

Abstract
Background
Non-daily or intermittent smoking is becoming common, but little is known about smoking patterns of intermittent smokers (ITS). This study assesses differences in the profile of smoking motives of non-daily, ITS and daily smokers (DS).
Methods
Participants were 218 DS and 252 ITS (152 converted ITS [CITS], who previously smoked daily, and 80 native ITS [NITS] who did not), not currently quitting, recruited by advertisement. ITS were defined as smoking 4–27 days per month; DS as smoking daily, 5–30 cigarettes per day. Participants completed the Wisconsin Inventory of Smoking Dependence Motives (WISDM), yielding scores for 13 different motives. The within-profile standard deviation expressed profile scatter (differentiation among motives), and profile shape was assessed on scores standardized for within-profile mean and standard deviation.
Results
There was no difference between ITS and DS on profile scatter. ITS and DS differed in the shape of the standardized score profile, with DS scoring higher on Tolerance, Craving, Automaticity, Loss of Control and Behavioral Choice motives, and ITS scoring higher on Cue Exposure, Weight Control, and Positive Reinforcement motives. CITS did not differ from NITS in profile scatter or profile shape.
Conclusion
ITS differ from DS in the relative importance of motives, with ITS emphasizing motives associated with acute, situational smoking, and DS emphasizing dependence-related motives. Among ITS, history of daily smoking did not influence the profile of motives.
Keywords: Smoking, Non-daily smoking, Smoking motives, Nicotine dependence
1. Introduction
Smoking patterns are changing dramatically. Non-daily, or intermittent, smokers (ITS) now constitute 22–33% of adult smokers in the US (Centers for Disease Control and Prevention, 2008a,b, 2011; Substance Abuse and Mental Health Services Administration, 2009) and Western Europe (Korhonen et al., 2009; Lindstrom and Ostergren, 2001), and their proportions are growing rapidly (40% US increase between 1996 and 2001; Centers for Disease Control and Prevention, 2003). The reasons for this shift are not known, but may involve increasing restrictions on smoking (Shiffman, 2009). The emergence of ITS not only changes the profile of smoking, but also challenges our theoretical understanding of smoking behavior, which has emphasized dependence as the main driver of smoking, with nicotine maintenance and withdrawal-avoidance as primary motivators. While this description has fit the behavior of daily smokers (DS), we know little about the motives behind ITS’ smoking.
Understanding ITS’ motives for smoking seems crucial, because despite their relative freedom from dependence (Gilpin et al., 1997; Hennrikus et al., 1996; Shiffman et al., 2012b,c), ITS have difficulty in quitting. US population data (Tindle and Shiffman, 2011) show that ITS have very high failure rates, only slightly lower than those seen in DS. This suggests that ITS’ smoking is not casual, but has significant motivational roots.
We recently collected more detailed descriptions of ITS’ smoking behavior (Shiffman et al., 2012c). The ITS were not recent initiates: they averaged 35 years of age, and had been smoking for more than 19 years. Further, two-thirds had previously been DS. ITS reported they were especially likely to smoke when drinking alcohol or with other smokers, suggesting that they might fit the pattern expected of “social smokers” (Schane et al., 2009), but they also reported being likely to smoke when feeling stressed or distressed (more so than DS), which suggests that their smoking motives are complex. Not surprisingly, ITS scored far lower than DS on multiple measures of dependence (Shiffman et al., 2012b), though the data suggested that some ITS do show signs of dependence.
Observing that ITS are less dependent is not unexpected, but begs the question of their motives for smoking. In this paper, we analyze scores on the Wisconsin Inventory of Smoking Dependence Motives (WISDM; Piper et al., 2004), which yields scores on 13 different smoking motives (Table 1). Some of the scales tap “core” motives associated with dependence (labeled Primary Dependence Motives, or PDM), while others tap motives less clearly associated with dependence (Secondary Dependence Motives – SDM; Piasecki et al., 2010b; Piper et al., 2008). PDM predict dependence-related outcomes such as heaviness of smoking and relapse after quitting, but SDM are also related to dependence, and predict the emergence of craving and withdrawal (Piasecki et al., 2010a; Piper et al., 2008). Thus, both scales are related to dependence, and indeed are highly correlated (Piper et al., 2008). Consistent with Piasecki et al. (2007), we found (Shiffman et al., 2012b) that DS scored higher than ITS on both PDM and SDM.
Table 1.
WISDM subscales and hypotheses of outcomes by smoker type.
| WISDM scale | Description | Hypothesis about relative differencesa |
|---|---|---|
| Primary Dependence Motives | ||
| Tolerance | Needing to smoke more over time to get desired effects or ability to smoke large amounts without acute toxicity. | ↑ DS, whose smoking has increased to a greater degree, and whose relatively uninterrupted smoking seems more likely to induce tolerance |
| Craving | Smoking in response to craving or intense and/or frequent urges | ↑ DS, because craving is considered a hallmark of dependence |
| Automaticity | Smoking without awareness or intention. | ↑ DS, where smoking is frequent and routine, and thus subject to becoming automatic |
| Loss of Control | Perceived loss of volitional control over smoking. | ↑ DS, because of their greater dependence and apparent need to smoke. Loss of control is considered central to dependence (American Psychiatric Association, 2000) |
| Secondary Dependence Motives | ||
| Behavioral Choice | Smoking despite constraints or negative consequences and/or the lack of other options or reinforcers. | ↑ DS, because of insensitivity to consequences is a hallmark of addictive use (American Psychiatric Association, 2000), as is the dominance of drug use, compared to other activities, as a reinforcer (NDSS; Shiffman et al., 2004b) |
| Affiliative Attachment | Emotional attachment to smoking. | ↑ DS, because of their greater involvement in smoking |
| Cognitive Enhancement | Smoking to improve cognitive functioning | ? Unclear, because DS may be more likely to need smoking to overcome withdrawal-induced cognitive deficits, but cognitive enhancement may not depend on addiction (Shiffman et al., 1995; West and Hack, 1991), and ITS could seek acute cognitive enhancement in particular settings |
| Negative Reinforcement | The tendency or desire to smoke to ameliorate negative internal states. | ↑ DS, because much negative reinforcement is thought to be due to amelioration of withdrawal, and because negative-affect smoking patterns are closely tied to dependence (Kassel et al., 2003) |
| Positive Reinforcement | The desire to smoke to experience a “buzz” or to enhance an already positive feeling or experience. | ↑ ITS, because this refers to acute positive effects of smoking and because it is consistent with the hypothesis that ITS are social smokers who smoke in positive situations such as parties |
| Taste-Sensory Properties | Smoke to experience the smell, taste, and sensation of smoking. | ↑ ITS, for whom the immediate positive experience of smoking seems more relevant, whereas DS are thought to smoke to ameliorate the negative effects of not smoking. Consistent with the notion that dependence involves ‘wanting’ to smoke, rather than ‘liking’ to smoke (Robinson and Berridge, 1993) |
| Weight Control | The use of cigarettes to control body weight or appetite | ↑ ITS, for whom positive effects are likely to be more important. Weight control seems a prominent motive early in smoking careers (Austin and Gortmaker, 2001) and ITS smoking is seen as similar to early pre-addictive smoking |
| Cue Exposure | Perceived link between cue exposure and the desire or tendency to smoke. | ↑ ITS, as their smoking seems to be more situation-specific, in contrast to pervasive smoking among DS |
| Social Goads | Influenced by social stimuli or contexts that model or promote smoking. | ↑ ITS, as it is consistent with the view of ITS as social smokers. Social influence is also thought to be strongest early in smokers’ careers, before dependence has set in (Barton et al., 1982; Russell, 1971) |
Hypotheses refer to differences in relative differences within the standardized WISDM profiles, and not to differences in raw-score profiles, where we expect DS to always score higher, due to their greater engagement with and dependence on smoking.
We hypothesized that ITS’ and DS’ profile of motives would differ in ways beyond the predicable total score on PDM and SDM. Cronbach and Gleser (1953) have articulated an approach to profile analysis that considers three aspects of score profiles: (1) Elevation – the overall “height” of the profile: the mean score across all the subscales (cf. mean differences in Piasecki et al., 2007; Shiffman et al., 2012b); (2) Scatter – the degree to which scores vary from the mean, creating a varied profile vs. a flat one (indexed by the within-profile standard deviation); and (3) Shape – the actual profile across scores, reflecting patterns of motives, once elevation and scatter have been removed by standardizing each subject’s scores within their own profile mean and standard deviation. This reflects the relative prominence of scores within the profile.
Differences in elevation have already been established (Shiffman et al., 2012b). We propose hypotheses about the other two profile parameters (i.e., Scatter and Shape). We hypothesize that profile Scatter will be greater among ITS, because their intermittent smoking may reflect more specificity of motivation; that each ITS, perhaps idiosyncratically, will be driven by only a few motives but not others. In contrast, we expect DS to endorse many motives, which may help to explain why their smoking is so pervasive and resistant to change. Finally, our main hypotheses concern profile Shape – the relative importance of particular motives. Table 1 lists our hypotheses for which motives are likely to be more prominent in ITS vs. DS profiles, based on the expectation that motives tied closely to dependence will dominate DS profiles, while those more associated with specific, situational motives, and with acute use, will dominate ITS profiles. In other words, DS are expected to show higher relative endorsement of PDM while ITS show higher relative endorsement of SDM.
Using a similar approach, we previously found that chippers –who smoke at very low levels, though often daily – show a different profile from heavy smokers on questionnaires of smoking patterns and motives (Shiffman et al., 1994). Chippers emphasized social and sensory motives for smoking, whereas heavy smokers emphasized addiction and automaticity as motives. We expect similar patterns contrasting ITS and DS, but it is not clear whether non-daily smokers (ITS) studied at a time when such behavior is common, are similar to very light smokers (chippers) studied at a time when such behavior was very rare.
ITS are a heterogeneous group. In particular, some ITS have never smoked daily (“native” ITS or NITS), while others have evolved to ITS from a history of having been daily smokers (“converted” ITS, or CITS; Edwards et al., 2010; Nguyen and Zhu, 2009; Shiffman et al., 2012c; Tindle and Shiffman, 2011). CITS demonstrate greater dependence than NITS (Shiffman et al., 2012b), including scores on the PDM and SDM subscales of the WISDM, but their profile of motives has not been compared. We expect that given their history of daily smoking, CITS will be more like DS, with flatter profiles (lower profile scatter), and profiles emphasizing dependence-related motives.
Besides shedding light on ITS’ smoking motives, and differences between CITS and NITS, the present analyses can help validate the WISDM, and particularly the distinction between PDM and SDM. Since ITS are expected to be less motivated by classical dependence motives, the study represents a known-groups validation design. Observing that specific motives associated with PDM are relatively lower in ITS, and specific motives associated with SDM relatively higher in ITS, would help validate the WISDM constructs.
2. Methods
2.1. Participants
Participants were volunteers recruited via media to participate in a non-cessation study on smoking patterns. Participants had to be at least 21 years old, report smoking for ≥3 years and at their current rate for ≥3 months, and not be planning to quit within the next month. DS had to report smoking daily, an average of 5–30 cigarettes per day (CPD), while ITS just had to report smoking 4–27 days per month. The study sample is described in greater detail in Shiffman et al. (2012c).
DS (n = 218) were 37.2% African American (AA), 43.6% female, and averaged 40.7 (SD = 11.3) years of age. ITS (n = 252) were 31.0% AA, 50.4% female, and averaged 36.0 (SD = 12.3) years of age. DS reported having smoked on average 25.2 (SD = 10.9) years, averaged 15.0 (SD = 5.9) CPD, and had an average Fagerstrom Test for Nicotine Dependence (FTND; Heatherton et al., 1991) score of 5.1 (SD = 1.9). ITS smoked for an average of 18.0 (SD = 12.1) years, averaged 4.5 (SD = 2.9) CPD on days in which they smoked, and had a mean FTND score of 1.4 (SD = 1.6), with nearly half of ITS (44.4%) having FTND scores of 0.
Among ITS, CITS (n = 152) averaged 38.2 (SD = 12.4) years of age and NITS’ (n = 80) mean age was 33.3 (SD = 11.6) years. [Classification data were missing for 20 ITS, who thus do not participate in these analyses.] CITS were 37.5% AA and 56.6% female. Among NITS, 21.3% were AA and 41.3% were female. CITS reported having smoked, on average, for 20.2 (SD = 12.1) years, an average of 5.1 (SD = 3.1) CPD on smoking days, and had an average FTND score of 1.7 (SD = 1.8). NITS reported smoking an average of 13.4 (SD = 10.7) years, 3.3 (SD = 1.8) CPD on smoking days, and scored a mean of 0.9 (SD = 1.2) on the FTND.
Only participants (n = 471) who had non-missing scores for all 13 WISDM scores were included: 41 participants dropped from the study before completing the WISDM and 3 skipped multiple items. One additional participant who responded “7” to all WISDM items, yielding a highly implausible profile with no variation (SD = 0), and undefined standardized scale scores, was dropped. Finally, a subset of participants completed WISDM assessments for which 2 items (one contributing to the Taste-Sensory scale; one contributing to the Weight Control scale) were systematically missing. For these individuals, scores for the Taste-Sensory (n = 115) and Weight Control (n = 117) scales were imputed using highly predictive multivariate regression (R2s = .98) from other subscale items.
2.2. Assessment
Subjects completed the 68-item WISDM, which was scored to yield 13 subscales. Piper et al. (2004) reported high reliability for all subscales, and a consistent factor structure in daily and non-daily smokers, suggesting it is suitable for use in ITS. Subjects were interviewed about their smoking history, to determine whether they had ever smoked daily for 6 months or more (CITS) or not (NITS); see Shiffman et al. (2012c) for a more complete description.
2.3. Analyses
Profile scatter was indexed by the within-profile standard deviation across the 13 scales of the WISDM. To assess profile shape independent of Elevation and Scatter, we normalized each individual’s scores relative to their own profile’s mean (Elevation) and standard deviation (Scatter). To make all values positive and interpretable, we expressed these standardized scale scores as T scores, normed to a mean of 50 and a standard deviation of 10 (within the profile). The WISDM scales (both raw-score and normalized) were compared between groups using multivariate repeated-measures MANOVA, with the scores as dependent variables, and contrasts tested differences in particular scores. As an alternative approach, we also analyzed the rank ordering of WISDM scales within each subject’s profile, using a nonparametric one-way test of differences. This analysis produced essentially identical results, so is not reported here in detail.
3. Results
As shown in Table 2, contrary to our hypothesis, DS and ITS had similar within-profile standard deviations (scatter). Repeated-measures MANOVA showed a significant group-by-scale interaction, indicating differences in profile shape. These are seen in the standardized profile, shown in Fig. 1a. In between-group comparisons of the standardized scores, DS score higher than ITS (in order of the size of the differences) on Tolerance, Craving, Automaticity, Loss of Control, and Behavioral Choice, while ITS score higher on Social Goads, Cue Exposure, Weight Control, Taste/Sensory Properties, and Positive Reinforcement (and numerically higher scores on Negative Reinforcement). The groups did not differ on Affiliative or Cognitive Enhancement motives. On higher-order factors, DS scored higher than ITS on PDM, but ITS scored higher on SDM, as seen in Fig. 2a (interaction p < .0001).
Table 2.
WISDM subscale raw scores by smoker type.
| Profile parameters | DS n = 218
|
ITS n = 252
|
DS vs. ITS | CITS n = 152
|
NITS n = 80
|
CITS vs. NITS | CITS vs. DS | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p | Mean | SD | Mean | SD | p | p | |
| Elevation (mean) | 4.27 | 1.04 | 2.64 | .91 | <.0001 | 2.80 | .96 | 2.44 | .78 | .0029 | <.0001 |
| Scatter (SD) | 1.27 | .38 | 1.23 | .41 | ns | 1.24 | .37 | 1.20 | .45 | ns | ns |
| Scale scores (raw)† | |||||||||||
| Primary Dependence Motives | |||||||||||
| Tolerance | 4.73 | 1.39 | 1.81 | 1.22 | <.0001 | 2.07 | 1.36 | 1.45 | .82 | .0001 | <.0001 |
| Craving | 5.02 | 1.39 | 2.69 | 1.31 | <.0001 | 2.87 | 1.38 | 2.51 | 1.24 | .0422 | <.0001 |
| Automaticity | 4.39 | 1.55 | 2.23 | 1.37 | <.0001 | 2.40 | 1.49 | 1.96 | 1.08 | .0096 | <.0001 |
| Loss of Control | 4.13 | 1.58 | 1.99 | 1.18 | <.0001 | 2.27 | 1.26 | 1.69 | .96 | .0003 | <.0001 |
| Secondary Dependence Motives | |||||||||||
| Behavioral Choice | 3.71 | 1.43 | 1.89 | 1.00 | <.0001 | 2.04 | 1.07 | 1.77 | .88 | .0485 | <.0001 |
| Affiliative Attachment | 3.21 | 1.76 | 1.59 | 1.01 | <.0001 | 1.72 | 1.11 | 1.46 | .84 | .0620 | <.0001 |
| Cognitive Enhancement | 3.54 | 1.67 | 1.99 | 1.24 | <.0001 | 2.12 | 1.25 | 1.80 | 1.20 | .0501 | <.0001 |
| Negative Reinforcement | 4.42 | 1.42 | 2.98 | 1.37 | <.0001 | 3.09 | 1.39 | 2.83 | 1.32 | .1540 | <.0001 |
| Positive Reinforcement | 4.23 | 1.39 | 2.88 | 1.28 | <.0001 | 2.91 | 1.30 | 2.91 | 1.31 | .9933 | <.0001 |
| Taste-Sensory Properties | 4.82 | 1.28 | 3.69 | 1.45 | <.0001 | 3.85 | 1.37 | 3.51 | 1.49 | .0711 | <.0001 |
| Weight Control | 2.79 | 1.75 | 1.89 | 1.36 | <.0001 | 2.03 | 1.44 | 1.69 | 1.29 | .0712 | <.0001 |
| Cue Exposure | 4.84 | 1.27 | 3.85 | 1.38 | <.0001 | 4.00 | 1.35 | 3.71 | 1.39 | .1092 | <.0001 |
| Social Goads | 4.61 | 1.92 | 3.73 | 1.86 | <.0001 | 3.91 | 1.82 | 3.41 | 1.84 | .0442 | <.0001 |
Scales shown in order of the magnitude of differences between DS and ITS.
Fig. 1.
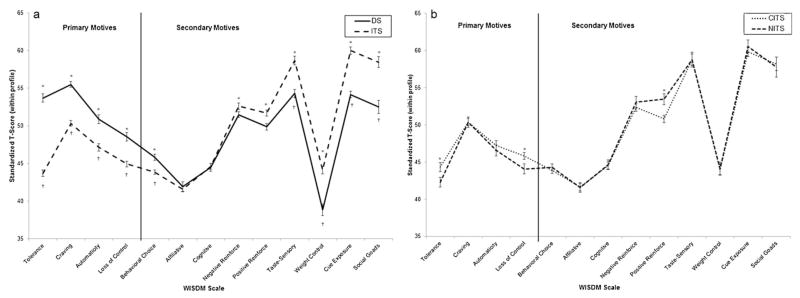
Profile of WISDM scores, standardized by each smoker’s mean and SD across the 13 scales of the WISDM, then scaled as T scores, with within-profile M = 50 and SD = 10. Scales are ordered by the size of the difference between DS and ITS. The vertical line and labels demarcate WISDM scales considered part of Primary Dependence Motives vs. Secondary Dependence Motives. (This classification had no role in the analysis, but is shown to indicate how the results map onto this classification.) (a) Profiles of DS and ITS differed significantly, based on a scale × group interaction in multivariate repeated-measures analysis (p < .0001). (b) Profiles of CITS and NITS did not differ significantly, based on a scale × group interaction in multivariate repeated-measures analysis (p > .35). However, some individual scale scores did differ, as indicated by asterisks. *p < .05 for individual scale comparisons between ITS and DS. †p < .05 for individual scale comparisons between CITS and DS.
Fig. 2.
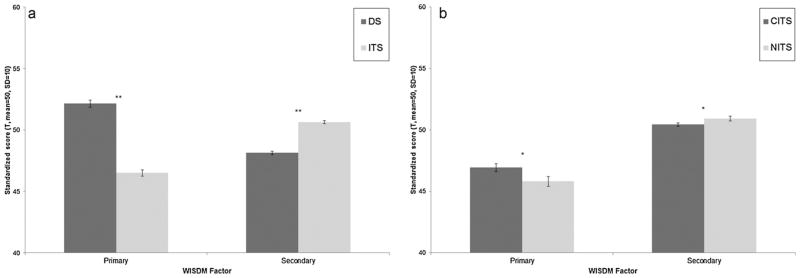
Computed values of Primary and Secondary Dependence Motives (PDM and SDM, respectively) summary scores, based on scale scores standardized by each smoker’s mean and SD across the 13 scales of the WISDM, then scaled as T scores, with within-profile mean = 50 and SD = 10. (a) DS score significantly higher on PDM (p < .0001), lower on SDM (p < .0001); interaction p < .0001. (b) CITS score significantly higher on PDM (p < .04), and lower on SDM, by non-parametric test (p < .05); interaction p < .05. *p < .05; **p < .0001.
Comparing the profiles of CITS and NITS showed no differences in profile scatter (Table 2). On contrasts based on standardized scores of individual scales, CITS scored higher in Tolerance and Loss of Control, while NITS scored higher on Positive Reinforcement. However, repeated-measures analysis yielded no significant group-by-scale interactions: the shapes of NITS’ and CITS’ profiles were not reliably different, despite the variations in the significance of differences on particular scales (Fig. 1b). On higher-order factors, CITS scored significantly higher on PDM, while NITS scored significantly higher on SDM (by non-parametric test). The group-by-scale interaction was significant (p < .05; see Fig. 2b).
Because CITS scored intermediate between NITS and DS, and were formerly DS, we also tested differences between CITS and DS. On raw scores, DS scored significantly higher on all scales (Table 2). On standardized scores, DS scored higher on all PDM scales, as well as Behavioral Choice, and lower on Social Goads, Cue Exposure, Weight Control, and Taste-Sensory motives, largely paralleling ITS–DS differences (Fig. 1).
4. Discussion
Previous analyses (Piasecki et al., 2007; Shiffman et al., 2012b) had demonstrated that ITS are less dependent than DS on multiple measues, including the WISDM. This analysis of the WISDM scales extends prior results by demonstrating differences between DS and ITS in the profiles of smoking motives. Whereas DS had relatively higher scores on the Tolerance, Craving, Automaticity, Loss of Control, and Behavioral Choice scales, ITS had higher relative scores on Social Goads, Cue Exposure, Weight Control, Positive Reinforcement, and Taste-Sensory motives. In other words, DS’ profiles emphasized motives associated with traditional models of dependence (so-called “trough maintenance”; Russell, 1971), whereas ITS’ profiles did not. The motives most important in DS’ profiles reflect dependence processes that lead to greater tobacco consumption, more continuous consumption, and loss of voluntary control – core characteristics of dependence. In contrast, ITS endorse motives that facilitate tobacco use even if one is not nicotine dependent in the traditional sense, and not smoking continuously (so called “peak-seeking”; Russell, 1971). Further, the motives most highly endorsed by ITS – Social Goads and Cue Exposure – imply being motivated to smoke in particular circumstances and in response to particular cues, rather than needing to smoking continually, which would be a hallmark of dependent smoking, as conventionally construed. Thus, the analysis of standardized WISDM profiles demonstrates that there are qualitative as well as quantitative differences in DS’ and ITS’ motives for smoking.
Our findings validate the proposed distinction (Piasecki et al., 2010a; Piper et al., 2008) between PDM and SDM: In analyses across all motives, with no preconceived organization of motives into PDM and SDM, DS emphasized motives that were part of the PDM cluster, while ITS emphasized motives associated with SDM. Differences between DS and ITS on scales within the standardized profiles (Fig. 1a) map remarkably well onto the assignment of scales to PDM and SDM (Piper et al., 2008), and our analysis of the secondary factor scores confirm the pattern. Our findings are also roughly consistent with the hypothesis put forth by Piper et al. (2008) and Piasecki et al. (2010a) that motives such as Craving, Automaticity, and Loss of Control (which were relatively more important among DS than ITS) emerge only after smokers progress to smoking heavily and develop other hallmarks of nicotine dependence (as traditionally defined), whereas other motives develop and increase well before this. We find these “primary” motives to be relatively more important among DS than ITS. However, Piper et al. (2004) also identified Behavioral Choice, Cognitive Enhancement, and Positive and Negative Reinforcement as late-emerging motives, yet we found that ITS give similar or even more weight to these motives relative to others. This may reflect the fact that ITS are not novice smokers, having smoked an average of 42,850 cigarettes (Shiffman et al., 2012c), so may well evince late-emerging motives, consistent with our observation (Shiffman et al., 2012b) that ITS do exhibit signs of dependence.
The motives on which ITS score higher than DS in relative endorsement are telling: the greatest difference in endorsement between groups is for Social Goads, consistent with the frequent assumption that ITS are “social smokers” (Schane et al., 2009) whose smoking is driven primarily by social factors, especially the presence of friends who are smoking. Yet it remains to be seen whether this truly accounts for ITS’ smoking; the fact that ITS were more likely to endorse stressful situations as occasions for smoking (Shiffman et al., 2012c) suggests that their smoking motives and patterns may be more than simply social.
ITS also gave the greatest emphasis to Cue Exposure motives – the tendency to smoke in particular situations but not others, depending on the cues present. Although DS are also thought to be influenced by cues (Carter and Tiffany, 1999; Ferguson and Shiffman, 2009; Niaura et al., 1988; Shiffman et al., 2012a, 2002), the fact that such motives are particularly prominent in ITS’ profiles is consistent with a stimulus-control account of ITS’ smoking (Shiffman et al., 2012b; Shiffman and Paty, 2006), which posits that ITS’ smoking comes under control of situational stimuli, such that smoking is prompted by particular cues, often external ones, instead of the endogenous rhythms of nicotine intake and clearance that are thought to drive the smoking of typical dependent smokers.
It was striking that ITS scored higher in the relative importance of Positive Reinforcement. Most theories of smoking suggest that positive reinforcement fades in importance as dependence progresses and negative reinforcement comes to dominate smoking. These data are consistent with that, though the small size of the difference suggests that positive reinforcement may continue to be important even in heavy and dependent smokers. ITS’ equal or greater emphasis (compared to DS) on negative reinforcement motives is consistent with their reports that they often smoke when emotionally distressed (Shiffman et al., 2012c), and with the finding of Piasecki et al. (2007) that non-daily smoking college students are more likely to say they smoke in order to cope with distress. However, it is at odds with most accounts of negative reinforcement by smoking, which typically attribute negative-affect smoking to relief of withdrawal symptoms caused by dependence (Eissenberg, 2004; Parrott, 1999). Since ITS demonstrate little to no dependence on traditional scales (Shiffman et al., 2012b,c) and demonstrate no withdrawal when they abstain, withdrawal-management cannot account for their reports of Negative Reinforcement. It has been proposed (Kassel et al., 2003) that nicotine may have direct distress-relief effects that do not depend on withdrawal-relief, but actually reduce distress from exogenous sources. Thus, ITS’ higher scores may reflect use of smoking for instrumental purposes, which is more associated with non-dependent smoking. DS’ lower scores on Negative Reinforcement may reflect the fact that the frequent smoking of DS may overwhelm or mask the relationship with affect. Indeed, EMA studies have shown no relationship between smoking and negative affect (Carter et al., 2008; Shiffman et al., 2002, 2004a). At the same time, EMA data (Shiffman et al., 1996; Shiffman and Waters, 2004) show that this association is quite strong when smokers are quitting. These context-specific differences underscore how such associations may vary according to abstinence status and phase of smoking; thus, the relationships described by the WISDM during ad lib. smoking may not apply when smokers are quitting. This issue requires further study.
We had hypothesized that ITS would have more jagged or scattered profiles of motives, emphasizing a few particular motives over others, but this was not supported. It appears that individual ITS, like DS, smoke for multiple reasons, rather than for just one or two. This diversity of motives may strongly root smoking in ITS’ behavioral repertoires, helping to explain why they have so much trouble giving up smoking, as indicated by analyses of national data (Tindle and Shiffman, 2011) showing that almost 80% of ITS’ quit efforts fail.
Surprisingly, CITS and NITS did not differ in their profile across the standardized WISDM motives. However, CITS scored higher on PDM, and lower on SDM, mirroring in a more subtle way the pattern seen for DS. Despite their history of daily smoking, CITS differed from DS much in the way NITS did. This suggests that, regardless of past history of daily smoking, individuals who now smoke intermittently emphasize situational motives to smoke, more than motives reflecting constant smoking or loss of control.
The cross-sectional design of this study precludes knowing whether the observed differences in smoking motives are causes or effects of subjects’ smoking status. Thus, we cannot say whether CITS’ profile of motives shifted as they changed from DS to CITS, or whether their NITS-like profile reflects a pre-existing variation in motives that enabled them to evolve from DS to ITS. Similarly, it remains unclear whether smokers who start their careers with a particular motives profile are able to avoid progressing to daily and dependent smoking and thus become ITS, or, alternatively, whether all smokers begin with similar profiles, but the profile shifts as most progress to daily smoking. Fundamentally, then, this study cannot determine the underlying causal factors that make some smokers DS and others ITS. It is likely that genetic factors play some role (Sullivan and Kendler, 1999). However, given ITS’ rapidly increasing prevalence in the last decade alone, environmental forces such as smoking restrictions likely promote ITS’ smoking behavior, perhaps interacting with genetic factors (Boardman, 2009; Boardman et al., 2010; Shiffman, 2009).
The study does, however, shed light on the dependence and motives of ITS. It has been suggested that dependence, craving, and loss of control develop very quickly after a few exposures to smoking (DiFranza et al., 2007, 2011). However, although we observe some inklings of dependence among ITS (Shiffman et al., 2012b), the levels are very low, and levels of Craving, Automaticity, Tolerance, and Loss of Control – the classic core of dependence – are particularly low, despite ITS having smoked for many years and consumed tens of thousands of cigarettes (Shiffman et al., 2012c). The analysis of motives profiles suggests instead that whatever dependence ITS exhibit is not only of a different magnitude, but also of a different character, emphasizing instrumental and situational use and reinforcement.
Our study was subject to certain limitations. The WISDM is based on global self-reports of when and why subjects smoke. Though there is some evidence for the validity of the WISDM (Piasecki et al., 2007), including some validation against reports from ecological momentary assessment (Piasecki et al., 2011), the validity of such measures has been questioned, both with respect to actual smoking patterns (Shiffman, 1993) and with regard to motives, which are notoriously difficult to access by introspection and retrospection (Shiffman et al., 1997). In addition, the study was based on a sample of convenience ascertained in one US city. That said, the characteristics of our DS sample were similar to a nationally representative population (Tindle and Shiffman, 2011) with regard to variables such as gender, daily cigarette consumption, and time to first cigarette, suggesting that the sample is not unreasonably skewed.
In summary, this demonstrated that ITS and DS differ in their profiles of smoking motives. Controlling for overall dependence, DS gave greater weight to motives associated with dependence and with continual smoking, such as Tolerance, Craving, Automaticity, and Loss of Control, while ITS gave greater weight to motives associated with situational influences and effects of smoking, such as Cue Exposure, Taste-Sensory effects of smoking, and Positive Reinforcement from smoking. Thus, ITS differ not only in the degree of motivation to smoke, but also in their pattern of motives for smoking. ITS have difficulty quitting (Tindle and Shiffman, 2011), and thus may need intervention; these results suggest that treatment would need to take account ITS’ different motives, emphasizing acute and situational influences rather than the addictive influences that drive DS’ smoking. The role of motivational profiles in explaining smoking and cessation deserves continuing consideration.
Acknowledgments
The authors are grateful to Stuart Ferguson, Thomas Kirchner, and Deborah Scharf for help launching this study and for input on study design; to Anna Tsivina, Joe Stafura, Rachelle Gish, and Aileen Butera for their work conducting research sessions; to Chantele Mitchell-Miland and Sarah Felter for data management and preparation; and to Laura Homonnay-Demilio for editorial assistance.
Role of funding source
This work was supported by Grant R01-DA020742 (Shiffman) from the National Institutes of Health, National Institute on Drug Abuse. Additional support was provided by National Science Foundation Graduate Research Fellowship (Dunbar), National Center for Research Resources (KL2-RR024154-03; Tindle), and National Cancer Institute Grants R25-CA057703-15 (Dunbar) and R01-CA141596-02 (Tindle). None of these institutions played a direct role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.
Footnotes
Contributors
Author Shiffman designed the study and authors Scholl and Tindle participated in the development of the protocol. All authors contributed to the literature searches and summaries of previous related work. Authors Shiffman and Dunbar undertook the statistical analysis, and author Shiffman wrote the first draft of the manuscript. All authors contributed to and have approved the final manuscript.
Conflict of interest
All authors declare that they have no conflict of interest.
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV-TR) American Psychiatric Association; Washington, DC: 2000. [Google Scholar]
- Austin S, Gortmaker S. Dieting and smoking initiation in early adolescent girls and boys: a prospective study. Am J Public Health. 2001;91:446–450. doi: 10.2105/ajph.91.3.446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barton J, Chassin L, Presson CC, Sherman SJ. Social image factors as motivators of smoking initiation in early and middle adolescence. Child Dev. 1982;53:1499–1511. [PubMed] [Google Scholar]
- Boardman JD. State-level moderation of genetic tendencies to smoke. Am J Public Health. 2009;99:480–486. doi: 10.2105/AJPH.2008.134932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boardman JD, Blalock CL, Pampel FC. Trends in the genetic influences on smoking. J Health Soc Behav. 2010;51:108–123. doi: 10.1177/0022146509361195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carter BL, Lam CY, Robinson JD, Paris MM, Waters AJ, Wetter DW, Cinciripini PM. Real-time craving and mood assessments before and after smoking. Nicotine Tob Res. 2008;10:1165–1169. doi: 10.1080/14622200802163084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carter BL, Tiffany ST. Meta-analysis of cue-reactivity in addiction research. Addiction. 1999;94:327–340. [PubMed] [Google Scholar]
- Centers for Disease Control Prevention. Prevalence of current cigarette smoking among adults and changes in prevalence of current and some day smoking – United States, 1996–2001. MMWR. 2003;52:303–307. [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System Survey Data. U.S. Department of Health and Human Services; Atlanta, GA: 2008a. [Google Scholar]
- Centers for Disease Control Prevention. Cigarette smoking among adults – United States, 2007. MMWR. 2008b;57:1221–1226. [PubMed] [Google Scholar]
- Centers for Disease Control Prevention. Vital signs: Current cigarette smoking among adults aged >18 years – United States, 2005–2010. MMWR. 2011;60:1207–1212. [PubMed] [Google Scholar]
- Cronbach LJ, Gleser GC. Assessing similarity between profiles. Psychol Bull. 1953;50:456–473. doi: 10.1037/h0057173. [DOI] [PubMed] [Google Scholar]
- DiFranza JR, Savageau JA, Fletcher K, O’Loughlin J, Pbert L, Ockene JK, McNeill AD, Hazelton J, Friedman K, Dussault G, Wood C, Wellman RJ. Symptoms of tobacco dependence after brief intermittent use: the Development and Assessment of Nicotine in Youth-2. Arch Pediatr Adolesc Med. 2007;161:704–710. doi: 10.1001/archpedi.161.7.704. [DOI] [PubMed] [Google Scholar]
- DiFranza JR, Wellman RJ, Mermelstein R, Pbert L, Klein JD, Sargent JD, Ahluwalla JS, Lando HA, Ossip DJ, Wilson KM, Balk SJ, Hipple B, Tanski SE, Prokhorov AV, Best D, Winickoff JP. The natural history and diagnosis of nicotine addiction. Curr Rev Pediatr. 2011;72:88–96. [Google Scholar]
- Edwards SA, Bondy SJ, Kowgier M, McDonald PW, Cohen JE. Are occasional smokers a heterogeneous group? An exploratory study. Nicotine Tob Res. 2010;12:1195–1202. doi: 10.1093/ntr/ntq168. [DOI] [PubMed] [Google Scholar]
- Eissenberg T. Measuring the emergence of tobacco dependence: the contribution of negative reinforcement models. Addiction. 2004;99:5–29. doi: 10.1111/j.1360-0443.2004.00735.x. [DOI] [PubMed] [Google Scholar]
- Ferguson SG, Shiffman S. The relevance and treatment of cue-induced cravings in tobacco dependence. J Subst Abuse Treat. 2009;36:235–243. doi: 10.1016/j.jsat.2008.06.005. [DOI] [PubMed] [Google Scholar]
- Gilpin E, Cavin S, Pierce J. Adult smokers who do not smoke daily. Addiction. 1997;92:473–480. [PubMed] [Google Scholar]
- Heatherton TF, Kozlowski LT, Frecker RC, Fagerstrom KO. The Fagerstrom Test for Nicotine Dependence: a revision of the Fagerstrom Tolerance Questionnaire. Br J Addict. 1991;86:1119–1127. doi: 10.1111/j.1360-0443.1991.tb01879.x. [DOI] [PubMed] [Google Scholar]
- Hennrikus DJ, Jeffery RW, Lando HA. Occasional smoking in a Minnesota working population. Am J Public Health. 1996;86:1260–1266. doi: 10.2105/ajph.86.9.1260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kassel JD, Stroud LR, Paronis CA. Smoking, stress, and negative affect: correlation, causation, and context across stages of smoking. Psychol Bull. 2003;129:270–304. doi: 10.1037/0033-2909.129.2.270. [DOI] [PubMed] [Google Scholar]
- Korhonen T, Broms U, Levalahti E, Koskenvuo M, Kaprio J. Characteristic and health consequences of intermittent smoking: long-term follow-up among Finnish adult twins. Nicotine Tob Res. 2009;11:148–155. doi: 10.1093/ntr/ntn023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindstrom M, Ostergren P. Intermittent and daily smokers: two different socioeconomic patterns, and diverging influence of social participation. Tob Control. 2001;10:258–266. doi: 10.1136/tc.10.3.258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nguyen QB, Zhu S. Intermittent smokers who used to smoke daily: a preliminary study on smoking situtations. Nicotine Tob Res. 2009;11:164–170. doi: 10.1093/ntr/ntp012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Niaura RS, Rohsenow DJ, Binkoff JA, Monti PM, Pedraza M, Abrams DB. Relevance of cue reactivity to understanding alcohol and smoking relapse. J Abnorm Psychol. 1988;97:133–152. doi: 10.1037//0021-843x.97.2.133. [DOI] [PubMed] [Google Scholar]
- Parrott AC. Does cigarette smoking cause stress? Am Psychol. 1999;54:817–820. doi: 10.1037//0003-066x.54.10.817. [DOI] [PubMed] [Google Scholar]
- Piasecki TM, Piper ME, Baker T. Refining the tobacco dependence phenotype using the Wisconsin Inventory of Smoking Dependence Motives: II. Evidence from a laboratory self-administration assay. J Abnorm Psychol. 2010a;119:513–523. doi: 10.1037/a0020235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piasecki TM, Piper ME, Baker T. Tobacco dependence: insights from investigations of self-reported smoking motives. Curr Dir Psychol Sci. 2010b;19:395–401. doi: 10.1177/0963721410389460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piasecki TM, Piper ME, Baker TB, Hunt-Carter EE. WISDM primary and secondary dependence motives: associations with self-monitored motives for smoking in two college samples. Drug Alcohol Depend. 2011;114:207–216. doi: 10.1016/j.drugalcdep.2010.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piasecki TM, Richardson AE, Smith SM. Self-monitored motives for smoking among college students. Psychol Add Beh. 2007;21:328–337. doi: 10.1037/0893-164X.21.3.328. [DOI] [PubMed] [Google Scholar]
- Piper ME, Bolt DM, Kim S, Japuntich SJ, Smith SS, Niederdeppe J, Cannon DS, Baker TB. Refining the tobacco dependence phenotype using the Wisconsin Inventory of Smoking Dependence Motives. J Abnorm Psychol. 2008;117:747–761. doi: 10.1037/a0013298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piper ME, Piasecki TM, Federman EB, Bolt DM, Smith SS, Fiore MC. A multiple motives approach to tobacco dependence: the Wisconsin Inventory of Smoking Dependence Motives. J Consult Clin Psychol. 2004;72:139–154. doi: 10.1037/0022-006X.72.2.139. [DOI] [PubMed] [Google Scholar]
- Robinson TE, Berridge KC. The neural basis of drug craving: an incentive-sensitization theory of addiction. Brain Res Rev. 1993;18:247–291. doi: 10.1016/0165-0173(93)90013-p. [DOI] [PubMed] [Google Scholar]
- Russell MAH. Cigarette smoking: the natural history of a dependence disorder. Br J Med Psychol. 1971;44:1–16. doi: 10.1111/j.2044-8341.1971.tb02141.x. [DOI] [PubMed] [Google Scholar]
- Schane RE, Glantz SA, Ling PM. Nondaily and social smoking: an increasingly prevalent pattern. Arch Intern Med. 2009;169:1742–1744. doi: 10.1001/archinternmed.2009.315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S. Assessing smoking patterns and motives. J Consult Clin Psychol. 1993;61:732–742. doi: 10.1037//0022-006x.61.5.732. [DOI] [PubMed] [Google Scholar]
- Shiffman S. Light and intermittent smokers: background and perspective. Nicotine Tob Res. 2009;11:122–125. doi: 10.1093/ntr/ntn020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S, Dunbar M, Kirchner T, Li X, Tindle H, Anderson S, Scholl S. Smoker reactivity to cues: effects on craving and on smoking behavior. J Abnorm Psychol. 2012a doi: 10.1037/a0028339. http://dx.doi.org/10.1037/a0028339. [DOI] [PMC free article] [PubMed]
- Shiffman S, Ferguson SG, Dunbar MS, Scholl SM. Tobacco dependence among intermittent smokers. Nicotine Tob Res. 2012b doi: 10.1093/ntr/nts097. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S, Tindle H, Li X, Scholl S, Dunbar M, Mitchell-Miland C. Characteristics and Smoking Patterns of Intermittent Smokers. Exp Clin Psychopharmacol. 2012c doi: 10.1037/a0027546. http://dx.doi.org/10.1037/a0027546. [DOI] [PMC free article] [PubMed]
- Shiffman S, Gwaltney CJ, Balabanis M, Liu KS, Paty JA, Kassel JD, Hickcox M, Gnys M. Immediate antecedents of cigarette smoking: an analysis from ecological momentary assessment. J Abnorm Psychol. 2002;111:531–545. doi: 10.1037//0021-843x.111.4.531. [DOI] [PubMed] [Google Scholar]
- Shiffman S, Hufford M, Hickcox M, Paty JA, Gnys M, Kassel JD. Remember that? A comparison of real-time versus retrospective recall of smoking lapses. J Consult Clin Psychol. 1997;65:292–300. doi: 10.1037/0022-006x.65.2.292.a. [DOI] [PubMed] [Google Scholar]
- Shiffman S, Kassel JD, Paty JA, Gnys M, Zettler-Segal M. Smoking typology profiles of chippers and regular smokers. J Subst Abuse. 1994;6:21–35. doi: 10.1016/s0899-3289(94)90052-3. [DOI] [PubMed] [Google Scholar]
- Shiffman S, Paty JA. Smoking patterns and non-dependent smokers: contrasting chippers and dependent smokers. J Abnorm Psychol. 2006;115:509–523. doi: 10.1037/0021-843X.115.3.509. [DOI] [PubMed] [Google Scholar]
- Shiffman S, Paty JA, Gnys M, Kassel JD, Elash C. Nicotine withdrawal in chippers and regular smokers: subjective and cognitive effects. Health Psychol. 1995;14:301–309. doi: 10.1037//0278-6133.14.4.301. [DOI] [PubMed] [Google Scholar]
- Shiffman S, Paty JA, Gnys M, Kassel JD, Hickcox M. First lapses to smoking: within-subjects analyses of real-time reports. J Consult Clin Psychol. 1996;64:366–379. doi: 10.1037//0022-006x.64.2.366. [DOI] [PubMed] [Google Scholar]
- Shiffman S, Paty JA, Gwaltney CJ, Dang Q. Immediate antecedents of cigarette smoking: an analysis of unrestricted smoking patterns. J Abnorm Psychol. 2004a;113:116–171. doi: 10.1037/0021-843X.113.1.166. [DOI] [PubMed] [Google Scholar]
- Shiffman S, Waters AJ. Negative affect and smoking lapses: a prospective analysis. J Consult Clin Psychol. 2004;72:192–201. doi: 10.1037/0022-006X.72.2.192. [DOI] [PubMed] [Google Scholar]
- Shiffman S, Waters AJ, Hickcox M. The Nicotine Dependence Syndrome Scale: a multi-dimensional measure of nicotine dependence. Nicotine Tob Res. 2004b;6:327–348. doi: 10.1080/1462220042000202481. [DOI] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration. Results from the National Survey on Drug Use and Health: National Findings. NSDUH Series Office of Applied Studies; Rockville, MD: 2009. [Google Scholar]
- Sullivan PF, Kendler KS. The genetic epidemiology of smoking. Nicotine Tob Res. 1999;1 (Suppl 2):S51–S57. doi: 10.1080/14622299050011811. discussion S69–S70. [DOI] [PubMed] [Google Scholar]
- Tindle HA, Shiffman S. Smoking cessation behavior among intermittent smokers versus daily smokers. Am J Public Health. 2011;101:e1–e3. doi: 10.2105/AJPH.2011.300186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- West R, Hack S. Effect of cigarettes on memory search and subjective ratings. Pharmacol Biochem Behav. 1991;38:281–286. doi: 10.1016/0091-3057(91)90279-b. [DOI] [PubMed] [Google Scholar]