

Abstract
Sepsis remains a leading cause of death in critically ill patients, despite efforts to improve patient outcome. Thus far, no magic drugs exist for severe sepsis and septic shock. Instead, early diagnosis and prompt initial management such as early goal-directed therapy are key to improve sepsis outcome. For early detection of sepsis, biological markers (biomarkers) can help clinicians to distinguish infection from host response to inflammation. Ideally, biomarkers can be used for risk stratification, diagnosis, monitoring of treatment responses, and outcome prediction. More than 170 biomarkers have been identified as useful for evaluating sepsis, including C-reactive protein, procalcitonin, various cytokines, and cell surface markers. Recently, studies have reported on the usefulness of biomarker-guided antibiotic stewardships. However, the other side of these numerous biomarkers is that no novel single laboratory marker can diagnose, predict, and track the treatment of sepsis. The purpose of this review is to summarize several key biomarkers from recent sepsis studies.
Keywords: Biomarkers, Cytokines, Diagnosis, Outcome, Prognosis, Sepsis
Introduction
1. Sepsis: Where are we now?
Severe sepsis and septic shock are leading causes of death, representing 30-50% of hospital-reported mortality [1]. Sepsis treatment outcomes are disappointing, despite a long history of interventions, such as numerous antibiotics including penicillin, efforts to follow guidelines from the Surviving Sepsis Campaign (SSC), and development of supportive modalities for organ dysfunctions accompanying sepsis (e.g., dialysis, ventilators, extracorporeal membrane oxygenation). We have seen the rise and fall of recombinant human activated protein C (drotrecogin alfa) for the treatment of severe sepsis, while the disappointing results might be explained by statistical insignificance stemming from the relatively lower mortality rate (25%) in the Protein C Worldwide Evaluation in Severe Sepsis (PROWESS) study [2, 3]. In addition to activated protein C, treatments with agents such as toll-like receptor (TLR) 4-blocker (eritoran) and human recombinant lactoferrin (talactoferrin) are also viewed with skepticism [4, 5, 6]. Failure of these treatments in clinical trials might be predictable for several reasons. Sepsis is the result of a complex chain of events composed of innate and adaptive immune responses, including activation of the complement system, coagulation cascades, and the vascular endothelial system (Fig. 1). Such complexity makes it difficult for new drugs targeting a single immunological event to improve sepsis outcome. In addition, immune responses are based on individual patient factors including age, underlying diseases, nutritional state, and even genetic variability. For this reason, treatments, especially immunotherapy, have to be individualized. Furthermore, pathogen factors also vary by patient. Given that adjunctive therapy for sepsis has shown disappointing results, conventional management is of immediate importance in the real world. Practically, "bundled care" for sepsis, with early administration of appropriate antibiotics and supportive care based on SSC guidelines, improves outcome [7, 8]. This emphasizes the necessity for early and accurate detection of sepsis. However, a definite microbiological diagnosis cannot be made in approximately one-third of patients with clinical manifestations of sepsis [9, 10]. For this reason, good biomarkers can guide the early diagnosis and management of sepsis. Here, we discuss sepsis biomarkers and directions for future research.
Figure 1.

Systemic responses to sepsis and possible biomarkers. Systemic response to sepsis results from multiple changes to the inflammatory, coagulatory, and vascular systems. Candidate biomarkers include proteins such as cytokines, soluble receptors, and acute phase reactants.
DAMP, damage-associated molecular pattern; PAMP, pathogen-associated molecular pattern; SIRS, systemic inflammatory response syndrome.
2. Pathophysiology of sepsis
Sepsis is the result of host response to infection by microbial pathogens, meaning that antimicrobial agents are insufficient for treatment of this infectious disease. In 1904, William Osler noted, "It appears that patients are dying not from their infections but rather their reaction to them." Sepsis has traditionally been considered as a result of uncontrolled inflammatory response, a "cytokine storm" that results in shock or organ dysfunction [11]. More than 30 clinical trials have focused on blocking these inflammatory cascades, such as steroids, tumor necrosis factor (TNF)-α antagonist, and anti-endotoxin. However, the paradigm of sepsis understanding and treatment has shifted toward its immunosuppressive effects [12]. For example, elderly patients with sepsis are lack of fever and other immune responses, that are associated with poor prognosis. Such immunosuppression is now considered a key pathogenesis associated with sepsis mortality. Immunosuppressed conditions lead to secondary infections due to nosocomial pathogens such as Acinetobacter, Enterococcus, Stenotrophomonas, or Candida species, which could worsen outcome. In addition, several clinical trials have shown that immune-enhancing therapies such as recombinant human interleukin (IL)-7 and granulocyte-macrophage colony-stimulating factor may have beneficial effects [13, 14]. Immunosuppression in sepsis has been also identified in post-mortem studies of patients who died of sepsis [11, 15]. There was a marked decrease in lipopolysaccharide (LPS)-stimulated cytokine secretion of mediators including TNF, interferon-γ, IL-6, and IL-10 in splenocytes from patients diagnosed with sepsis. In addition, immune effector cells, including clusters of differentiation (CD) 4, CD8 cells, and human leukocyte antigen-DR were significantly decreased in splenic tissue of patients dying of sepsis compared to control patients [15]. Early hyper-inflammatory and late compensatory anti-inflammatory response syndromes are included in current immunological models of sepsis (Fig. 2). However, this is not a simple biphasic model in many cases. The degree and duration of immune response differs from patient to patient according to age, underlying physical state, comorbidities, pathogen virulence, pathogen burden, and genetic factors. These cycles may repeat, with waxing and waning of clinical symptoms. During the course of sepsis, the duration and degree of immunosuppression could affect the outcome, which leads us to consider tailored immunomodulatory therapy.
Figure 2.

Inflammatory response to sepsis. Immune response to sepsis is both proinflammatory and anti-inflammatory. An initial hyper-inflammatory phase is followed by a hypo-inflammatory (immunosuppressive) phase. Immunosuppression in sepsis contributes to increased mortality in elderly patients. Ideally, good biomarkers can reflect the hyper- (A) or hypo-inflammatory (B) status and the direction of inflammatory response (A or C).
Biomarkers of sepsis
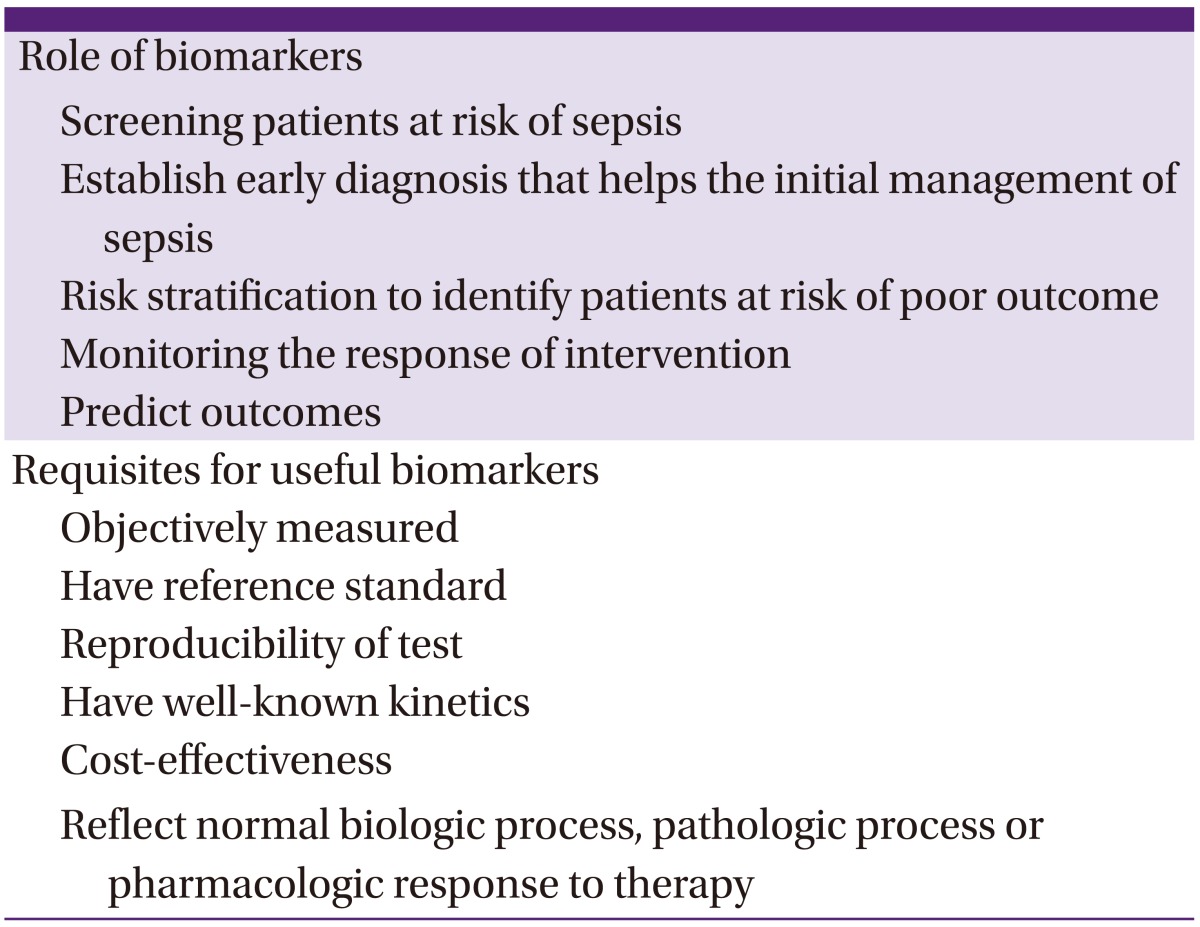
An ideal biomarker can be objectively measured and reflects normal biological and pathogenic processes as well as responses to therapeutic interventions [16]. Many trials have identified potential biomarkers. More than 170 biomarkers have been studied for use in evaluation of sepsis [17]. Development of sepsis changes the expression and activity of thousands of endogenous mediators of inflammation, coagulation, and intermediary metabolism [18, 19]. Even when biomarkers start at equal values, the effect of inflammatory responses can cause these values to change in opposite directions (Fig. 2). While early diagnosis is helpful, biphasic or repeated biphasic models of sepsis make it difficult to predict mortality and prognosis based on initial biomarker levels. Nevertheless, the ideal biomarkers could play a role in sepsis screening, early diagnosis, risk stratification, critical assessment, and prognosis prediction [19, 20], which can improve outcomes (Table 1). This review will discuss the major measurable sepsis biomarkers that have been proposed for clinical use.
Table 1.
Characteristics of ideal sepsis biomarkers
1. Markers for early response to sepsis
The traditional sepsis model is the immune response activated when TLR expressed on the macrophage recognizes LPS in cell walls of gram-negative bacteria. This is an example of pattern recognition receptors (PRR) and pathogen-associated molecular patterns (PAMP). This recognition stimulates secretion of proinflammatory cytokines, such as TNF-α, IL-1β, and IL-6. Various inflammatory cytokines and LPS have therefore been studied as sepsis biomarkers.
1) Cytokines and chemokines
TNF-α, IL-1β, and IL-6 are cytokines responsible for mediation of the initial innate immune system response to injury or infection. These proinflammatory cytokines contribute to fever, activate endothelial cells, attract circulating polymorphonuclear cells (PMNs), and enter the circulatory system. Studies have demonstrated increased blood cytokine levels in patients with sepsis. However, levels of these cytokines also increase after trauma, surgery, stroke, or with autoimmune diseases. Use of these inflammatory cytokines to diagnosis sepsis is difficult because they are nonspecific and unable to differentiate infection from inflammation. TNF-α and IL-6 levels have been reported to be related to organ damage and mortality, making them potentially useful prognosis predictors [21, 22, 23]. However, a clinical trial of pretreatment with polyclonal ovine anti-TNF fragment antigen binding fragments (CytoFab) showed no difference in 28-day mortality [24, 25]. The conflicting reports could be explained by the short half-life (the half-life of TNF, for example, is 17 minutes) and earlier peak concentration of proinflammatory cytokines than other biomarkers. IL-1β levels are not elevated to the same degree as TNF. Therefore, neither TNF nor IL-1β has proven to be useful as major biomarkers of sepsis. It is difficult to translate certain clinical condition into particular cytokine profile [26], which could be caused by and is the result of complex inflammatory responses. Recent studies have proposed that measurement of multiple cytokines correlates well with disease severity and prognosis [26, 27, 28]. Combined biomarkers will be addressed later.
2) Lipopolysaccharide-binding protein
LPS-binding protein (LBP), mainly synthesized in the liver, is a polypeptide that binds LPS. The LPS-LBP complex initiates signal transduction according to LBP level. This complex complex has a dual action, enhancing and inhibiting LPS signaling at low and higher levels, respectively [29]. Serum LBP level increases several-fold in sepsis, making it useful for diagnosis [30, 31]. It may also be effective as a predictive marker for disease severity and outcome [32, 33]. However, LPS and LBP levels are affected by administration of antibiotics and generally do not correlate to the clinical course of sepsis [34]. Therefore, it is of limited use as a sepsis biomarker.
2. Markers for late response to sepsis
TNF-α and IL-1β are released within minutes of exposure to LPS. In the late 1990s, investigators found that LPS-treated mice died after serum TNF-α and IL-1β returned to basal levels, suggesting that mediators other than TNF-α might contribute to death. There are two well-known inflammatory mediators, high-mobility group box 1 (HMGB1) protein and macrophage migration inhibitory factor (MIF), which are important in late phase of severe infections.
1) High-mobility group box 1 protein
HMGB1 is a cytoplasmic and nuclear protein that is undetectable in healthy subjects. It is released by activated monocytes or necrotic tissues during infection or injury. This proinflammatory cytokine reaches detectable levels after 8-12 hours and plateaus after 18-32 hours. Plasma HMGB1 concentration has been shown to increase in patients with severe sepsis and septic shock and is correlated with the degree of organ failure [35, 36]. In a prospective study, HMGB1 measurements on day 3 discriminated survivors from non-survivors with a sensitivity and specificity of 66% and 67%, respectively. HMGB1 levels greater than 4 ng/mL on day 3 were associated with a 5.5-fold increased risk of death (95% confidence interval [CI]: 1.3-23.6) [37].
2) Macrophage migration inhibitory factor
The other "late" proinflammatory molecule, MIF normally circulates at low levels of 2-10 ng/mL [38]. Plasma MIF concentration increases during infection and very high levels have been found in cases with severe sepsis and septic shock [39]. A recent study concluded that high MIF levels serve as an early indicator of poor outcome in sepsis [40]. These results imply that late mediators such as HMGB1 and MIF could predict sepsis prognosis.
3. C-reactive protein
Tillet & Francis first discovered C-reactive protein (CRP) in a patient with lobar pneumonia in 1930. It was identified as a protein responsible for precipitating C polysaccharide during the acute phase of Streptococcus pneumonia infection [41]. CRP was also found in patients with endocarditis or rheumatic fever. Its response is stronger in acutely ill patients; levels decrease as patients recover. These characteristics make CRP a member of the class of acute-phase reactants. CRP is an old biomarker used most commonly in clinical settings. It is a nonspecific marker of inflammation that also increases after surgery, burns, myocardial infarctions, and rheumatic diseases [42]. The sensitivity and specificity of CRP as a marker for bacterial infections are 68-92% and 40-67%, respectively [43, 44, 45, 46]. Its low specificity and inability to differentiate bacterial infections from noninfectious causes of inflammation makes CRP of limited diagnostic value. However, CRP shows promise for evaluating sepsis severity and prognosis. CRP plasma levels have been shown to correlate with the severity of infection [47]. A rapid decrease in CRP levels has been reported to correlate with good response to initial antimicrobial therapy in septic patients [48]. CRP is a useful biomarker to monitor treatment response. However, hasty interpretation or antibiotic guidance within 1-2 days after starting empirical antibiotic treatment is problematic in many clinical situations. Clinicians cannot interpret changes in CRP levels without considering the kinetics of this marker.
4. Procalcitonin
Procalcitonin (PCT) is a precursor of calcitonin, a calcium regulatory hormone secreted from thyroid tissue in healthy individuals. In infectious conditions, PCT is released from nearly all tissues including lung, liver, kidney, pancreas, spleen, colon, and adipose tissues. In 1993, PCT was first described as a marker elevated in bacterial infections [49]. In 2008, PCT was proposed as an adjunctive diagnostic marker to differentiate acute bacterial infection from other inflammatory states by the American College of Critical Care Medicine and the Infectious Diseases Society of America [50]. In a systematic review and meta-analysis, PCT was found to be more specific (specificity 81% [95% CI: 67-90%]) than CRP (67% [95% CI: 56-77%]) for differentiating bacterial infection among hospitalized patients [46]. The cutoff median PCT value in this meta-analysis was 1.1 ng/mL (interquartile range: 0.5-2.0 ng/mL). PCT cutoffs for diagnosis of sepsis or guidance of antibiotic choice have not yet been fully determined; the sensitivity and specificity of this marker for diagnosis of sepsis are affected by different cutoff values. PCT values need to be further evaluated according to different sites of infection, hosts, and pathogens. Another recent meta-analysis showed that PCT is a useful marker for early diagnosis of sepsis in critically ill patients, with sensitivity and specificity of 77% (95% CI: 72-81%) and 79% (95% CI: 74-84%), respectively [51]. PCT levels are also elevated after surgery, cardiogenic shock, heat shock, acute graft-versus-host disease, and immunotherapy such as granulocyte transfusion, which could limit its usefulness as a sepsis biomarker [52, 53]. PCT has also drawn attention because it can be used for guidance of antibiotic stewardship to reduce inappropriate use of antibiotics [54]. However, many experts recommend that PCT-guided decision-making should be an adjunctive method based on consideration of the patient's clinical course.
5. Lactate
Serum lactate levels can reflect tissue hypoperfusion and anaerobic metabolism in severe sepsis and septic shock. At a cellular level, energy production depends on glucose and oxygen metabolism. Glycolysis converts glucose to pyruvate and yields 2 adenosine triphosphates (ATPs). Pyruvate then enters the Krebs cycle, which produces more ATPs. However, in hypoxic circumstances, pyruvate is instead converted to lactate. Elevated lactate levels and lactate-to-pyruvate ratios result mostly from increased glycolysis and lactate production as well as limited tissue oxygenation. Elevated levels are also related to impaired hepatic lactate clearance and mitochondrial dysfunction [20]. Several studies have demonstrated that elevated lactate levels are related to mortality in patients with sepsis [55, 56, 57, 58]. In a retrospective study of critically ill patients, serum lactate levels greater than 2 mmol/L on admission were associated with a 1.94-10.89-fold increased mortality compared to levels below 2 mmol/L [59]. In a large study of 1,278 patients with infections, those with lactate levels above 4 mmol/L had higher in-hospital mortality rates than patients with lactate levels less than 2.5 mmol/L (28.4% vs. 4.9%) [57]. Another study has reported that sustained hyperlactatemia is predictive of in-hospital mortality [60]. In contrast, however, early lactate clearance was associated with improved outcomes in patients with severe sepsis and septic shock [61]. A recent systematic review further confirmed the utility of monitoring serial blood lactate and its value as a predictive marker of in-hospital mortality [58]. Recently, data from a retrospective study by the Vasopressin Septic Shock Trial and a single-center septic shock cohort (St. Paul's Hospital cohort) have suggested that even minimal increases in arterial lactate concentration within the reference range (1.4-2.3 mmol/L) may predict 28-day mortality (sensitivity and specificity of 86% and 27%, respectively). Furthermore, the data suggested that patients with lactate levels below 1.4 mmol/L might benefit from vasopressin infusion [56]. Therefore, lactate screening and monitoring may be a valuable tool for risk stratification and to predict sepsis outcome.
6. Mid-regional proadrenomedullin
Like PCT, proadrenomedullin (proADM) is a kind of "hormokine" that encompasses the cytokine-like behavior of hormones during inflammation and infections. Adrenomedullin (ADM) is a 52-amino-acid peptide produced by the adrenal medulla. ADM is produced during physiological stress and has various functions including vasodilation and anti-inflammatory and antimicrobial effects [62]. Plasma ADM concentration and ADM gene expression increases in patients with sepsis [63]. However, ADM is rapidly cleared from the circulation, making measurements unreliable. Therefore, instead of ADM, serum quantification of the mid-regional fragment of proADM has been studied. Recent clinical data have shown that circulating mid-regional proADM levels are significantly higher in patients with sepsis than in patients with systemic inflammatory response syndrome (SIRS) [64]. A recent study of febrile patients with hematologic malignancies reported that proADM could predict localized bacterial infections and differentiate sepsis from SIRS [65]. In addition, proADM is responsible for hypotension associated with severe sepsis, which has been proposed as a good marker for risk assessment and predicting sepsis prognosis [64, 66]. If further data support these findings on the predictive value of proADM, it could be useful as both a prognostic marker and a diagnostic marker for early stages of localized infections.
7. Cell surface markers and soluble receptors
1) CD64
CD64 is a membrane glycoprotein with increased expression in patients with bacterial infections. CD64 expression increases hours after activation of innate immunity; it is not expressed by PMN in healthy individuals. Therefore, CD64 expression can reflect very early stages of infection and help to both make early diagnosis and predict prognosis. The CD64 index has been suggested to be predictive of positive bacterial cultures and a useful test for management of sepsis and other significant bacterial infections [67]. Another study demonstrated that the CD64 index is higher in febrile adult patients with bacterial infections, with a sensitivity of 87% (95% CI: 79-92%), and that high CD64 expression is related to survival [68]. In contrast, it has been reported that CD64 indices greater than 2.2 are specific (89% specificity [95% CI: 83-94%]) but less sensitive (63% sensitivity [95% CI: 55-71%]) to predict bacterial infections in critically ill patients [69]. A systematic review and meta-analysis concluded that CD64 could be a marker for bacterial infection with a pooled sensitivity and specificity of 79% (95% CI: 70-86%) and 91% (95% CI: 85-95%), respectively. However, because published studies have low methodological quality, further studies are needed to verify these findings [70].
2) Soluble triggering receptor expressed on myeloid cells 1
Soluble triggering receptor expressed on myeloid cell 1 (sTREM-1) is a soluble form of TREM-1, a glycopeptide receptor expressed on the surface of myeloid cells such as PMNs, mature monocytes, and macrophages. TREM-1 expression increases in bacterial or fungal infections [71, 72, 73]. A prospective study by Gibot et al. suggested that the sensitivity and specificity of sTREM-1 for diagnosis of sepsis are comparable to that of CRP and PCT [74, 75]. A meta-analysis reported that the sensitivity and specificity of sTREM-1 to diagnose bacterial infections were 82% (95% CI: 68-90%) and 86% (95% CI: 77-91%), respectively [76]. Another recent meta-analysis showed that plasma sTREM-1 had only moderate diagnostic performance to differentiate sepsis from SIRS [77]. A prospective study at a single center in Korea reported that sTREM-1 levels on admission were independently significant for survival in patients with severe sepsis [78]. In addition, rapid decrease of sTREM-1 is correlated with better outcome [72]. Therefore, sTREM-1 may be useful for sepsis diagnosis or predicting sepsis prognosis. The usefulness of sTREM-1 as a biomarker requires further evaluation in clinical settings either measured alone or combined with other biomarkers.
3) Soluble urokinase plasminogen activator receptor
First described in 1990, urokinase plasminogen activator receptor (uPAR) is a surface signaling receptor expressed on most leukocytes [79]. uPAR was originally thought to assist directional invasion of migrating cells, but is now known to be involved in multiple immunological functions including cellular adhesion, differentiation, proliferation and angiogenesis, as well as migration [80]. During inflammatory processes, uPAR is cleaved from the cell surface by proteases and released as soluble uPAR (suPAR). It is measurable in blood and body fluids including urine, cerebrospinal fluid, bronchial washing fluid, and saliva. suPAR plasma levels reflect immune activation in response to bacterial or viral infection, cancer, burns, and rheumatic diseases. suPAR levels are significantly higher in patients with sepsis than those without and also higher in critically ill patients than control patients [81]. However, recent studies have demonstrated that suPAR has a lower diagnostic value for sepsis (areas under receiver operating characteristic curves [AUC-ROC] of 0.62) than CRP or PCT [82, 83, 84]. Several studies have suggested suPAR to be an informative marker for severity of sepsis [81, 84, 85, 86, 87]. In a prospective study of 543 acutely-ill patients, baseline suPAR levels were significantly associated with 30 day- and 90 day-mortality after adjusting for age, CRP, and Charlson's comorbidity index [86]. In a recent systematic review, suPAR was superior to other biomarkers, including CRP, PCT, and sTREM-1 for predicting prognosis [84]. Overall, suPAR might have better prognostic value to predict mortality instead of diagnosing sepsis.
8. Angiopoietin
Angiopoietin (Ang)-1 and -2 are endothelial-derived vascular growth factors that play opposing roles during sepsis. Ang-1 stabilizes the endothelium, whereas Ang-2 facilitates loss of endothelial integrity and vascular leakage. Ang-1 or Ang-2 activates the transmembrane endothelial tyrosine kinase Tie2, which mediates the quiescent, healthy state of blood vessels [88]. Ang-2 plays a crucial role in induction of inflammation [88, 89]. Elevated levels of circulating Ang-2 are associated with sepsis with multi-organ dysfunction, which is indicative of impaired vascular endothelial integrity. A cohort study revealed that elevated Ang-1 and lower Ang-2 levels were observed in sepsis survivors [90]. The endothelium and Ang-Tie2 receptor ligand system have been the recent focus of ongoing sepsis studies.
9. Combined biomarkers and sepsis scoring systems
We have discussed several sepsis biomarkers. Numerous biomarkers have been evaluated for clinical use in sepsis, with moderate to good sensitivity and specificity for diagnosis and prognosis. However, the results of measuring a single biomarker are inconclusive in clinical settings. Owing to this limitation, combination approaches measuring multiple biomarkers have recently been introduced. "Scoring systems" have also been developed, which use both clinical and laboratory markers [28, 91, 92]. In 2003, the infection probability score (IPS) was introduced to assess the probability of infection in critically ill patients. The IPS ranges from 0 to 26 points, and includes patient body temperature (0-2 points), heart rate (0-1 points), respiratory rate (0-1 points), white blood cell counts (0-3 points), CRP (0-6 points), and sepsis-related organ failure assessment score (0-2 points). The AUC-ROC of IPS was 0.82 for predicting the probability of infection. Patients with <14 points have only a 10% risk of infection [93]. Several clinical examples of combinations of biomarkers and scoring for sepsis are shown in Table 2 [27, 31, 44, 82, 91, 92, 94, 95].
Table 2.
Several clinical examples of combined sepsis biomarkers
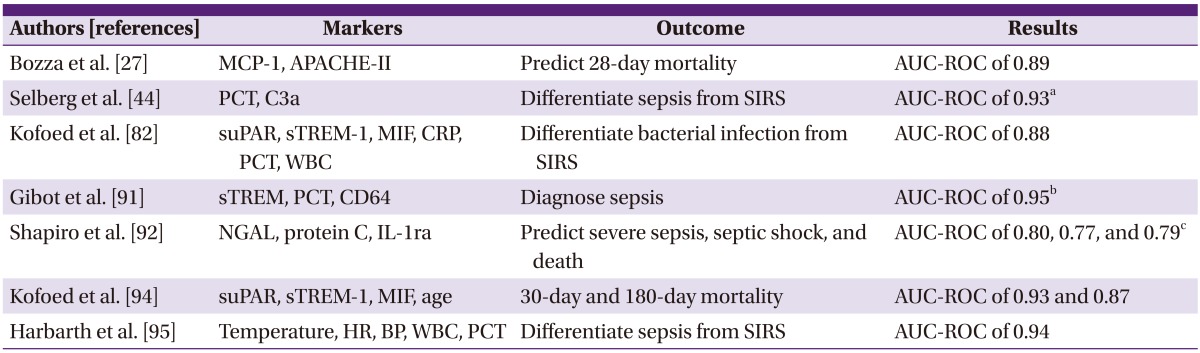
ap (sepsis) = e(-28.6106 + 0.8912 × ln(PCT) + 4.3571 ×ln(C3a)/[1 + e(-28.6106 + 0.8912 × ln(PCT) + 4.3571 × ln(C3a)].
b"bioscore" was calculated by scoring as 0 or 1 values below or above each threshold value for sTREM, PCT, and CD64 index.
cSepsis Score = probability of severe sepsis = [e(raw score)/1 + e(raw score)] × 100; Raw Score = -8.7 + 0.63 (NGAL quartile) + 0.41 (IL-1ra quartile) + 0.50 (protein C quartile) APACHE-II, acute physiology and chronic health evaluation II; AUC-ROC, areas under receiver operating characteristic curves; BP, blood pressure; CD, cluster of differentiation; CRP, C-reactive protein; C3a, complement 3a; HR, heart rate; IL-1ra, interleukin-1 receptor antagonist; MCP, monocyte chemoattractant protein; MIF, macrophage migration inhibitory factor; NGAL, neutrophil gelatinase-associated lipocalin; PCT, procalcitonin; sTREM-1, soluble triggering receptor expressed on myeloid cell-1, suPAR; soluble form of urokinase-type plasminogen activator receptor, WBC; white blood cell.
Combined biomarkers and inclusion of sepsis scoring systems showed better AUC-ROC values than single biomarkers. Theoretically, combining multiple markers can improve diagnostic and prognostic values, because sepsis is composed of multiple immune responses with various changes in cytokines and biomarkers. However, which and how many combinations of biomarkers are most informative have not yet been investigated for use as a high-throughput technology. Cost-effectiveness and comprehensive clinical interpretation must also be evaluated.
Conclusions
Biomarkers are useful for early diagnosis of sepsis, to predict outcome, and to guide choice of antibiotic therapy. In these modern times, clinicians encounter the laboratory results on a daily basis. Therefore, proper interpretation and wise use of biomarkers are necessary. Combination approaches of biomarkers with new techniques needs to be further evaluated.
References
- 1.Levy MM, Dellinger RP, Townsend SR, Linde-Zwirble WT, Marshall JC, Bion J, Schorr C, Artigas A, Ramsay G, Beale R, Parker MM, Gerlach H, Reinhart K, Silva E, Harvey M, Regan S, Angus DC. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med. 2010;36:222–231. doi: 10.1007/s00134-009-1738-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ranieri VM, Thompson BT, Barie PS, Dhainaut JF, Douglas IS, Finfer S, Gårdlund B, Marshall JC, Rhodes A, Artigas A, Payen D, Tenhunen J, Al-Khalidi HR, Thompson V, Janes J, Macias WL, Vangerow B, Williams MD PROWESS-SHOCK Study Group. Drotrecogin alfa (activated) in adults with septic shock. N Engl J Med. 2012;366:2055–2064. doi: 10.1056/NEJMoa1202290. [DOI] [PubMed] [Google Scholar]
- 3.Vincent JL. The rise and fall of drotrecogin alfa (activated) Lancet Infect Dis. 2012;12:649–651. doi: 10.1016/S1473-3099(12)70175-5. [DOI] [PubMed] [Google Scholar]
- 4.Guntupalli K, Dean N, Morris PE, Bandi V, Margolis B, Rivers E, Levy M, Lodato RF, Ismail PM, Reese A, Schaumberg JP, Malik R, Dellinger RP TLF LF-0801 Investigator Group. A phase 2 randomized, double-blind, placebo-controlled study of the safety and efficacy of talactoferrin in patients with severe sepsis. Crit Care Med. 2013;41:706–716. doi: 10.1097/CCM.0b013e3182741551. [DOI] [PubMed] [Google Scholar]
- 5.McCulloh R, Opal SM. Human recombinant lactoferrin for sepsis: too good to be true? Crit Care Med. 2013;41:908–909. doi: 10.1097/CCM.0b013e3182770fd6. [DOI] [PubMed] [Google Scholar]
- 6.Opal SM, Laterre PF, Francois B, LaRosa SP, Angus DC, Mira JP, Wittebole X, Dugernier T, Perrotin D, Tidswell M, Jauregui L, Krell K, Pachl J, Takahashi T, Peckelsen C, Cordasco E, Chang CS, Oeyen S, Aikawa N, Maruyama T, Schein R, Kalil AC, Van Nuffelen M, Lynn M, Rossignol DP, Gogate J, Roberts MB, Wheeler JL, Vincent JL ACCESS Study Group. Effect of eritoran, an antagonist of MD2-TLR4, on mortality in patients with severe sepsis: the ACCESS randomized trial. JAMA. 2013;309:1154–1162. doi: 10.1001/jama.2013.2194. [DOI] [PubMed] [Google Scholar]
- 7.Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, Osborn TM, Nunnally ME, Townsend SR, Reinhart K, Kleinpell RM, Angus DC, Deutschman CS, Machado FR, Rubenfeld GD, Webb SA, Beale RJ, Vincent JL, Moreno R Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580–637. doi: 10.1097/CCM.0b013e31827e83af. [DOI] [PubMed] [Google Scholar]
- 8.Choi JH. Recent evidences of sepsis treatment. Infect Chemother. 2008;40:67–75. [Google Scholar]
- 9.Sands KE, Bates DW, Lanken PN, Graman PS, Hibberd PL, Kahn KL, Parsonnet J, Panzer R, Orav EJ, Snydman DR, Black E, Schwartz JS, Moore R, Johnson BL, Jr, Platt R Academic Medical Center Consortium Sepsis Project Working Group. Epidemiology of sepsis syndrome in 8 academic medical centers. JAMA. 1997;278:234–240. [PubMed] [Google Scholar]
- 10.Vincent JL, Sakr Y, Sprung CL, Ranieri VM, Reinhart K, Gerlach H, Moreno R, Carlet J, Le Gall JR, Payen D Sepsis Occurrence in Acutely Ill Patients Investigators. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med. 2006;34:344–353. doi: 10.1097/01.ccm.0000194725.48928.3a. [DOI] [PubMed] [Google Scholar]
- 11.Hotchkiss RS, Karl IE. The pathophysiology and treatment of sepsis. N Engl J Med. 2003;348:138–150. doi: 10.1056/NEJMra021333. [DOI] [PubMed] [Google Scholar]
- 12.Hotchkiss RS, Monneret G, Payen D. Immunosuppression in sepsis: a novel understanding of the disorder and a new therapeutic approach. Lancet Infect Dis. 2013;13:260–268. doi: 10.1016/S1473-3099(13)70001-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Unsinger J, McGlynn M, Kasten KR, Hoekzema AS, Watanabe E, Muenzer JT, McDonough JS, Tschoep J, Ferguson TA, McDunn JE, Morre M, Hildeman DA, Caldwell CC, Hotchkiss RS. IL-7 promotes T cell viability, trafficking, and functionality and improves survival in sepsis. J Immunol. 2010;184:3768–3779. doi: 10.4049/jimmunol.0903151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Meisel C, Schefold JC, Pschowski R, Baumann T, Hetzger K, Gregor J, Weber-Carstens S, Hasper D, Keh D, Zuckermann H, Reinke P, Volk HD. Granulocyte-macrophage colony-stimulating factor to reverse sepsis-associated immunosuppression: a double-blind, randomized, placebo-controlled multicenter trial. Am J Respir Crit Care Med. 2009;180:640–648. doi: 10.1164/rccm.200903-0363OC. [DOI] [PubMed] [Google Scholar]
- 15.Boomer JS, To K, Chang KC, Takasu O, Osborne DF, Walton AH, Bricker TL, Jarman SD, 2nd, Kreisel D, Krupnick AS, Srivastava A, Swanson PE, Green JM, Hotchkiss RS. Immunosuppression in patients who die of sepsis and multiple organ failure. JAMA. 2011;306:2594–2605. doi: 10.1001/jama.2011.1829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: preferred definitions and conceptual framework. Clin Pharmacol Ther. 2001;69:89–95. doi: 10.1067/mcp.2001.113989. [DOI] [PubMed] [Google Scholar]
- 17.Pierrakos C, Vincent JL. Sepsis biomarkers: a review. Crit Care. 2010;14:R15. doi: 10.1186/cc8872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Calvano SE, Xiao W, Richards DR, Felciano RM, Baker HV, Cho RJ, Chen RO, Brownstein BH, Cobb JP, Tschoeke SK, Miller-Graziano C, Moldawer LL, Mindrinos MN, Davis RW, Tompkins RG, Lowry SF Inflamm and Host Response to Injury Large Scale Collab. Res. Program. A network-based analysis of systemic inflammation in humans. Nature. 2005;437:1032–1037. doi: 10.1038/nature03985. [DOI] [PubMed] [Google Scholar]
- 19.Marshall JC, Reinhart K International Sepsis Forum. Biomarkers of sepsis. Crit Care Med. 2009;37:2290–2298. doi: 10.1097/CCM.0b013e3181a02afc. [DOI] [PubMed] [Google Scholar]
- 20.Samraj RS, Zingarelli B, Wong HR. Role of biomarkers in sepsis care. Shock. 2013;40:358–365. doi: 10.1097/SHK.0b013e3182a66bd6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Pettilä V, Hynninen M, Takkunen O, Kuusela P, Valtonen M. Predictive value of procalcitonin and interleukin 6 in critically ill patients with suspected sepsis. Intensive Care Med. 2002;28:1220–1225. doi: 10.1007/s00134-002-1416-1. [DOI] [PubMed] [Google Scholar]
- 22.Oberholzer A, Souza SM, Tschoeke SK, Oberholzer C, Abouhamze A, Pribble JP, Moldawer LL. Plasma cytokine measurements augment prognostic scores as indicators of outcome in patients with severe sepsis. Shock. 2005;23:488–493. [PubMed] [Google Scholar]
- 23.Pinsky MR, Vincent JL, Deviere J, Alegre M, Kahn RJ, Dupont E. Serum cytokine levels in human septic shock. Relation to multiple-system organ failure and mortality. Chest. 1993;103:565–575. doi: 10.1378/chest.103.2.565. [DOI] [PubMed] [Google Scholar]
- 24.Qiu P, Cui X, Barochia A, Li Y, Natanson C, Eichacker PQ. The evolving experience with therapeutic TNF inhibition in sepsis: considering the potential influence of risk of death. Expert Opin Investig Drugs. 2011;20:1555–1564. doi: 10.1517/13543784.2011.623125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Rice TW, Wheeler AP, Morris PE, Paz HL, Russell JA, Edens TR, Bernard GR. Safety and efficacy of affinity-purified, anti-tumor necrosis factor-alpha, ovine fab for injection (CytoFab) in severe sepsis. Crit Care Med. 2006;34:2271–2281. doi: 10.1097/01.CCM.0000230385.82679.34. [DOI] [PubMed] [Google Scholar]
- 26.Lvovschi V, Arnaud L, Parizot C, Freund Y, Juillien G, Ghillani-Dalbin P, Bouberima M, Larsen M, Riou B, Gorochov G, Hausfater P. Cytokine profiles in sepsis have limited relevance for stratifying patients in the emergency department: a prospective observational study. PLoS One. 2011;6:e28870. doi: 10.1371/journal.pone.0028870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bozza FA, Salluh JI, Japiassu AM, Soares M, Assis EF, Gomes RN, Bozza MT, Castro-Faria-Neto HC, Bozza PT. Cytokine profiles as markers of disease severity in sepsis: a multiplex analysis. Crit Care. 2007;11:R49. doi: 10.1186/cc5783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Andaluz-Ojeda D, Bobillo F, Iglesias V, Almansa R, Rico L, Gandía F, Resino S, Tamayo E, de Lejarazu RO, Bermejo-Martin JF. A combined score of pro- and anti-inflammatory interleukins improves mortality prediction in severe sepsis. Cytokine. 2012;57:332–336. doi: 10.1016/j.cyto.2011.12.002. [DOI] [PubMed] [Google Scholar]
- 29.Jerala R. Structural biology of the LPS recognition. Int J Med Microbiol. 2007;297:353–363. doi: 10.1016/j.ijmm.2007.04.001. [DOI] [PubMed] [Google Scholar]
- 30.Zweigner J, Gramm HJ, Singer OC, Wegscheider K, Schumann RR. High concentrations of lipopolysaccharide-binding protein in serum of patients with severe sepsis or septic shock inhibit the lipopolysaccharide response in human monocytes. Blood. 2001;98:3800–3808. doi: 10.1182/blood.v98.13.3800. [DOI] [PubMed] [Google Scholar]
- 31.Gaïni S, Koldkjaer OG, Pedersen C, Pedersen SS. Procalcitonin, lipopolysaccharide-binding protein, interleukin-6 and C-reactive protein in community-acquired infections and sepsis: a prospective study. Crit Care. 2006;10:R53. doi: 10.1186/cc4866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Opal SM, Scannon PJ, Vincent JL, White M, Carroll SF, Palardy JE, Parejo NA, Pribble JP, Lemke JH. Relationship between plasma levels of lipopolysaccharide (LPS) and LPS-binding protein in patients with severe sepsis and septic shock. J Infect Dis. 1999;180:1584–1589. doi: 10.1086/315093. [DOI] [PubMed] [Google Scholar]
- 33.Sakr Y, Burgett U, Nacul FE, Reinhart K, Brunkhorst F. Lipopolysaccharide binding protein in a surgical intensive care unit: a marker of sepsis? Crit Care Med. 2008;36:2014–2022. doi: 10.1097/CCM.0b013e31817b86e3. [DOI] [PubMed] [Google Scholar]
- 34.Choi JH, Shin WS. Pathogenesis of sepsis and concepts of immunotherapy. Korean J Infect Dis. 2000;32:148–157. [Google Scholar]
- 35.Sundén-Cullberg J, Norrby-Teglund A, Rouhiainen A, Rauvala H, Herman G, Tracey KJ, Lee ML, Andersson J, Tokics L, Treutiger CJ. Persistent elevation of high mobility group box-1 protein (HMGB1) in patients with severe sepsis and septic shock. Crit Care Med. 2005;33:564–573. doi: 10.1097/01.ccm.0000155991.88802.4d. [DOI] [PubMed] [Google Scholar]
- 36.Hatada T, Wada H, Nobori T, Okabayashi K, Maruyama K, Abe Y, Uemoto S, Yamada S, Maruyama I. Plasma concentrations and importance of High Mobility Group Box protein in the prognosis of organ failure in patients with disseminated intravascular coagulation. Thromb Haemost. 2005;94:975–979. doi: 10.1160/TH05-05-0316. [DOI] [PubMed] [Google Scholar]
- 37.Gibot S, Massin F, Cravoisy A, Barraud D, Nace L, Levy B, Bollaert PE. High-mobility group box 1 protein plasma concentrations during septic shock. Intensive Care Med. 2007;33:1347–1353. doi: 10.1007/s00134-007-0691-2. [DOI] [PubMed] [Google Scholar]
- 38.Petrovsky N, Socha L, Silva D, Grossman AB, Metz C, Bucala R. Macrophage migration inhibitory factor exhibits a pronounced circadian rhythm relevant to its role as a glucocorticoid counter-regulator. Immunol Cell Biol. 2003;81:137–143. doi: 10.1046/j.0818-9641.2002.01148.x. [DOI] [PubMed] [Google Scholar]
- 39.Calandra T, Echtenacher B, Roy DL, Pugin J, Metz CN, Hultner L, Heumann D, Männel D, Bucala R, Glauser MP. Protection from septic shock by neutralization of macrophage migration inhibitory factor. Nat Med. 2000;6:164–170. doi: 10.1038/72262. [DOI] [PubMed] [Google Scholar]
- 40.Bozza FA, Gomes RN, Japiassú AM, Soares M, Castro-Faria-Neto HC, Bozza PT, Bozza MT. Macrophage migration inhibitory factor levels correlate with fatal outcome in sepsis. Shock. 2004;22:309–313. doi: 10.1097/01.shk.0000140305.01641.c8. [DOI] [PubMed] [Google Scholar]
- 41.Tillett WS, Francis T. Serological reactions in pneumonia with a non-protein somatic fraction of pneumococcus. J Exp Med. 1930;52:561–571. doi: 10.1084/jem.52.4.561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Vincent JL, Donadello K, Schmit X. Biomarkers in the critically ill patient: C-reactive protein. Crit Care Clin. 2011;27:241–251. doi: 10.1016/j.ccc.2010.12.010. [DOI] [PubMed] [Google Scholar]
- 43.Müller B, Becker KL, Schächinger H, Rickenbacher PR, Huber PR, Zimmerli W, Ritz R. Calcitonin precursors are reliable markers of sepsis in a medical intensive care unit. Crit Care Med. 2000;28:977–983. doi: 10.1097/00003246-200004000-00011. [DOI] [PubMed] [Google Scholar]
- 44.Selberg O, Hecker H, Martin M, Klos A, Bautsch W, Köhl J. Discrimination of sepsis and systemic inflammatory response syndrome by determination of circulating plasma concentrations of procalcitonin, protein complement 3a, and interleukin-6. Crit Care Med. 2000;28:2793–2798. doi: 10.1097/00003246-200008000-00019. [DOI] [PubMed] [Google Scholar]
- 45.Suprin E, Camus C, Gacouin A, Le Tulzo Y, Lavoue S, Feuillu A, Thomas R. Procalcitonin: a valuable indicator of infection in a medical ICU? Intensive Care Med. 2000;26:1232–1238. doi: 10.1007/s001340000580. [DOI] [PubMed] [Google Scholar]
- 46.Simon L, Gauvin F, Amre DK, Saint-Louis P, Lacroix J. Serum procalcitonin and C-reactive protein levels as markers of bacterial infection: a systematic review and meta-analysis. Clin Infect Dis. 2004;39:206–217. doi: 10.1086/421997. [DOI] [PubMed] [Google Scholar]
- 47.Póvoa P, Coelho L, Almeida E, Fernandes A, Mealha R, Moreira P, Sabino H. C-reactive protein as a marker of infection in critically ill patients. Clin Microbiol Infect. 2005;11:101–108. doi: 10.1111/j.1469-0691.2004.01044.x. [DOI] [PubMed] [Google Scholar]
- 48.Schmit X, Vincent JL. The time course of blood C-reactive protein concentrations in relation to the response to initial antimicrobial therapy in patients with sepsis. Infection. 2008;36:213–219. doi: 10.1007/s15010-007-7077-9. [DOI] [PubMed] [Google Scholar]
- 49.Assicot M, Gendrel D, Carsin H, Raymond J, Guilbaud J, Bohuon C. High serum procalcitonin concentrations in patients with sepsis and infection. Lancet. 1993;341:515–518. doi: 10.1016/0140-6736(93)90277-N. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.O'Grady NP1, Barie PS, Bartlett JG, Bleck T, Carroll K, Kalil AC, Linden P, Maki DG, Nierman D, Pasculle W, Masur H American College of Critical Care Medicine; Infectious Diseases Society of America. Guidelines for evaluation of new fever in critically ill adult patients: 2008 update from the American College of Critical Care Medicine and the Infectious Diseases Society of America. Crit Care Med. 2008;36:1330–1349. doi: 10.1097/CCM.0b013e318169eda9. [DOI] [PubMed] [Google Scholar]
- 51.Wacker C, Prkno A, Brunkhorst FM, Schlattmann P. Procalcitonin as a diagnostic marker for sepsis: a systematic review and meta-analysis. Lancet Infect Dis. 2013;13:426–435. doi: 10.1016/S1473-3099(12)70323-7. [DOI] [PubMed] [Google Scholar]
- 52.Reinhart K, Meisner M. Biomarkers in the critically ill patient: procalcitonin. Crit Care Clin. 2011;27:253–263. doi: 10.1016/j.ccc.2011.01.002. [DOI] [PubMed] [Google Scholar]
- 53.Schuetz P, Affolter B, Hunziker S, Winterhalder C, Fischer M, Balestra GM, Hunziker P, Marsch S. Serum procalcitonin, C-reactive protein and white blood cell levels following hypothermia after cardiac arrest: a retrospective cohort study. Eur J Clin Invest. 2010;40:376–381. doi: 10.1111/j.1365-2362.2010.02259.x. [DOI] [PubMed] [Google Scholar]
- 54.Kopterides P, Siempos II, Tsangaris I, Tsantes A, Armaganidis A. Procalcitonin-guided algorithms of antibiotic therapy in the intensive care unit: a systematic review and meta-analysis of randomized controlled trials. Crit Care Med. 2010;38:2229–2241. doi: 10.1097/CCM.0b013e3181f17bf9. [DOI] [PubMed] [Google Scholar]
- 55.Mikkelsen ME, Miltiades AN, Gaieski DF, Goyal M, Fuchs BD, Shah CV, Bellamy SL, Christie JD. Serum lactate is associated with mortality in severe sepsis independent of organ failure and shock. Crit Care Med. 2009;37:1670–1677. doi: 10.1097/CCM.0b013e31819fcf68. [DOI] [PubMed] [Google Scholar]
- 56.Wacharasint P, Nakada TA, Boyd JH, Russell JA, Walley KR. Normal-range blood lactate concentration in septic shock is prognostic and predictive. Shock. 2012;38:4–10. doi: 10.1097/SHK.0b013e318254d41a. [DOI] [PubMed] [Google Scholar]
- 57.Shapiro NI, Howell MD, Talmor D, Nathanson LA, Lisbon A, Wolfe RE, Weiss JW. Serum lactate as a predictor of mortality in emergency department patients with infection. Ann Emerg Med. 2005;45:524–528. doi: 10.1016/j.annemergmed.2004.12.006. [DOI] [PubMed] [Google Scholar]
- 58.Kruse O, Grunnet N, Barfod C. Blood lactate as a predictor for in-hospital mortality in patients admitted acutely to hospital: a systematic review. Scand J Trauma Resusc Emerg Med. 2011;19:74. doi: 10.1186/1757-7241-19-74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Khosravani H, Shahpori R, Stelfox HT, Kirkpatrick AW, Laupland KB. Occurrence and adverse effect on outcome of hyperlactatemia in the critically ill. Crit Care. 2009;13:R90. doi: 10.1186/cc7918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Claridge JA, Crabtree TD, Pelletier SJ, Butler K, Sawyer RG, Young JS. Persistent occult hypoperfusion is associated with a significant increase in infection rate and mortality in major trauma patients. J Trauma. 2000;48:8–14. doi: 10.1097/00005373-200001000-00003. discussion 14-5. [DOI] [PubMed] [Google Scholar]
- 61.Nguyen HB, Rivers EP, Knoblich BP, Jacobsen G, Muzzin A, Ressler JA, Tomlanovich MC. Early lactate clearance is associated with improved outcome in severe sepsis and septic shock. Crit Care Med. 2004;32:1637–1642. doi: 10.1097/01.ccm.0000132904.35713.a7. [DOI] [PubMed] [Google Scholar]
- 62.Linscheid P, Seboek D, Zulewski H, Keller U, Müller B. Autocrine/paracrine role of inflammation-mediated calcitonin gene-related peptide and adrenomedullin expression in human adipose tissue. Endocrinology. 2005;146:2699–2708. doi: 10.1210/en.2004-1424. [DOI] [PubMed] [Google Scholar]
- 63.Hinson JP, Kapas S, Smith DM. Adrenomedullin, a multifunctional regulatory peptide. Endocr Rev. 2000;21:138–167. doi: 10.1210/edrv.21.2.0396. [DOI] [PubMed] [Google Scholar]
- 64.Christ-Crain M, Morgenthaler NG, Struck J, Harbarth S, Bergmann A, Müller B. Mid-regional pro-adrenomedullin as a prognostic marker in sepsis: an observational study. Crit Care. 2005;9:R816–R824. doi: 10.1186/cc3885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Al Shuaibi M, Bahu RR, Chaftari AM, Al Wohoush I, Shomali W, Jiang Y, Debiane L, Raad S, Jabbour J, Al Akhrass F, Hachem RY, Raad I. Pro-adrenomedullin as a novel biomarker for predicting infections and response to antimicrobials in febrile patients with hematologic malignancies. Clin Infect Dis. 2013;56:943–950. doi: 10.1093/cid/cis1029. [DOI] [PubMed] [Google Scholar]
- 66.Suberviola B, Castellanos-Ortega A, Ruiz Ruiz A, Lopez-Hoyos M, Santibañez M. Hospital mortality prognostication in sepsis using the new biomarkers suPAR and proADM in a single determination on ICU admission. Intensive Care Med. 2013;39:1945–1952. doi: 10.1007/s00134-013-3056-z. [DOI] [PubMed] [Google Scholar]
- 67.Icardi M, Erickson Y, Kilborn S, Stewart B, Grief B, Scharnweber G. CD64 index provides simple and predictive testing for detection and monitoring of sepsis and bacterial infection in hospital patients. J Clin Microbiol. 2009;47:3914–3919. doi: 10.1128/JCM.00628-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Cid J, García-Pardo G, Aguinaco R, Sánchez R, Llorente A. Neutrophil CD64: diagnostic accuracy and prognostic value in patients presenting to the emergency department. Eur J Clin Microbiol Infect Dis. 2011;30:845–852. doi: 10.1007/s10096-011-1164-7. [DOI] [PubMed] [Google Scholar]
- 69.Gros A, Roussel M, Sauvadet E, Gacouin A, Marqué S, Chimot L, Lavoué S, Camus C, Fest T, Le Tulzo Y. The sensitivity of neutrophil CD64 expression as a biomarker of bacterial infection is low in critically ill patients. Intensive Care Med. 2012;38:445–452. doi: 10.1007/s00134-012-2483-6. [DOI] [PubMed] [Google Scholar]
- 70.Cid J, Aguinaco R, Sánchez R, García-Pardo G, Llorente A. Neutrophil CD64 expression as marker of bacterial infection: a systematic review and meta-analysis. J Infect. 2010;60:313–319. doi: 10.1016/j.jinf.2010.02.013. [DOI] [PubMed] [Google Scholar]
- 71.Bouchon A, Facchetti F, Weigand MA, Colonna M. TREM-1 amplifies inflammation and is a crucial mediator of septic shock. Nature. 2001;410:1103–1107. doi: 10.1038/35074114. [DOI] [PubMed] [Google Scholar]
- 72.Gibot S. Clinical review: role of triggering receptor expressed on myeloid cells-1 during sepsis. Crit Care. 2005;9:485–489. doi: 10.1186/cc3732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Ford JW, McVicar DW. TREM and TREM-like receptors in inflammation and disease. Curr Opin Immunol. 2009;21:38–46. doi: 10.1016/j.coi.2009.01.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Gibot S, Kolopp-Sarda MN, Béné MC, Cravoisy A, Levy B, Faure GC, Bollaert PE. Plasma level of a triggering receptor expressed on myeloid cells-1: its diagnostic accuracy in patients with suspected sepsis. Ann Intern Med. 2004;141:9–15. doi: 10.7326/0003-4819-141-1-200407060-00009. [DOI] [PubMed] [Google Scholar]
- 75.Zhang J, She D, Feng D, Jia Y, Xie L. Dynamic changes of serum soluble triggering receptor expressed on myeloid cells-1 (sTREM-1) reflect sepsis severity and can predict prognosis: a prospective study. BMC Infect Dis. 2011;11:53. doi: 10.1186/1471-2334-11-53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Jiyong J, Tiancha H, Wei C, Huahao S. Diagnostic value of the soluble triggering receptor expressed on myeloid cells-1 in bacterial infection: a meta-analysis. Intensive Care Med. 2009;35:587–595. doi: 10.1007/s00134-008-1333-z. [DOI] [PubMed] [Google Scholar]
- 77.Wu Y, Wang F, Fan X, Bao R, Bo L, Li J, Deng X. Accuracy of plasma sTREM-1 for sepsis diagnosis in systemic inflammatory patients: a systematic review and meta-analysis. Crit Care. 2012;16:R229. doi: 10.1186/cc11884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Jeong SJ, Song YG, Kim CO, Kim HW, Ku NS, Han SH, Choi JY, Kim JM. Measurement of plasma sTREM-1 in patients with severe sepsis receiving early goal-directed therapy and evaluation of its usefulness. Shock. 2012;37:574–578. doi: 10.1097/SHK.0b013e318250da40. [DOI] [PubMed] [Google Scholar]
- 79.Ploug M, Rønne E, Behrendt N, Jensen AL, Blasi F, Danø K. Cellular receptor for urokinase plasminogen activator. Carboxyl-terminal processing and membrane anchoring by glycosyl-phosphatidylinositol. J Biol Chem. 1991;266:1926–1933. [PubMed] [Google Scholar]
- 80.Blasi F, Carmeliet P. uPAR: a versatile signalling orchestrator. Nat Rev Mol Cell Biol. 2002;3:932–943. doi: 10.1038/nrm977. [DOI] [PubMed] [Google Scholar]
- 81.Koch A, Voigt S, Kruschinski C, Sanson E, Dückers H, Horn A, Yagmur E, Zimmermann H, Trautwein C, Tacke F. Circulating soluble urokinase plasminogen activator receptor is stably elevated during the first week of treatment in the intensive care unit and predicts mortality in critically ill patients. Crit Care. 2011;15:R63. doi: 10.1186/cc10037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Kofoed K, Andersen O, Kronborg G, Tvede M, Petersen J, Eugen-Olsen J, Larsen K. Use of plasma C-reactive protein, procalcitonin, neutrophils, macrophage migration inhibitory factor, soluble urokinase-type plasminogen activator receptor, and soluble triggering receptor expressed on myeloid cells-1 in combination to diagnose infections: a prospective study. Crit Care. 2007;11:R38. doi: 10.1186/cc5723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Koch A, Tacke F. Why high suPAR is not super--diagnostic, prognostic and potential pathogenic properties of a novel biomarker in the ICU. Crit Care. 2011;15:1020. doi: 10.1186/cc10577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Backes Y, van der Sluijs KF, Mackie DP, Tacke F, Koch A, Tenhunen JJ, Schultz MJ. Usefulness of suPAR as a biological marker in patients with systemic inflammation or infection: a systematic review. Intensive Care Med. 2012;38:1418–1428. doi: 10.1007/s00134-012-2613-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Donadello K, Scolletta S, Covajes C, Vincent JL. suPAR as a prognostic biomarker in sepsis. BMC Med. 2012;10:2. doi: 10.1186/1741-7015-10-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Haupt TH, Petersen J, Ellekilde G, Klausen HH, Thorball CW, Eugen-Olsen J, Andersen O. Plasma suPAR levels are associated with mortality, admission time, and Charlson Comorbidity Index in the acutely admitted medical patient: a prospective observational study. Crit Care. 2012;16:R130. doi: 10.1186/cc11434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Uusitalo-Seppälä R, Huttunen R, Tarkka M, Aittoniemi J, Koskinen P, Leino A, Vahlberg T, Rintala EM. Soluble urokinase-type plasminogen activator receptor in patients with suspected infection in the emergency room: a prospective cohort study. J Intern Med. 2012;272:247–256. doi: 10.1111/j.1365-2796.2012.02569.x. [DOI] [PubMed] [Google Scholar]
- 88.David S, Kümpers P, van Slyke P, Parikh SM. Mending leaky blood vessels: the angiopoietin-Tie2 pathway in sepsis. J Pharmacol Exp Ther. 2013;345:2–6. doi: 10.1124/jpet.112.201061. [DOI] [PubMed] [Google Scholar]
- 89.Fiedler U, Reiss Y, Scharpfenecker M, Grunow V, Koidl S, Thurston G, Gale NW, Witzenrath M, Rosseau S, Suttorp N, Sobke A, Herrmann M, Preissner KT, Vajkoczy P, Augustin HG. Angiopoietin-2 sensitizes endothelial cells to TNF-alpha and has a crucial role in the induction of inflammation. Nat Med. 2006;12:235–239. doi: 10.1038/nm1351. [DOI] [PubMed] [Google Scholar]
- 90.Ricciuto DR, dos Santos CC, Hawkes M, Toltl LJ, Conroy AL, Rajwans N, Lafferty EI, Cook DJ, Fox-Robichaud A, Kahnamoui K, Kain KC, Liaw PC, Liles WC. Angiopoietin-1 and angiopoietin-2 as clinically informative prognostic biomarkers of morbidity and mortality in severe sepsis. Crit Care Med. 2011;39:702–710. doi: 10.1097/CCM.0b013e318206d285. [DOI] [PubMed] [Google Scholar]
- 91.Gibot S, Béné MC, Noel R, Massin F, Guy J, Cravoisy A, Barraud D, De Carvalho Bittencourt M, Quenot JP, Bollaert PE, Faure G, Charles PE. Combination biomarkers to diagnose sepsis in the critically ill patient. Am J Respir Crit Care Med. 2012;186:65–71. doi: 10.1164/rccm.201201-0037OC. [DOI] [PubMed] [Google Scholar]
- 92.Shapiro NI, Trzeciak S, Hollander JE, Birkhahn R, Otero R, Osborn TM, Moretti E, Nguyen HB, Gunnerson KJ, Milzman D, Gaieski DF, Goyal M, Cairns CB, Ngo L, Rivers EP. A prospective, multicenter derivation of a biomarker panel to assess risk of organ dysfunction, shock, and death in emergency department patients with suspected sepsis. Crit Care Med. 2009;37:96–104. doi: 10.1097/CCM.0b013e318192fd9d. [DOI] [PubMed] [Google Scholar]
- 93.Peres Bota D, Mélot C, Lopes Ferreira F, Vincent JL. Infection Probability Score (IPS): A method to help assess the probability of infection in critically ill patients. Crit Care Med. 2003;31:2579–2584. doi: 10.1097/01.CCM.0000094223.92746.56. [DOI] [PubMed] [Google Scholar]
- 94.Kofoed K, Eugen-Olsen J, Petersen J, Larsen K, Andersen O. Predicting mortality in patients with systemic inflammatory response syndrome: an evaluation of two prognostic models, two soluble receptors, and a macrophage migration inhibitory factor. Eur J Clin Microbiol Infect Dis. 2008;27:375–383. doi: 10.1007/s10096-007-0447-5. [DOI] [PubMed] [Google Scholar]
- 95.Harbarth S, Holeckova K, Froidevaux C, Pittet D, Ricou B, Grau GE, Vadas L, Pugin J Geneva Sepsis Network. Diagnostic value of procalcitonin, interleukin-6, and interleukin-8 in critically ill patients admitted with suspected sepsis. Am J Respir Crit Care Med. 2001;164:396–402. doi: 10.1164/ajrccm.164.3.2009052. [DOI] [PubMed] [Google Scholar]