Learning and Study Strategies Inventory subtests and factors as predictors of National Board of Chiropractic Examiners Part 1 examination performance. J Chiropr Educ. 2013;27(1):5–10. doi: 10.7899/JCE-D-12-012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Pringle RK, Lee J. The use of Learning and Study Strategies Inventory (LASSI) as a predictor for success or failure on part I of the National Board of Chiropractic Examiners Test. J Manipulative Physiol Ther. 1998;21(3):164–166. [PubMed] [Google Scholar]
- 17.VARK a guide to learning styles. The VARK. 2013 Questionnaire available from: http://www.vark-learn.com/english/page.asp?p=questionnaire. Christchurch, New Zealand: Neil Fleming; c2001–2013. Cited August 1. [Google Scholar]
- 18.Leite WL, Svinicki M, Shi Y. Attempted validation of the scores of the VARK: learning styles inventory with multitrait-multimethod confirmatory factor analysis models. Educ Psychol Meas. 2010;70:323–339. [Google Scholar]
- 19.VARK® a guide to learning styles. Research & Statistics. 2013 Available from: http://www.vark-learn.com/english/page.asp?p=research. Christchurch, New Zealand: Neil Fleming; c2001–2013. Cited August 1. [Google Scholar]
- 20.Geake J. Neuromythologies in education. Educ Res. 2008;50(2):123–133. [Google Scholar]
- 21.Dekker S, Lee NC, Howard-Jones P, et al. Neuromyths in education: prevalence and predictors of misconceptions among teachers. Front Psychol. 2012;3(429):1–8. doi: 10.3389/fpsyg.2012.00429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Wilson M. Students' learning style preferences and teachers' instructional strategies: correlations between matched styles and academic achievement. SRATE J. 2012;22(1):36–44. [Google Scholar]
- 23.Murphy RJ, Gray SA, Straja SR, et al. Student learning preferences and teaching implications. J Dent Educ. 2004;68:859–866. [PubMed] [Google Scholar]
- 24.Alkhasawneh IM, Mrayyan MT, Docherty C, et al. Problem-based learning (PBL): assessing students' learning preferences using VARK. Nurse Educ Today. 2008;28:572–579. doi: 10.1016/j.nedt.2007.09.012. [DOI] [PubMed] [Google Scholar]
- 25.Turner DA, Narayan AP, Whicker SA, et al. Do pediatric residents prefer interactive learning? Educational challenges in the duty hours era. Med Teach. 2011;33(6):494–496. doi: 10.3109/0142159X.2010.542524. [DOI] [PubMed] [Google Scholar]
- 26.Meehan-Andrews TA. Teaching mode efficiency and learning preferences of first year nursing students. Nurse Educ Today. 2009;29:24–32. doi: 10.1016/j.nedt.2008.06.007. [DOI] [PubMed] [Google Scholar]
- 27.James S, D'Amore A, Thomas T. Learning preferences of first year nursing and midwifery students: utilising VARK. Nurse Educ Today. 2011;31(4):417–423. doi: 10.1016/j.nedt.2010.08.008. [DOI] [PubMed] [Google Scholar]
- 28.Dobson JL. A comparison between learning style preferences and sex, status, and course performance. Adv Physiol Educ. 2010;34(4):197–204. doi: 10.1152/advan.00078.2010. [DOI] [PubMed] [Google Scholar]
- 29.Lujan H, DiCarlo S. First-year medical students prefer multiple learning styles. Adv Physiol Educ. 2006;30(1):13–16. doi: 10.1152/advan.00045.2005. [DOI] [PubMed] [Google Scholar]
- 30.Coffield F, Moseley D, Hall E, et al. Learning Styles and Pedagogy in Post-16 Learning: A Systematic and Critical Review. London, UK: Learning and Skills Research Centre;; 2004. [Google Scholar]
- 31.Landrum TJ, McDuffie KA. Learning styles in the age of differentiated instruction. Exceptionality. 2010;18:6–17. [Google Scholar]
- 32.Pashler H, McDaniel M, Rohrer D, et al. Learning styles: concepts and evidence. Psychol Sci Public Interest. 2009;9:105–119. doi: 10.1111/j.1539-6053.2009.01038.x. [DOI] [PubMed] [Google Scholar]
- 33.Kratzig GP, Arbuthnott KD. Perceptual learning style and learning proficiency: a test of a hypothesis. J Educ Psychol. 2006;98(1):238–246. [Google Scholar]
- 34.Kavale K, Forness S. Substance over style: assessing the efficacy of modality testing and teaching. Except Child. 1987;54:228–239. [Google Scholar]