

SUMMARY
The objectives of this study were: 1) study cochlea size variability among age and degree of deafness; 2) calculate the length of the cochlear implant electrode needed to obtain the optimal final insertion depth angle of 270°. A total of 241 patients (482 ears) that underwent high resolution computed tomography (HRCT) of the ear in our Institution between 2003 and 2008 were included to collect temporal bone data, and were divided in 3 groups: 97 (194 ears) patients with bilateral severe or profound sensorineural hearing loss (Group A), 70 patients (140 ears) with bilateral moderate sensorineural hearing loss (Group B), 74 patients (148 ears) without sensorineural or mixed hearing loss (Group C). In each of the 3 groups, 5 subgroups were identified with the following age criteria: 1) subgroup 1: subjects ≤5 years old; 2) subgroup 2: subjects 6-10 years old; 3) subgroup 3: patients 11-15 years old; 4) subgroup 4: patients 16-20 years old; 5) subgroup 5: subjects >; 20 years old. The length of the cochlea, height of the cochlea, basal turn lumen diameter (BTLD) and volume of the cochlea were measured. The Mann-Whitney test was used to assess the alternative hypothesis that a statistically significant difference in size exists between the different groups and subgroups. The following equation was adopted to calculate the length of a straight electrode which follows the outer wall of the scala tympani required to obtain the ideal insertion depth angle of 270°( LIC ):
. We found that the cochlea is completely developed and has reached adult size at birth. The degree of deafness does not affect the length or volume of the cochlea, while it can affect the height and BTLD. To assist the surgeon to calculate the ideal insertion depth angle of 270° in order to preserve residual hearing, it is useful to propose a straight electrode with 3 landmarks on the array (the first at 16.635 mm from the tip, the second at 17.987 mm and the third at 19.34 mm).
KEY WORDS: Cochlear implant, Cochlea size, Degree of deafness, Age, Length of cochlea, Height of cochlea, Basal turn lumen diameter, Volume of cochlea, Residual hearing preservation, Insertion depth angle
RIASSUNTO
Gli obbiettivi di questo studio sono stati: 1) lo studio della variabilità delle dimensioni cocleari in relazione all'età e al grado di ipoacusia; 2) calcolare la lunghezza dell'elettrodo dell'impianto cocleare richiesta per ottenere l'angolo ideale d'inserzione profonda di 270°. Per raccogliere i dati riguardanti le ossa temporali sono stati inclusi nello studio 241 pazienti (482 ossa temporali) che hanno ricevuto una Tomografia Computerizzata a alta risoluzione (HRCT) dell'orecchio nel nostro Policlinico Universitario tra il 2003 e il 2008; i pazienti sono stati divisi in 3 Gruppi: 97 (194 orecchie) aventi una ipoacusia neurosensoriale severa o profonda bilaterale (Gruppo A), 70 (140 orecchie) aventi una ipoacusia neurosensoriale moderata bilaterale (Gruppo B), 74 pazienti (148 orecchie) senza ipoacusia neurosensoriale o mista (gruppo C). In ciascuno dei 3 gruppi, sono stati identificati 5 sottogruppi in base all'età: 1) sottogruppo 1: soggetti ≤ 5 anni, 2) sottogruppo 2: soggetti da 6 a 10 anni; 3) sottogruppo 3: pazienti da 11 a 15 anni, 4) sottogruppo 4: pazienti da 16 a 20 anni, 5) sottogruppo 5: soggetti >; 20 anni. Sono stati misurati la lunghezza della coclea (L), l'altezza della coclea (H), il diametro del lume del giro basale (BTLD) e il Volume della coclea (V). Il Test di Mann-Whitney è stato utilizzato per verificare l'ipotesi alternativa che a livello di queste dimensioni esiste una differenza statisticamente significativa tra i differenti gruppi e sottogruppi. La seguente equazione è stata adottata per calcolare la Lunghezza di un elettrodo rettilineo che segue la parete esterna della scala timpani necessaria per ottenere l'angolo ideale di inserzione profonda di 270° (LIC):
. Secondo i nostri risultati alla nascita la coclea è completamente sviluppata e ha già raggiunto le dimensioni dell'adulto. Il Grado di ipoacusia non influenza la Lunghezza (L) e il Volume (V) della coclea, mentre può influenzare la sua altezza (H) e il diametro del lume del giro basale (BTLD). Per aiutare il chirurgo a ottenere l'angolo di inserzione profonda ideale di 270° nell'intento di preservare l'udito residuo sarebbe utile proporre un elettrodo rettilineo con 3 punti di riferimento: il primo a 16.635 mm dalla punta, il secondo a 17.987 mm, il terzo a 19,34 mm)
Introduction
By the middle of gestation, the cochlea is completely developed and has reached adult size: no further gain in size or change in shape is expected after birth 1-3. At present, there is anatomic 4 5 and radiological 6-16 evidence that the size of the cochlea presents some degree of variation between normal hearing subjects. Such evidence, on the one hand, prompted different authors to look radiologically for the existence of differences in cochlea size between normal hearing subjects and subjects with sensorineural hearing loss having a normal inner ear 7-11 16 17, and on the other hand have raised awareness regarding the cochlea size related variability of insertion depth angles for cochlear implant electrodes, making cochlear measurements and prediction of insertion depth angles for cochlear implant electrodes two important prerequisites to develop a next generation of implants that are more suited to cochlear size and therefore less traumatic 6 12.
The aims of the current study were: 1) study cochlea size variability considering age and degree of deafness in 3 groups of subjects: patients with bilateral severe or profound sensorineural hearing loss (group A), patients with bilateral moderate sensorineural hearing loss (group B), patients without sensorineural or mixed hearing loss (group C); 2) calculate the length of the cochlear implant electrode needed to obtain a final insertion depth angle of 270°, which in our opinion is the optimal insertion depth angle in the modern soft surgery era, since it allows to preserve most residual hearing without significant loss in hearing performances after cochlear implantation.
Methods
Patients
A total of 241 patients (482 ears) were included in this study to collect HRCT temporal bone data, and were divided in 3 groups: 97 (194 ears) patients with bilateral severe or profound sensorineural hearing loss (Group A), 70 patients (140 ears) with bilateral moderate sensorineural hearing loss (Group B), 74 patients (148 ears) without sensorineural or mixed hearing loss (Group C).
The 97 patients with bilateral severe or profound sensorineural hearing loss were selected between all patients who received a cochlear implant and had a preoperative HRCT in our institution between 2003 and 2008. The 70 patients with bilateral moderate sensorineural hearing loss were selected between all patients with bilateral moderate sensorineural hearing loss that received a hearing aid device who had been screened in our institution for middle and/or inner ear anomaly in the same period. The 74 patients without sensorineural or mixed hearing loss were selected between all patients with cholesteatoma scheduled for tympanoplasty who had a preoperative HRCT in our institution during the same period. The criteria for inclusion were: 1) HRCT performed in our institution and still available on the PACS; 2) slice thickness of 0.6 mm or less 3) radiologically undetectable abnormalities of the inner ear.
In each of the 3 groups, 5 subgroups were identified following age criteria: 1) subgroup 1: subjects ≤5 years old; 2) subgroup 2: subjects 6-10 years old; 3) subgroup 3: patients 11-15 years old; 4) subgroup 4: patients 16-20 years old; 5) subgroup 5: subjects >; 20 years old (Table I).
Table I.
Distribution of patients in the 3 groups among the age-related subgroups.
| Subgroup Group |
1 (<5 years-old) |
2 (6-10 years-old) |
3 (11-15 years-old) |
4 (16-20 years-old) |
5 (>;20 years- old) |
Total |
|---|---|---|---|---|---|---|
| A (bilateral severe or profound sensorineural hearing loss) | 24 | 7 | 5 | 5 | 57 | 97 |
| B (bilateral moderate sensorineural hearing loss) | 15 | 29 | 16 | 7 | 3 | 70 |
| C (no sensorineural or mixed hearing loss) | 2 | 11 | 14 | 10 | 37 | 74 |
Images processing
The images were treated with the Myrian® Expert 1.2 software developed by Intrasense® in order to obtain the following measures: 1) cochlear length (L); 2) cochlear height (H); 3) basal turn of cochlea lumen diameter (BTLD); 4) cochlear volume (V).
A view of the basal turn of the cochlea was developed as shown in Figure 1 to obtain L, H and BTLD, in accordance with the method described by Fraysse et al. [6]
Fig. 1.

Two-dimensional reconstruction from HRCT data of the basal turn of the cochlea using a 1.1 mm layer, minimum intensity projection. Distance L (cochlear length), here 8.4 mm, perpendicular distance H (cochlear height), here 6.1 mm, and distance BTLD (basal turn lumen diameter), here 1.9 mm, are measured using the scanner system.
The aim was to view the lateral wall from the round window to one full turn (360°). The entire basal turn cannot be viewed using a single two-dimensional plane and thus a reconstruction was performed using a 1.1 mm layer with minimum intensity projection. This layer captures the extremity of the cochlear canal and either the scala tympani or scala vestibuli. The viewing angle was adjusted with the aid of the perpendicular sections to obtain a view that gave the largest area of dark pixels. In one view, one can visualize round window, oval window, basal turn of the cochlea, vestibule and the anterior branches of the lateral and superior semicircular canals.
The view developed allowed the largest distance L from the inferior lip of the round window niche, through the modiolar axis, to the lateral wall and the perpendicular distance H to be measured as in Figure 1. The same view also allowed BTLD to be measured: it was arbitrarily decided to measure BTLD in the bisector of the second quarter of the cochlea as in Figure 1.
To measure the volume (V), the software required encompassing the limits of the cochlea in multiple contiguous axial slices. The accuracy of the measurement V was checked by visual inspection of the area obtained in the view of the basal turn of the cochlea developed to obtain the other measures and in the axial, coronal and sagittal view, as shown in Figure 2.
Fig. 2.

The accuracy of the manually defined volume was checked by visual inspection of the coloured area obtained in four planes: coronal (upper left), sagittal (upper right), axial (lower left) and reconstructed view (lower right). Cochlea should only be defined by the striped area.
Statistical analysis
The Mann-Whitney test was used to assess the alternative hypothesis that a statistically significant difference in size exists between the different groups and subgroups. The same test was used to assess the alternative hypothesis that a statistically significant difference in size exists between the left ear and the right ear.
CI array optimal length determination
According to Fraysse et al, [6] the following equation was adopted to calculate the length of a straight electrode which follows the outer wall of the scala tympani required to obtain the ideal insertion depth angle of 270° (LIC):
.
Results
Cochlear measurements in group A (bilateral severe or profound sensorineural hearing loss)
The median, mean, range and the standard deviation for each measurement in group A was, respectively:
cochlear length (L): 9 mm, 9.0623 mm, 7.4-11.4 mm, 0.7036 mm;
cochlear height (H): 6.9 mm, 6.9247 mm, 4.8-8.5 mm, 0.6101 mm;
Basal Turn Lumen Diameter (BTLD): 2.2 mm, 2.1814 mm, 1.5-2.8 mm, 0.2266 mm;
cochlear volume (V): 0.1415 ml, 0.1504 ml, 0.067- 1.112 ml, 0.0963 ml.
Table II summarizes the results of the cochlear measurements in group A.
Table II.
Cochlear measurement results in group A (bilateral severe or profound sensorineural hearing loss): length (L), height (H), basal turn lumen diameter (BTLD), volume (V).
| L (mm) | H (mm) | BTLD (mm) | V (ml) | |
|---|---|---|---|---|
| Mean | 9.0623 | 6.9247 | 2.1814 | 0.1504 |
| Median | 9 | 6.9 | 2.2 | 0.1415 |
| Min | 7.4 | 4.8 | 1.5 | 0.067 |
| Max | 11.4 | 8.5 | 2.8 | 1.112 |
| Range | 7.4-11.4 | 4.8-8.5 | 1.5-2.8 | 0.067-1.112 |
| Standard deviation | 0.7036 | 0.6101 | 0.2266 | 0.0963 |
Cochlear measurements in group B (bilateral moderate sensorineural hearing loss)
The median, mean, range and standard deviation for each measurement in group B was, respectively:
cochlear length (L): 8.95 mm, 8.9642 mm, 7.4-11 mm, 0.5481 mm;
cochlear height (H): 6.8 mm, 6.7678 mm, 5.3-7.7 mm, 0.4143 mm;
Basal Turn Lumen Diameter (BTLD): 2.1 mm, 2.1264 mm, 1.8-2.8 mm, 0.2306 mm;
cochlear volume (V): 0.1335 ml, 0.1460 ml, 0.094- 1.101 ml, 0.117 ml.
Table III summarizes the results of the cochlear measurements in group B.
Table. III.
Cochlear measurement results in group B (bilateral moderate sensorineural hearing loss): length (L), height (H), basal turn lumen diameter (BTLD), volume (V).
| L (mm) | H (mm) | BTLD (mm) | V (ml) | |
|---|---|---|---|---|
| Mean | 8.9642 | 6.7678 | 2.1264 | 0.1460 |
| Median | 8.95 | 6.8 | 2.1 | 0.1335 |
| Min | 7.4 | 5.3 | 1.8 | 0.094 |
| Max | 11 | 7.7 | 2.8 | 1.101 |
| Range | 7.4-11 | 5.3-7.7 | 1.8-2.8 | 0.094-1.101 |
| Standard deviation | 0.5481 | 0.4143 | 0.2306 | 0.1170 |
Cochlear measurements in group C (patients without sensorineural or mixed hearing loss)
The median, mean, range and standard deviation for each measure in group C was, respectively:
cochlear length (L): 9.1 mm, 9.125 mm, 7.7-11.9 mm, 0.6806 mm;
cochlear height (H): 6.85 mm, 6.8128 mm, 4.8-8.2 mm, 0.502 mm;
Basal Turn Lumen Diameter (BTLD): 2.2 mm, 2.2263 mm, 1.5-2.7 mm, 0.2322 mm;
cochlear volume (V): 0.152 ml, 0.1854 ml, 0.084-2.01 ml, 0.2309 ml.
Table IV summarizes the results of the cochlear measurements in group C.
Tab. IV.
Cochlear measurements results in group C (patients without sensorineural or mixed hearing loss): length (L), height (H), basal turn lumen diameter (BTLD), volume (V).
| L (mm) | H (mm) | BTLD (mm) | V (ml) | |
|---|---|---|---|---|
| Mean | 9.125 | 6.8128 | 2.2263 | 0.1854 |
| Median | 9.1 | 6.85 | 2.2 | 0.152 |
| Min | 7.7 | 4.8 | 1.5 | 0.084 |
| Max | 11.9 | 8.2 | 2.7 | 2.01 |
| Range | 7.7-11.9 | 4.8-8.2 | 1.5-2.7 | 0.084-2.01 |
| Standard deviation | 0.6806 | 0.502 | 0.2322 | 0.2309 |
Influence of the side on cochlear measurements
No statistical difference was found between the length (L), the height (H), BTLD and volume (V) of the right and left cochlea in any of the three groups (p >; 0.05).
Statistical analysis of the influence of age on cochlear size
In all groups, there was no increase in length (L), height (H), BTLD or volume (V) after birth (Figs. 3-5).
Fig. 3.

Group A (bilateral severe or profound sensorineural hearing loss): measurement obtained in left ear versus age for L, H, BTLD and V.
Fig. 5.

Group C (patients without sensorineural or mixed hearing loss): measurement obtained in left ear versus age for L, H, BTLD and V.
Fig. 4.

Group B (bilateral moderate sensorineural hearing loss): measurement obtained in left ear versus age for L, H, BTLD and V.
Statistical analysis of the influence of the degree of deafness on cochlear length (L), cochlear height (H), BTLD and cochlear volume (V)
No statistically significant difference was found between the L of the different groups (p >; 0.05) (Fig. 6). A statistically significant difference was found between the H in group A (bilateral severe or profound sensorineural hearing loss) and group B (bilateral moderate sensorineural hearing loss) (p ≤ 0.02308), although no statistically significant difference was found between the H of group A and group C (patients without sensorineural or mixed hearing loss) (p >; 0.05) or between the H of group B and group C (p >; 0.05) (Fig. 6).
Fig. 6.
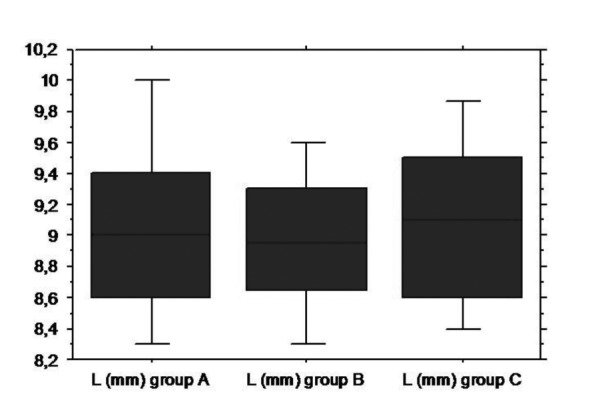

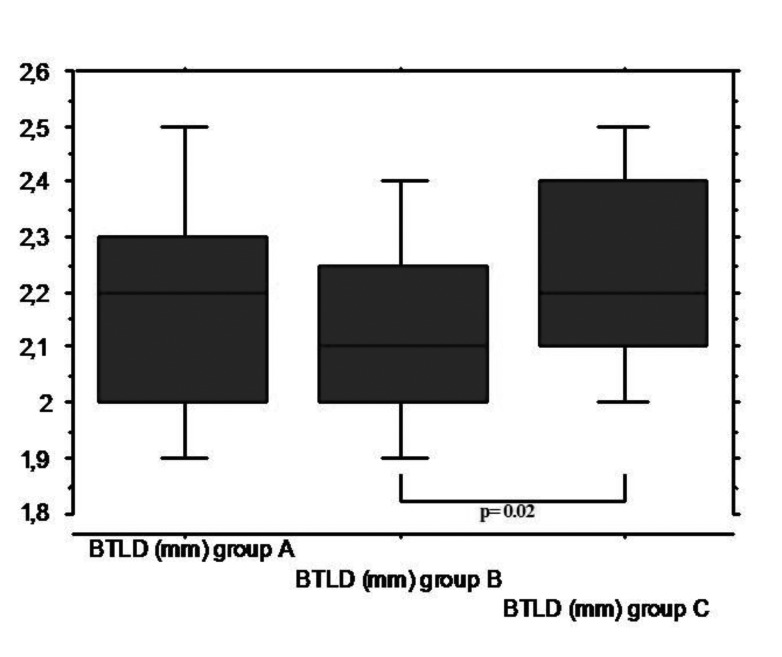
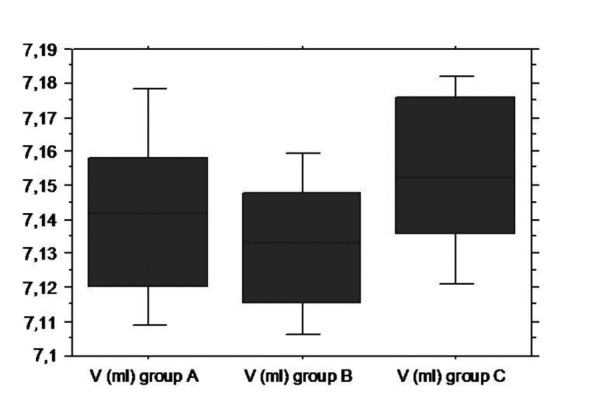
Box-plots illustrating the influence of the degree of deafness on the length of the cochlea (L) (upper-left), height of the cochlea (H) (upper-right), basal turn lumen diameter (BTLD) (lower-left) and volume of the cochlea (V) (lower-right). Group A: bilateral severe or profound sensorineural hearing loss; group B: bilateral moderate sensorineural hearing loss; group C: patients without sensorineural or mixed hearing loss.
A statistically significant difference was found between the BTLD of the group B (bilateral moderate sensorineural hearing loss) and group C (patients without sensorineural or mixed hearing loss) (p ≤ 0.02373), but no statistically significant difference was found between the BTLD of group A (bilateral severe or profound sensorineural hearing loss) and group B (p >; 0.05) or between the BTLD of group A and group C (p >; 0.05) (Fig. 6).
No statistically significant difference was found between the V between groups (p >; 0.05) (Fig. 6).
Statistical analysis of the influence of age in each group
We defined 5 age related subgroups for group to analyze the influence of age in each group: 1) subgroup 1: subjects ≤5 years old; 2) subgroup 2: subjects 6-10 years old; 3) subgroup 3: patients 11-15 years old; 4) subgroup 4: patients 16-20 years old; 5) subgroup 5: subjects >; 20 years old (tab 1). Comparing the L, H, BTLD and V of the different subgroups a statistically significant difference was found in in 2 cases:
H between subgroup A1 (48 ears) and subgroup B1 (30 ears) (p ≤ 0.02417);
H between subgroup A5 (112 ears) and subgroup C5 (74 ears) (p ≤ 0.03517).
Length of a straight electrode required to obtain the ideal insertion depth angle of 270° ( LIC)
The length of a straight electrode that follows the outer wall of the scala tympani required to obtain the ideal insertion depth angle of 270° (LIC ) was calculated for the cochlea of all groups (482 ears), and not just for the patients in group A, as no statistical difference was found between the L of the different groups. The mean, standard deviation and range of LIC we found was, respectively, 18.144 mm, 1.316 mm, 14.831-23.85 mm. The histogram in Figure 7 shows the distribution of LIC in the three groups. LIC ranged between 16.635 and 19.34 mm in more than 75% of inner ears.
Fig. 7.

Histogram illustrating the distribution of the calculated length of a straight electrode required to obtain the ideal insertion depth angle of 270° (LIC) in the subjects of all group.
Discussion
The current investigation was designed to study cochlea size variability considering age and degree of deafness in 3 groups of subjects, and assist in the conception of cochlear implants designed to preserve residual hearing by calculating the length of the straight (e.g. not preformed) cochlear implant electrode needed to obtain a final insertion depth angle of 270°.
The L and H obtained in the current investigation were similar to those obtained by Dimopoulos and Muren from 95 plastic casts 4 and to those obtained by Fraysse et al. from HRCT of 42 patients.6 The latter had already shown the L and H measurement method to be reliable at least to within the resolution of the HRCT scan 6.
The measurement of BTLD was similar to that obtained by Purcell et al. from the HRCT of 15 patients 7. The BTLD measurement method, different from the L and H measurement method, showed obvious limits related to the voxel resolution of the images, but a more accurate method is not possible with current technology.
The measure of V was not similar to that obtained by Kendi et al. from the MR of 29 healthy volunteers 18: in fact, we found a considerably higher mean value for V, but an obvious explanation can be suggested. We measured the volume of the anterior bony labyrinth on HRCT images, while Kendi et al. measured the volume of the anterior inner ear fluids on MR images, i.e. we obtained a measure of the container while Kendi et al. measured the content. Nonetheless, the V measurement method showed obvious limits related to the necessity of manually encompassing the limits of the cochlea in multiple axial slices and to the necessity of subjectively distinguishing the limit between the cochlea and other anatomical structures of the inner ear in multiple axial slices. This difficulty could represent another explanation for the discordance from results of Kendi along with the use of MRI. Also in the case of the V measurement method, a more accurate method is not possible with current technology. The interobserver variability was not calculated in the current investigation, but it was clearly felt that it is expected to be important for volume and especially for BTLD.
Our results confirm that cochlear size variability exists, and that this variability is not related to either age or side. The degree of deafness does not affect the length or volume of the cochlea, while it can affect height and the BTLD.
We found that the degree of deafness can affect the height of the cochlea, and the age-related subgroups analysis showed that this measure is also influenced by the age in each group. A statistically significant difference for H was found for the following:
between group A (bilateral severe or profound sensorineural hearing loss) and group B (bilateral moderate sensorineural hearing loss) (p ≤ 0.02308 ). The H of group B seems to be smaller;
between subgroup A1 (bilateral severe or profound sensorineural hearing loss, ≤ 5 years old) and subgroup B1 (bilateral moderate sensorineural hearing loss, ≤ 5 years old) (p ≤ 0.02417). The H of group B1 seems to be smaller;
between subgroup A5 (bilateral severe or profound sensorineural hearing loss, >; 20 years old ) and subgroup C5 (patients without sensorineural or mixed hearing loss, >; 20 years old) (p ≤ 0.03517). The H of group C5 seems to be smaller.
Interestingly, other authors have previously noted that the degree of deafness affects the height of the cochlea, even if they performed measurements of H on coronal or axial temporal bone CT, so that it is missing the real axis of the cochlea and underestimating H. Purcell et al. have suggested routine measurement of H on HRCT coronal images to improve the sensitivity of HRCT in detecting inner ear malformations when very subtle abnormalities are involved, and established a normative measurement to aid in the diagnosis of inner ear malformations (4.27 mm to 6.35 mm) 7. Moreover, performing measurements of the inner ear structures on axial temporal bone CT scans of 45 ears with congenital SNHL and grossly normal temporal bone CT scans and 45 ears with normal inner ear structures and normal hearing, Lan found that there were significant differences in the measurements of the maximal height of cochlea between the two groups (the maximal height of cochlea in the SNHL group was larger than the control group: 4.79 vs. 4.46 mm) 11.
The BTLD measurement method showed obvious limits related to the voxel resolution of images, thus making our results unreliable; however, we found a statistically significant difference between the BTLD of the 70 patients (140 ears) with bilateral moderate sensorineural hearing loss (Group B) and the BTLD of the 74 patients (148 ears) without sensorineural or mixed hearing loss (Group C). Interestingly, measuring BTLD on HRCT axial slice Purcell et al. found that the lumen of the basal turn in a group of 15 congenital SNHL with grossly normal temporal bone CT scans was smaller than the control group composed of 15 patients with normal hearing 8.
In the modern cochlear implantation era, there is growing interest in developing an atraumatic surgical technique designed to preserve cochlear function, minimize cochlear damage and allow easy, possibly repeated reimplantation 19-21. We used the data collected herein to optimize the length of the electrode array to preserve residual hearing by obtaining a final insertion depth angle of 270°. We calculated the length of a straight electrode which follows the outer wall of the scala tympani required to obtain the ideal insertion depth angle of 270° (LIC) for the cochlea of subjects in all groups (482 ears) and found that the mean LIC was 18.144 mm with a SD of 1.316 mm. LIC ranged from 16.635 to 19.34 mm in more than 75% of inner ears, so we propose to place 3 landmarks on the array, the first at 16.635 mm from the tip, the third at 19.34 mm, and the second between the first and the third, at 17.9875 mm.
These 3 landmarks could help to obtain a 270° insertion depth angle if preoperative measurement of cochlear length on HRCT has been performed, and could replace fluoroscopy. These conclusions only apply to straight electrodes that follow the outer wall of the scala tympani.
Conclusions
Cochlear size variability exists, and this variability is not age-related; the cochlea has already reached adult size at birth. The degree of deafness does affect the length or volume of the cochlea, while it can affect height and BTLD. In order to preserve residual hearing it seems reasonable to propose a straight electrode with 3 landmarks on the array (the first at 16.635 mm from the tip, the second at 17.987 mm, the third at 19.34 mm) to assist the surgeon in obtaining the ideal insertion depth angle of 270° when a preoperative measurement of cochlear length (L) by HRCT has been performed. These landmarks might be an alternative to fluoroscopy to assist array insertion, and could be an interesting subject for future research.
Acknowledgments
We acknowledge Intrasense® for making available Myrian ® Expert 1.2 software to obtain cochlear measurements.
References
- 1.Jackler RK, Luxford WM, House WF. Congenital malformations of the inner ear: a classification based on embryogenesis. Laryngoscope. 1987;97:2–14. doi: 10.1002/lary.5540971301. [DOI] [PubMed] [Google Scholar]
- 2.Pappas DG, Simpson LC, McKenzie RA, et al. High-resolution computed tomography: determination of the cause of pediatric sensorineural hearing loss. Laryngoscope. 1990;100:564–569. doi: 10.1288/00005537-199006000-00002. [DOI] [PubMed] [Google Scholar]
- 3.Nemzek WR, Brodie HA, Chong BW, et al. Imaging findings of the developing temporal bone in fetal specimens. AJNR Am J Neuroradiol. 1996;17:1467–1477. [PMC free article] [PubMed] [Google Scholar]
- 4.Dimopoulos P, Muren C. Anatomic variations of the cochlea and relations to other temporal bone structures. Acta Radiol. 1990;31:439–444. [PubMed] [Google Scholar]
- 5.Hardy M. The length of the organ of Corti in man. Am J Anat. 1938;62:291–311. [Google Scholar]
- 6.Escude B, James C, Deguine O, et al. The size of the cochlea and predictions of insertion depth angles for cochlear implant electrodes. Audiol Neurootol. 2006;11:27–33. doi: 10.1159/000095611. [DOI] [PubMed] [Google Scholar]
- 7.Purcell DD, Johnson J, Fischbein NJ, et al. Establishment of normative cochlear and vestibular measurements to aid in the diagnosis of inner ear malformations. Otolaryngol Head Neck Surg. 2003;128:78–87. doi: 10.1067/mhn.2003.51. [DOI] [PubMed] [Google Scholar]
- 8.Purcell DD, Fischbein NJ, Lalwani AK. Identification of previously "undetectable" abnormalities of the bony labyrinth with computed tomography measurement. Laryngoscope. 2003;113:1908–1911. doi: 10.1097/00005537-200311000-00009. [DOI] [PubMed] [Google Scholar]
- 9.Chen JL, Gittleman A, Barnes PD, et al. Utility of temporal bone computed tomographic measurements in the evaluation of inner ear malformations. Arch Otolaryngol Head Neck Surg. 2008;134:50–56. doi: 10.1001/archoto.2007.4. [DOI] [PubMed] [Google Scholar]
- 10.Purcell DD, Fischbein NJ, Patel A, et al. Two temporal bone computed tomography measurements increase recognition of malformations and predict sensorineural hearing loss. Laryngoscope. 2006;116:1439–1446. doi: 10.1097/01.mlg.0000229826.96593.13. [DOI] [PubMed] [Google Scholar]
- 11.Lan MY, Shiao JY, Ho CY, et al. Measurements of normal inner ear on computed tomography in children with congenital sensorineural hearing loss. Eur Arch Otorhinolaryngol. 2009;266:1361–1364. doi: 10.1007/s00405-009-0923-x. [DOI] [PubMed] [Google Scholar]
- 12.Shim HG, Shin JE, Chung JW, et al. Inner ear anomalies in cochlear implantees: importance of radiologic measurements in the classification. Otol Neurotol. 2006;27:831–837. doi: 10.1097/01.mao.0000227902.47483.ef. [DOI] [PubMed] [Google Scholar]
- 13.Kawano A, Seldon HL, Clark GM. Computer-aided threedimensional reconstruction in human cochlear maps: measurement of the lengths of organ of Corti, outer wall, inner wall, and Rosenthal's canal. Ann Otol Rhinol Laryngol. 1996;105:701–709. doi: 10.1177/000348949610500906. [DOI] [PubMed] [Google Scholar]
- 14.Ketten DR, Skinner MW, Wang G, et al. In vivo measures of cochlear length and insertion depth of nucleus cochlear implant electrode arrays. Ann Otol Rhinol Laryngol. 1998;175:1–16. [PubMed] [Google Scholar]
- 15.Xu J, Xu SA, Cohen LT, et al. Cochlear view: postoperative radiography for cochlear implantation. Am J Otol. 2000;21:49–56. [PubMed] [Google Scholar]
- 16.Melhem ER, Shakir H, Bakthavachalam S, et al. Inner ear volumetric measurements using high-resolution 3D T2- weighted fast spin- echo MR imaging: initial experience in healthy subjects. AJNR Am J Neuroradiol. 1998;19:1819–1822. [PMC free article] [PubMed] [Google Scholar]
- 17.Connor SE, Bell DJ, O'Gorman R, et al. CT and MR imaging cochlear distance measurements may predict cochlear implant length required for a 360° insertion. AJNR Am J Neuroradiol. 2009;30:1425–1430. doi: 10.3174/ajnr.A1571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kendi TK, Arikan OK, Koc C. Volume of components of labyrinth: magnetic resonance imaging study. Otol Neurotol. 2005;26:778–781. doi: 10.1097/01.mao.0000169635.25322.9e. [DOI] [PubMed] [Google Scholar]
- 19.Paludetti G, Conti G, Nardo W, et al. Infant hearing loss: from diagnosis to therapy Official Report of XXI Conference of Italian Society of Pediatric Otorhinolaryngology. Acta Otorhinolaryngol Ital. 2012;32:347–370. [PMC free article] [PubMed] [Google Scholar]
- 20.Forli F, Arslan E, Bellelli S, et al. Systematic review of the literature on the clinical effectiveness of the cochlear implant procedure in paediatric patients. Acta Otorhinolaryngol Ital. 2011;31:281–298. [PMC free article] [PubMed] [Google Scholar]
- 21.Berrettini S, Baggiani A, Bruschini L, et al. Systematic review of the literature on the clinical effectiveness of the cochlear implant procedure in adult patients. Acta Otorhinolaryngol Ital. 2011;31:299–310. [PMC free article] [PubMed] [Google Scholar]