

Abstract
Introduction:
Expansion in road network, motorization, and urbanization in the country has been accompanied by a rise in road accidents leading to road traffic injuries (RTIs). Today RTIs are one of the leading causes of deaths, disabilities, and hospitalizations with severe socioeconomic costs across the world.
Objectives:
The following study analyses the:
Age and sex distribution of injured in road traffic accidents (RTAs).
Circumstances leading to RTA.
Pattern and severity of injuries sustained in RTAs cases.
Design:
Retrospective record-based study.
Materials and Methods:
The aim of this study was to audit retrospectively the circumstances, severity, and pattern of injury sustained by vehicle occupants presenting to the Saraswathi Institute of Medical Sciences (SIMS) hospital Hapur, for a period of one year. Data were collected using the case sheets of 347 patients from the medical records section of hospital and analyzed using SPSS computer software version 16.0. Results are interpreted in terms of percentage, mean, chi-square, and z-test.
Results:
The pattern and severity of injuries sustained by 347 vehicle occupants admitted to the emergency department of SIMS, Hapur were retrospectively documented. Male victims 258 (74.35%) were more commonly involved than females 89 (25.65%) and majority of victims 141 (40.63%) were in age group of 20-30 years. Urban victims 222 (64.00%) outnumbered rural. The most frequently injured body regions were the extremities 499 (53.54%), followed by maxillofacial180(19.31%).. Out of total 802 external injuries, the most common type of injury was lacerations 307 (38.28%), abrasions 306 (38.15%)and followed by bruises 154 (19.20%). Multiple external injuries were more common on upper limb 216 (26.93%), lower limbs 210 (26.18%) and face 170 (21.20%), while crush injuries were more predominently seen in both the limbs. While laceration were common on face 120 (38.83%). Injuries to the chest 19 (2.36%), abdomen13 (1.61%), and spine 11 (1.36%) were seen in roughy equal proprotion of victims. The bones on right side 55 (55.55%) were more commonly fractured which is statistically significant. Skull injuries were mostly found on frontal 77 (47.53%), followed by parietal bone 33 (20.37%), mostly on right side. Conclusion: RTAs constitute a major public health problem in our setting. Urgent preventive measures targeting at reducing the occurrence of RTAs are necessary to reduce the morbidity and mortality resulting from these injuries.
Keywords: Injury pattern, road traffic accidents road traffic injuries, victims
Introduction
Road traffic accidents (RTAs) is an issue of national concern, considering its magnitude and gravity and the consequent negative impacts on the economy, public health and the general welfare of the people. Road traffic injury (RTI) is major but neglected public health problem in both developing and developed countries. World Health Statistics 2008 cited in Global Status Report on Road Safety states that RTIs in 2004 were the 9th leading cause of death and at current rates by 2030 are expected to be the 5th leading cause of death, overtaking diabetes and Human immunodeficiency virus infection/acquired immunodeficiency syndrome.
According to the National Crime Record Bureau (2010), the number of vehicular accidents was 430600 resulting in 133938 deaths and 470600 injuries, thereby accounting for 37.2% of all accidental deaths due to unnatural causes.(1)
Road traffic crashes are a major cause of misery, disability, and death globally, with a disproportionate number occurring in developing countries.(2,3) It has been predicted that by 2020, RTIs will rank as high as third among causes of disability adjusted life years lost.(3,4,5)
Injuries related to RTAs contribute significantly to the number of trauma admissions at Medical College, taking out a significant number of lives and resources. We need to know more about the numbers and types of injuries and about the circumstances in which these injuries occur. This information will indicate just how serious the injury problem is and where, exactly, prevention measures are most urgently needed.
Materials and Methods
The study is a retrospective analysis of cases of RTAs victims admitted in Saraswathi Institute of Medical Sciences, Hapur (UP) during the period between Feb 2008 and Jan 2009 after getting ethical clearance. The information about the patients admitted as cases of RTAs were ascertained from the hospital records. Case sheets of RTAs victims from the medical records sections were read and the necessary details were sought in terms of age, sex, residence, season of accidents, place, alcohol intake, type and site of injury. The cases with incomplete details were not taken into consideration. The analysis is done by SPSS-16 and the results were interpreted in terms of percentage, mean, chi-square, and z-test. A total of 347 RTAs cases were studied and analyzed for the different variables.
The patients thought to be and not to be under the influence of alcohol was based on the clinical impression of the attending doctor, where possible by breath alcohol. Injury patterns were identified using case sheets and Medico Legal Certificates (MLC) of the patients who seek medical care in hospital.
For the purpose of this study, the pattern of injury was documented by dividing the body into body regions. Thoraco-spinal injuries were included with those of the thorax and those of the lumbar spine with the abdomen. The face was defined as that part of the head lying between the hairline and chin. Injuries of the shoulder and hip joint were included within the limb region.
By careful recording of the circumstances of the accident, the risk factors for serious injury could be identified. Descriptive statistics was used and statistical significance was tested for using the chi-square and z-test. All statistical procedures were performed on separate data collection sheet using SPSS.16 software and run under Microsoft® XP Windows®.
Results
Out of total patients under review, 347 patients treated for injuries sustained in RTAs were included in the study and analyzed.
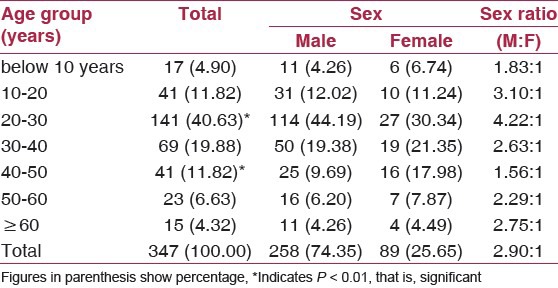
The distribution of study subjects according to the age and sex is depicted in Table 1. The patient's age ranged from 2 to 65 years with the mean age being 30.91 years. Out of total 347 victims, 258 (74.35%) were males, while only 89 (25.65%) were female subjects. Highest numbers of victims were in 20-30 years age group, accounting for 141 (40.63%) patients. On applying z-test, it is shown that age group 20-30 and 40-50 are statistically significant. Males are much more exposed to RTAs than females. Maximum sex differentiation was observed in age group of 20-30 years with male and female ratio of 4.22:1. While overall male and female ratio was 2.90:1.
Table 1.
Age and Sex-wise distribution of study subjects
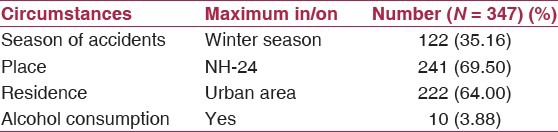
Various factors were attributed to the causation of these injuries as it is shown in Table 2 that maximum number of accidents took place during winter season (35.16%) and on national highway (69.50%). A total of 10 (3.88%) injured patients were intoxicated with alcohol at the time of accidents, all males.
Table 2.
Circumstances leading to accidents
The most common offender was two wheeler vehicles Regarding recorded causality by type of collision, four wheeler to heavy vehicle 66.15% was most common form among dozens of causes observed, followed by collision of two wheeler to four wheeler 44.44%. A significant relationship is observed between type of vehicle and collision between different vehicles [Table 3].
Table 3.
Recorded causality by type of collision
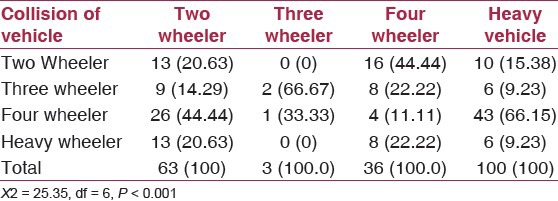
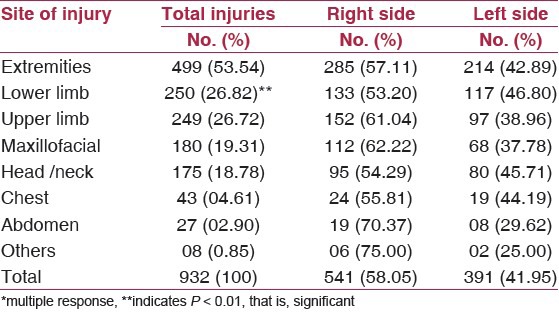
Table 4 showed that extremities 499 (53.54%) and the Maxillofacial injuries 180 (19.31%) were the most common body region injured. Head/neck were also more common and accounts for 175(18.78%) cases. The relatively low proportion of other injuries 08 (0.85%) is also noteworthy which includes missing tooth, amputation, burn, and genital injuries. Injuries are common on right side of body; this difference is statistically significant (P < 0.01) in lower limb.
Table 4.
Distribution of body regions injured in the accident (MR*)
Head injury was the commonest form of internal injuries seen in victims which was observed in 14 (2.30%) victims, showing clinical symptoms like unconsciousness, ENT bleed, vomiting, and nausea.
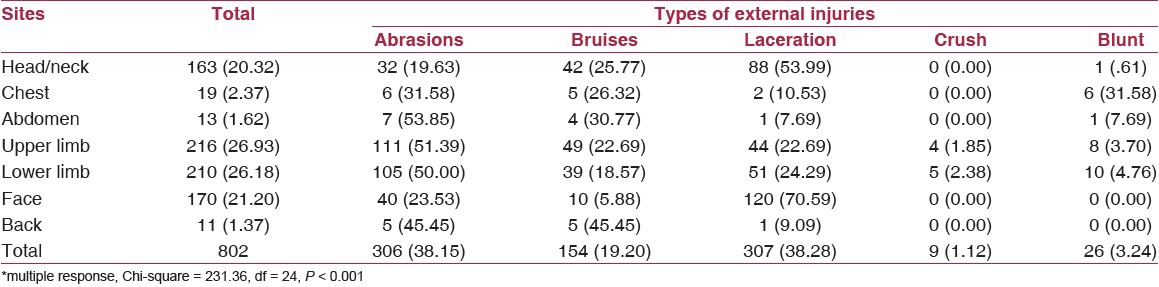
A detail analysis of various injuries on the body of victims revealed that out of total 802 external injuries seen in 347 victims, the most common pattern of injury was lacerations observed in 307 (38.28%), abrasions 306 (38.15%), followed by bruises 154 (19.20%) as shown in Table 5. The upper limb 216 (26.93%), lower limb 210 (26.18%), and head/neck 167 (20.32%) were the most common effected areas to suffer with external injuries seen in the victims. Upper limb 111 (51.39%), lower limb 105 (50.00%) and face 40 (23.53) were the most commonly involved by abrasion. While lacerations were common on face 120 (70.59%), head/neck 88 (53.99%), and upper limbs 44 (22.69%) and lower limbs 51 (24.29%). Multiple external injuries were more common on upper limbs 216(26.80%) and lower limbs 210 (26.05%) and head/neck 167 (20.72%) in that order, while crush injuries were more predominantly seen in both the limbs. Injuries to the chest 19 (2.37%), abdomen 13 (1.62%), and back 11 (1.37%) were seen in roughly equal proportion of victims.
Table 5.
External injuries among the victims (n = 347)*
As shown in Figure 1, the commonest site of fracture was the lower limbs 38 (38.00%), followed by upper limbs 34 (34.00%) and skull/maxillofacial bones 10 (10.00%). The less common sites were spine 5 (5.00%), and pelvis 2 (2.0%).
Figure 1.
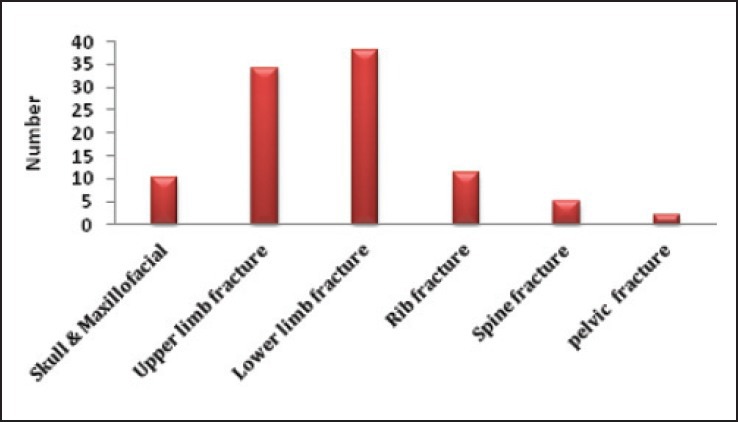
Site of fractures among the victims
The bones on right side 55 (55.55%) of body were more commonly fractured as compared to the left side. On applying chi-square test, a statistically significant difference is observed as shown in Table 6. In lower limb, fracture involved both the side equally 19 (50%). Next, common bones involved were of upper limb being fractured in 21 (61.76%) and 13 (38.24%) cases on right and left sides, respectively. A further analysis of these fractures indicate that skull and maxillofacial fractures involved in RTA were more on right side 7 (70.00%) as compared with 3 (30.00%) on left side [Table 7].
Table 6.
Distribution of fractures sustained in road traffic accident cases
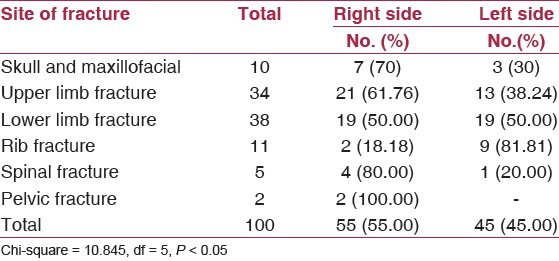
Table 7.
Skull injuries according to anatomical site due to road traffic accident
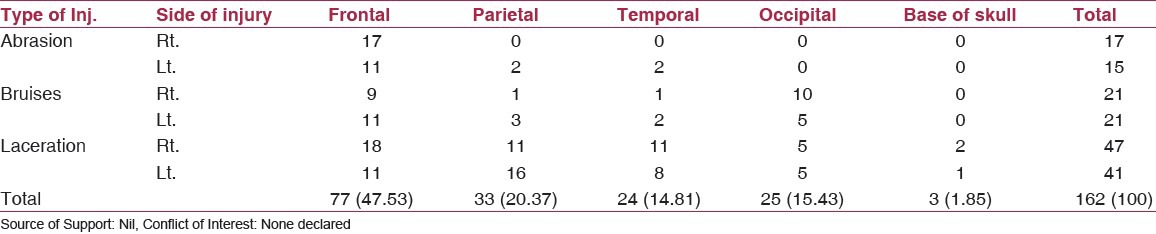
Out of total 162 injuries on skull, most common site was frontal 77 (47.53%), parietal 33 (20.37%), occipital 25 (15.43), and temporal bone 24 (14.81). Most of injuries were on right side of skull.
Skull injuries commonly involved laceration and bruises on the frontal and parietal bone. Laceration is more on right side of frontal, parietal, and temporal area. Base of skull showed very few external injuries [Figure 2].
Figure 2.
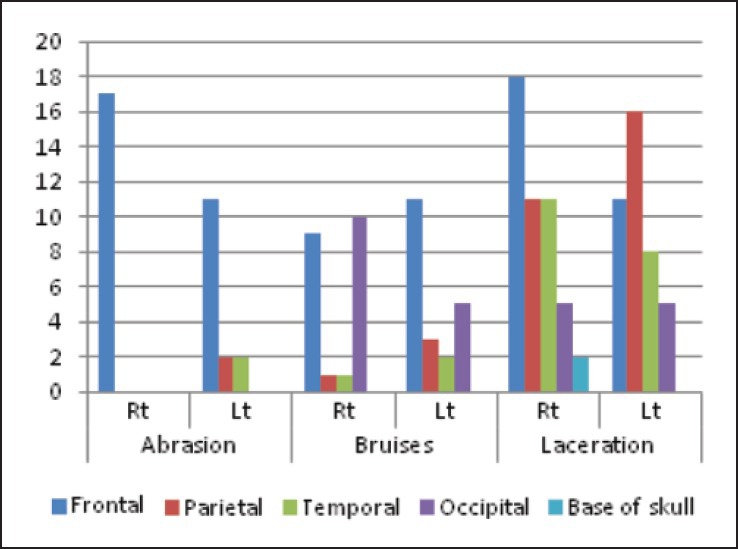
Skull injuries according to anatomical site due to road traffic accident
Discussion
RTAs constitute a major public health problem in all over the world. In this review, the majority of RTA victims were young in their most reproductive and productive years and showed a male preponderance.
The results of the present study revealed that 258 (74.35%) of the victims were males and the rest 89 (25.65%) were females. The highest number of victims 141 (40.63%) were from 20 to 30 years of age group. In males, the maximum numbers of cases were seen in the age group 20-30 years 114 (44.19%). The mean age of the RTA victim came out to be 30.91. Overall, male is to female ratio is 2.90:1. The reason for high incidence of RTAs in males reflects their high activity levels and participation in high-risk activities such as recklessness driving/riding, over-speeding and drunken driving without wearing any protective gears. It is due to greater male exposure on streets.(6,7,8,9) On the contrary, females are involved in various indoor activities mostly due to cultural background and extra precaution taken by family members to keep them safe. However, other studies observed that the peak age of male victims was in the 4th decade, with the mean at 33 years.(10,11)
Majority of these accidents occurred on the national highway 241 (69.50%). This can be explained on the fact that national highway-24 is the busiest roads with vehicles travelling at high speeds, the roads being less wider multiple intersections and divider cuts are present at every kilometer for changing the side.(12,13,14,15) Maximum number of cases (32.20%) was recorded in the winter months, which is in concurrence with others studies.(12,13,14)
In the present study, 10 (3.88%) of the male victims involved in RTA had consumed alcohol. This is a lower proportion than 4.6% and 8%, reported by others from Delhi.(8,16)
There was a higher rate of face, head, and neck injuries in the present study. A possible explanation might be that motor vehicle occupants did not use seat belts, resulting in forward jerk during a collision and higher rate of injury. Abrasions and lacerations were the commonest types of injuries among the external injuries noted in this study. Similar results were also observed by others researchers.(6,10) Common sites for injuries were the lower and upper limbs and face.(6,7)
Among fractures, present study found that the commonest site of fracture was the lower limb 38 (38.34%), followed by upper limb 34 (34.340%) and skull/maxillofacial 10 (10.10%). The more fractures on lower extremity is again due to interaction of gravitational force and velocity of the vehicle at the time of accidents.(6)
But in another study, it was reported that the highest number of fractures was in upper limbs followed by lower limbs and facial bones.(10) In contrast, result of other study showed that the commonest injury was fracture of bones particularly of the head and face and closely followed by the lower extremity.(17)
The present study also indicates that injuries and fractures were more common on right side in both upper and lower extremities.(18)
Conclusion
The result of this study enables a health care to predict fracture and site of injury. Strict enforcement of road safety regulations and improving emergency medical services may prevent untimely deaths and disabilities caused by RTAs.
Awareness campaigns concerning safety rules targeted at the high-risk groups and by improvement of the roads. The fact that the economically productive age-group were mostly involved an urgent public policy response with special reference to education, engineering, environment, and emergency care of road accident victims.
Limitation
The analysis of the details of the riders in vehicles was not possible due to insufficient information from the hospital record in relation to their seating, wearing of seat belt, and amount of alcohol consumption, and so on. The other limitations of this study were the extent of internal injury which was not analyzed up due to referral to higher centers.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.National Crime Record Bureau. Annual Report on Road Accidents. 2010 [Google Scholar]
- 2.Nantulya VM, Reich MR. The neglected epidemic: Road traffic injuries in developing countries. BMJ. 2002;324:1139–41. doi: 10.1136/bmj.324.7346.1139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lagarde E. Road traffic injury is an escalating burden in Africa and deserves proportionate research efforts. PLoS Med. 2007;4:e170. doi: 10.1371/journal.pmed.0040170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ghaffar A, Hyder AA, Masud TI. The burden of road traffic injuries in developing countries: The first national survey of Pakistan. Public Health. 2004;118:211–7. doi: 10.1016/j.puhe.2003.05.003. [DOI] [PubMed] [Google Scholar]
- 5.Museru LM, Leshabari MT. Road traffic accidents in Tanzania: A 10-year epidemiological appraisal. East Cent Afr J Surg. 2002;7:23–6. [Google Scholar]
- 6.Mehta SP. An epidemiological study of road traffic accident cases admitted in Safdarjang Hospital, New Delhi. Indian J Med Res. 1968;56:456–66. [PubMed] [Google Scholar]
- 7.Sathiyasekaran BW. Study of the injured and the pattern in road traffic accidents. Indian J Forensic Sci. 1991;5:63–8. [Google Scholar]
- 8.Ghosh PK. Epidemiological study of the victims of vehicular accidents in Delhi. J Indian Med Assoc. 1992;90:309–12. [PubMed] [Google Scholar]
- 9.Varghese M, Mohan D. New Delhi: Proceedings of the International Conference on Traffic Safety; 1991. Jan 27-30, Transportation injuries in rural Haryana, North India 1991. [Google Scholar]
- 10.Clark DW, Morton JH. The motorcycle accident: A growing problem. J Trauma. 1971;11:230–7. [PubMed] [Google Scholar]
- 11.Akang EE, Kuti MA, Osunkoya AO, Komolafe EO, Malomo AO, Shokunbi MT, et al. Pattern of fatal head injuries in Ibadan - A 10 year review. Med Sci Law. 2002;42:160–6. doi: 10.1177/002580240204200207. [DOI] [PubMed] [Google Scholar]
- 12.Kual A, Sinha US, Pathak YK, Singh A, Kapoor AK, Sharma S, et al. Fatal road traffic accidents, study of distribution, nature and type of injury. J Indian Acad Forensic Med. 2005;27:71–6. [Google Scholar]
- 13.Dhillon S, Kapila P, Sekhon HS. Pattern of injuries in road traffic accidents in Shimla hills. J Punjab Acad Forensic Med Toxicol. 2007;7:50–3. [Google Scholar]
- 14.Kumar PM, Ziya A, Prashant A, Yadav S, Chaturvedi R, Tripathi SK. Fatality due to chest injury in Road traffic accident victims of Varanasi and adjoining districts, U.P. Medico-Legal Update. 2006;6:7–9. [Google Scholar]
- 15.Singh H, Dhattarwal SK. Pattern and distribution of injuries in fatal road traffic accidents in Rohtak (Haryana) J Indian Acad Forensic Med. 2004;26:20–3. [Google Scholar]
- 16.Sood S. Survey of factors influencing injury among riders involved in motorized two wheelers accidents in India: A Prospective study of 302 cases. J Trauma. 1988;28:530–4. doi: 10.1097/00005373-198804000-00021. [DOI] [PubMed] [Google Scholar]
- 17.Wong TW, Phoon WO, Lee J, Yiu PC, Fung KP, Smith G, et al. Non-fatal injuries among motorcyclists treated as in-patients in a general hospital. Ann Acad Med Singapore. 1989;18:672–4. [PubMed] [Google Scholar]
- 18.Vijayamahantesh SN, Vijayanath VA. A Cross-sectional study: Pattern of injuries in non fatal road traffic accident cases in Bagalkot city of Karnatka. Int J Med Toxicol Forensic Medicine. 2012;2:27–32. [Google Scholar]