

Abstract
Angioleiomyoma is a benign tumor of vascular smooth muscle origin. Although many factors have been implicated in its pathogenesis, presence of lipometaplasia suggests its hamartomatous nature. This tumor presents as a painful nodular mass in extremities. Thus angioleiomyoma should be considered as a differential diagnosis of any solitary painful mass of forearm. Herein we report a case of 37-years-old female presenting with a slow growing mass in the right forearm. Histopathological and immunohistochemical examination confirmed the diagnosis of angioleiomyoma.
Keywords: Angioleiomyoma, forearm, immunohistochemistry, lipometaplasia
INTRODUCTION
Angioleiomyoma is an uncommon benign neoplasm arising from the vascular smooth muscle.[1] Histologically they have been classified into capillary or solid, cavernous, and venous.[2] Clinically most of them occur as painful nodular mass occurring in the extremities.[1,2] Here we present a case of subcutaneous angioleiomyoma occurring in the right forearm.
CASE REPORT
A 37-years-old female presented with a slowly enlarging mass in the right forearm since two years. She occasionally experienced pain and tenderness over the lesion. There was no history of trauma, and the patient was otherwise healthy.
On physical examination, an ovoid swelling measuring 1.5 × 1.5 × 1 cm was present on the right forearm. It was subcutaneous in plane and free from underlying bone. The lesion was smooth and firm. There were no skin changes and no signs of infection. There were no other masses and lymphadenopathy.
An excisional biopsy was done and sent for histopathological examination. The specimen, measuring 1.5 × 1.5 × 1 cm, was well encapsulated. On cut section it was gray white and solid. On examining the histopathological sections, many slits like vessels interspersed among spindled shaped tumor cells arranged in whorls and interlacing fascicles were revealed. The vessels were surrounded by an inner layer of muscle arranged circumferentially and outer layer blending with the less ordered tumor cells [Figure 1a]. Islands showing lipometaplasia were also observed among tumor cells [Figure 1b]. There was no evidence of nuclear atypia, mitosis, or necrosis. On immunohistochemistry, these tumor cells were diffusely positivity for Smooth Muscle Actin (SMA) [Figure 1c] and endothelial cells lining the vascular spaces were positive for CD34 [Figure 1d]. In view of the above histopathological and immunohistochemical findings, a diagnosis of solid variant of angioleiomyoma was made.
Figure 1.
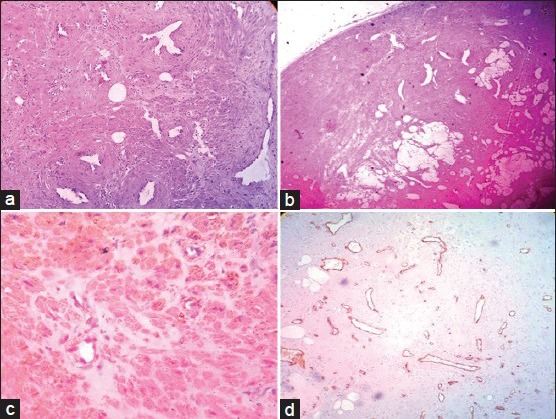
(a) Inner layer of muscle are arranged circumferentially around vessels and outer layer blends with less well-ordered smooth muscle tissue of tumor. (H and E, ×40) (b) Islands of lipometaplasia within the tumor. (H and E, ×40) (c) Diffuse cytoplasmic positivity present in tumor cells for smooth muscle actin. (×100) (d) CD34 positivity seen only in endothelial cell of vessel wall. (×40)
Post-operative period was uneventful with no evidence of recurrence.
DISCUSSION
Angioleiomyomas have been reported from several anatomical sites but are usually located in the subcutis and deep dermis of the extremities, more commonly in the lower limbs.[1,2] Lesions in the upper limbs are mainly located in the dorsal and palmar aspect of the hand, fingers, wrist, and forearms.[3] Other sites are head and neck region, and trunk of the body. It is more common in females and presents commonly between third and fifth decades of life.[2] Mechanism of development of angioleiomyoma remains obscure. While these tumors have been considered as vascular hamartomas, mechanical and hormonal factors have also been implicated in their pathogenesis.[2,4] In the present case, mature fat cells were demonstrated within the tumor, suggesting the hamartomatous nature of these tumors. Most of the cases present as solitary painful nodular mass less than 2 cm in diameter.[2] However, these are often painless in the head and neck region.[5] Although, the exact mechanism of pain remains unknown, it is thought to be associated with local ischemia caused by vascular contraction and making contact with the peripheral nerve fibres.[6]
Microscopically, this tumor is composed of smooth muscle cells with thick-walled blood vessels. They are classified into three subtypes: Capillary or solid, cavernous, and venous.[2] Tumors of the capillary type are composed of compact intersecting smooth-muscle bundles that surround these slit-like vessels. Dilated vascular channels are characteristics of cavernous type tumors. They have less smooth-muscle content and indistinct boundaries between the perivascular smooth-muscle bundles and the vessel walls. Tumors of venous type have distinct smooth-muscle vascular walls and less compact smooth-muscle bundles.[7] Immunohistochemical markers for smooth muscle cells such as SMA and vessel marker CD34 and CD31 are positive in angioleiomyoma.[8] Though these tumors are vascular, they bleed rarely probably because the feeding vessels are very small. In the present case, the tumor was excised without any significant bleeding. Angioleiomyomas do not recur if excision is complete.[1,8]
CONCLUSION
Angioleiomyoma is an uncommon tumor of the forearm, and it should be considered in the differential diagnosis of any solitary painful slow-growing nodular mass of the extremities.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Ramesh P, Annapureddy SR, Khan F, Sutaria PD. Angioleiomyoma: A clinical, pathological and radiological review. Int J Clin Pract. 2004;58:587–91. doi: 10.1111/j.1368-5031.2004.00085.x. [DOI] [PubMed] [Google Scholar]
- 2.Hachisuga T, Hashimoto H, Enjoji M. Angioleiomyoma. A clinicopathologic reappraisal of 562 cases. Cancer. 1984;54:126–30. doi: 10.1002/1097-0142(19840701)54:1<126::aid-cncr2820540125>3.0.co;2-f. [DOI] [PubMed] [Google Scholar]
- 3.Uchida M, Kojima T, Hirase Y, Iizuka T. Clinical characteristics of vascular leiomyoma of the upper extremity: Report of 11 cases. Br J Plast Surg. 1992;45:547–9. doi: 10.1016/0007-1226(92)90153-o. [DOI] [PubMed] [Google Scholar]
- 4.Hasey TC, Jacob T, Kaller H. Vascular leiomyoma. A case report and review of the literature. J Am Podiatry Assoc. 1984;74:93–5. doi: 10.7547/87507315-74-2-93. [DOI] [PubMed] [Google Scholar]
- 5.Wang CP, Change YL, Sheen TS. Vascular leiomyoma of the head and neck. Laryngoscope. 2004;114:661–5. doi: 10.1097/00005537-200404000-00012. [DOI] [PubMed] [Google Scholar]
- 6.Lawson GM, Salter DM, Hooper G. Angioleiomyomas of the hand: A report of 14 cases. J Hand Surg Br. 1995;20:479–83. doi: 10.1016/s0266-7681(05)80157-3. [DOI] [PubMed] [Google Scholar]
- 7.Morimoto N. Angiomyoma (vascular leiomyoma): A clinicopathologic study. Med J Kagoshima Univ. 1973;24:663–83. [Google Scholar]
- 8.Agarwal S, Gupta SK, Tejwani N. Angioleiomyoma of broad ligament. J Gynecol Endosc Surg. 2009;1:116–7. doi: 10.4103/0974-1216.71609. [DOI] [PMC free article] [PubMed] [Google Scholar]