

Abstract
ATM mutation and BIRC3 deletion and/or mutation have independently been shown to have prognostic significance in chronic lymphocytic leukemia. However, the relative clinical importance of these abnormalities in patients with a deletion of 11q encompassing the ATM gene has not been established. We screened a cohort of 166 patients enriched for 11q-deletions for ATM mutations and BIRC3 deletion and mutation and determined the overall and progression-free survival among the 133 of these cases treated within the UK LRF CLL4 trial. SNP6.0 profiling demonstrated that BIRC3 deletion occurred in 83% of 11q-deleted cases and always co-existed with ATM deletion. For the first time we have demonstrated that 40% of BIRC3-deleted cases have concomitant deletion and mutation of ATM. While BIRC3 mutations were rare, they exclusively occurred with BIRC3 deletion and a wild-type residual ATM allele. In 11q-deleted cases, we confirmed that ATM mutation was associated with a reduced overall and progression-free survival comparable to that seen with TP53 abnormalities, whereas BIRC3 deletion and/or mutation had no impact on overall and progression-free survival. In conclusion, in 11q-deleted patients treated with first-line chemotherapy, ATM mutation rather than BIRC3 deletion and/or mutation identifies a subgroup with a poorer outcome.
Introduction
Deletion of chromosome 11q (termed del11q) was first recognized as a recurrent karyotypic abnormality acquired during the course of the disease in patients with progressive chronic lymphocytic leukemia (CLL).1 Subsequent interphase fluorescence in situ hybridization (FISH) analysis identified 11q deletion in approximately 20% of patients with CLL, and associations with bulky lymphadenopathy and a poorer outcome for patients under the age of 55 years were noted.2,3 Subsequent studies have documented associations with unmutated IGHV genes, del13q, genomic complexity, short telomeres, progressive disease and a poor outcome in response to alkylating agent or purine analog treatment, which was improved by their use in combination and ameliorated by the further addition of rituximab.4–10
Genomic profiling studies have refined previous karyotypic and FISH studies showing that 11q deletions are mono-allelic, frequently large and include a minimally deleted region (MDR), which encompasses the ATM gene.11–14 Evidence that ATM is a key target of 11q deletions is derived from findings that: 1) mutation of the ATM gene is found in 30–40% of patients with an 11q deletion;15,16 2) the presence of an ATM mutation results in impaired DNA damage responses;15,17–19 and 3) patients in the UK LRF CLL4 trial with biallelic ATM abnormalities (deletion and mutation) have a poorer outcome following the initial therapy with alkylating agent and/or purine analog therapy compared to those with mono-allelic ATM deletion or mutation.20
However, uncertainty remains as to whether the poorer outcome of patients with 11q deletion in the absence of an ATM mutation is simply a consequence of ATM haploinsufficiency. Alternative possibilities that have been considered include deletion, mutation or epigenetic silencing of other genes either within or outside the MDR or the associated genomic complexity.8,21–23 Neither candidate gene sequencing nor whole exome sequencing studies have identified mutations within other genes located in the MDR.24,25 However, recent data have revealed a high incidence of deletion or, more rarely, mutation of BIRC3, a negative regulator of non-canonical NFκB signaling located at 11q22. It has been reported that BIRC3 deletion and/or mutation (previously termed “BIRC3 disruption”) occurs in a mutually exclusive manner with TP53 abnormalities, is associated with fludarabine-resistance,26 and when detected at diagnosis predicts for poor overall survival independent of 11q deletion.27
The above data strongly suggest that there are subsets of del11q patients that exhibit differing responses to standard treatment. However, the relative frequency and clinical significance of ATM and BIRC3 abnormalities is unclear. This study addresses this issue in a large cohort of 11q-deleted patients detected by SNP6 profiling and screened for ATM and BIRC3 mutations. As a consequence, in the context of a phase III clinical trial of chemotherapy, we show that ATM mutational status remains the most clinically informative genomic lesion in 11q-deleted CLL, identifying cases with outcome comparable to TP53 deletion and/or mutation patients, and that the presence of BIRC3 deletion and/or mutation is associated with outcome comparable to other 11q-deleted CLL cases.
Methods
Patients and molecular diagnostic assays
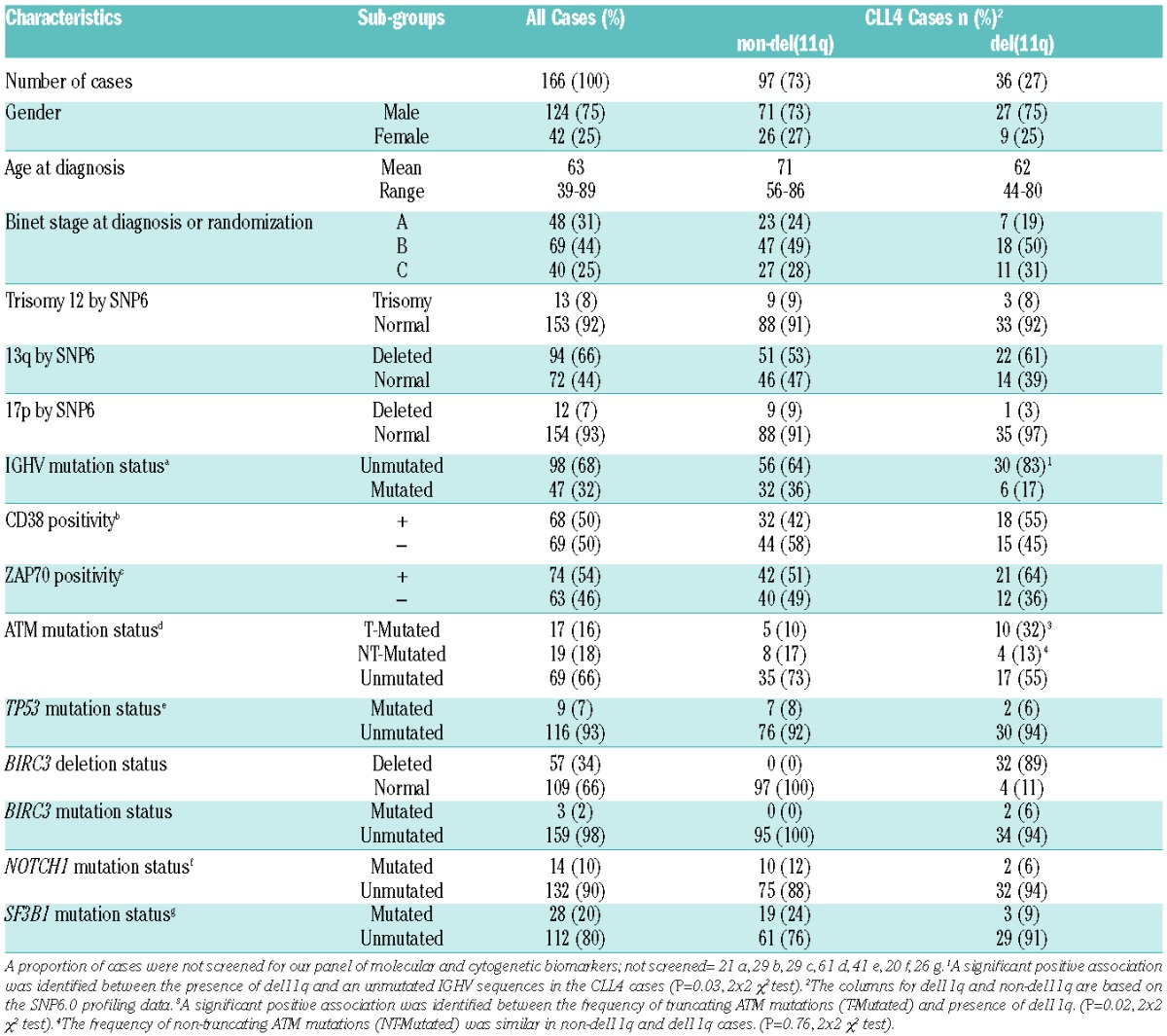
A total of 166 untreated CLL patients diagnosed according to standard morphological and immunophenotypic criteria were included in this study (Table 1 and Online Supplementary Table S1). This cohort principally included patients from the UK LRF CLL4 trial9 (n=133) which allowed accurate clinical correlations to be made. An additional 33 11q-deleted patients were also included to allow more significant associations between the 11q deletion and other genomic variables to be made, such as with mutational status of ATM and BIRC3. The additional del11q patients were sampled subsequent to the development of progressive disease, with a median time from diagnosis of 3.2±5.2 years (±1 standard deviation (SD); range 1 month-27 years). For the entire cohort of 166 patients, mutational data were available for TP53 (n=125), SF3B1 (n=140) and NOTCH1 (n=146).28,29 Details on the molecular diagnostic assays30,31 are available in the Online Supplementary Methods. Informed consent was obtained from all patients in accordance with the Declaration of Helsinki and our local ethics committee gave their approval for the study.
Table 1.
Cohort characteristics.
DNA extraction, SNP6 array hybridization, data extraction and analysis
Genomic DNA was extracted from CLL B cells (n=166) and buccal swabs (n=32), prior to being purified, amplified, labeled and hybridized to the Affymetrix SNP6.0 platform (Affymetrix, Santa Clara, CA, USA) as previously described32 (Online Supplementary Methods).
Mutational analysis of ATM and BIRC3 genes
The presence or absence of somatically-acquired single nucleotide variants (SNVs or mutations) in ATM and BIRC3 were successfully ascertained in 105 (CLL4 cases: n=79 of 133) and 162 (CLL4 cases: n=131 of 133) patients, respectively. Denaturing high-performance liquid chromatography (DHPLC), high-resolution melt (HRM) polymerase chain reaction (PCR) analysis and Sanger sequencing were utilized.20,26,27,29 More details of methods and the strategy adopted for assigning the somatic nature of each SNV are provided in the Online Supplementary Methods and Online Supplementary Table S2.
Statistical analysis
Statistical analysis was performed using SPSS (v.20). Associations with treatment response and clinical outcome were only performed on the LRF UK CLL4 cases due to the homogeneous and well-annotated nature of this cohort (Online Supplementary Methods). The LRF UK CLL4 cohort included in this current study did not differ significantly from the entire cohort for an extensive panel of variables, with the enrichment exception of del11q (P=0.002) and del13q (P<0.001) (Online Supplementary Table S1). Kaplan-Meier analysis with the log rank test or Cox regression was used for survival analyses on overall survival (OS) and progression-free survival (PFS). χ2 test (Pearson or Fisher Exact test when necessary) were also employed for some comparisons and are described where relevant in the main text or table footnotes. P=0.05 was considered statistically significant. Previous reports have demonstrated that BIRC3 disruption occurs in 50% of 11q deleted cases and is associated with survival comparable to TP53 deleted CLL.26,27 Therefore, with clinical follow up of ten years, our UK LRF CLL4 cohort (del11q, n=36) had 97% power with a significance level of 0.05 to detect a difference in OS between cases with and without BIRC3 deletion and/or mutation based on the median CLL4 OS duration for cases with del11q (53 months) and del17p (14 months) detected by FISH.
Results
Incidence of ATM and BIRC3 deletions
We analyzed all 166 patients for 11q deletions and copy number neutral-loss of heterozygosity (CNNLOH) events using the SNP 6.0 genome-wide copy number arrays. Sixty-nine patients had 11q deletions that all included a minimally deleted region (MDR) which was 416 Kb in size (chr11:107.498-107.914Mb) and contained the following genes: ACAT1, NPAT, ATM, C11orf65, KDELC2, LOC1000127964, LOC1000128794 and EXPH5 (Figure 1A). We observed that the majority of 11q-deleted cases (67 of 69) had deletions much larger than the MDR and 57 of 69 (83%) lost one copy of the BIRC3 gene. In 56 of these patients, ATM and BIRC3 genes were lost as part of a single deletion event while in one patient the genes were lost as a consequence of two separate deletions events. In 4 patients (6%), the centromeric deletion breakpoint was within the BIRC3 gene body, resulting in loss of the 3′ end of the gene that contains the C terminal RING domain important for the proteasomal degradation of MAP3K14 (Figure 1A).
Figure 1.

Chromosome 11 architecture, 11q23 minimally deleted region and BIRC3 deletion and/or mutation in 11q-deleted CLL [In color] (A) Left to right: Genomic location in Mb from the telomere of 11p (top), through the centromere to the telomere of 11q (bottom); an example 11q deleted SNP6.0 probe profile showing an interstitial deletion between genomic locations 74 and 103Mb which includes the ATM and BIRC3 loci; representative CNNLOH (green lines) observed in our cohort where the size and position of the line shows the genomic location and size of the CNNLOH event; heatmap of 69 11q deleted cases, where white, red and blue show regions of no copy number change, duplications and deletions, respectively. Focussed heatmap views of ATM and BIRC3 genes demonstrating the ATM MDR and the 4 cases with a telomeric deletion breakpoint in the 3′ BIRC3 gene locus are also shown (the second case from the left has deletion of both BIRC3 and ATM, which is the result of two deletion events in this patient). (B) Abnormality matrix of cases with ATM and BIRC3 lesions. Each row is a genetic lesion present in our cohort, and each column is a patient where red, grey and white, shows the presence, absence or no data for the lesion in question, respectively. (C) Sanger sequencing traces of the three BIRC3 gene mutations identified in our study. (D) Venn-diagram of the relationship between BIRC3 deletion and/or mutation and ATM deletion and mutation (n: number of observations).
Incidence of ATM and BIRC3 mutations
BIRC3 mutation screening was successfully ascertained in 162 of 166 patients. A BIRC3 gene mutation was detected in only 3 patients all of whom had a large mono-allelelic 11q-deletion encompassing both the ATM gene and the BIRC3 gene located at 11q22. The BIRC3 gene mutations are predicted to be deleterious for BIRC3 protein function, the p.R434Kfs*10 (frameshift in/del) and p.L585* (STOP-codon) mutations both target highly conserved amino acid residues, resulting in truncation of BIRC3 protein with loss of the C terminal CARD-RING and RING domains, respectively. The p.I570del (3bp in-frame deletion) mutation targets another highly conserved amino acid, resulting in loss of the C-beta branched amino acid residue, isoleucine at the C terminal end of the beta-sheet structure in the RING domain (Figure 1C). ATM gene mutation screening was successfully completed in 105 patients and identified mutations in 36 patients. The mutations were classified as somatic and pathogenic based on our previously reported criteria (Online Supplementary Methods) and occurred in exons 2-63, between amino acids 37-3047, affecting the TAN, FAT, PI3K and FATc domains of the ATM protein (Online Supplementary Table S3). ATM mutations occurred in the absence of an 11q-deletion in 27% (13 of 48) of patients screened and in 40% (23 of 57) of 11q-deleted patients. Interestingly, we identified that a single case with an ATM mutation (c.8428-8450del23:p.Lys2810fs) also harbored CNNLOH of the region duplicating the variant. This case highlights that in rare instances biallelic inactivation of ATM may occur independently of chromosome deletion yet current molecular diagnostic tests do not detect these events (N.B. this case was not included in our survival analyses). Importantly, we observed that within 11q-deleted patients, with loss of both ATM and BIRC3 genes, and successfully screened for gene mutation, 40% (19 of 48) with a BIRC3 deletion also had an ATM mutation (Figure 1D).
Relative importance of ATM and BIRC3 abnormalities on outcome of patients with 11q deletions
Within the CLL4 cohort (n=133), there were 36 patients with an 11q deletion of whom 32 had loss of both ATM and BIRC3 genes, 2 had a BIRC3 mutation, and 14 had an ATM mutation. Initially, we confirmed in univariate analysis that within this cohort, unmutated IGHV genes and deletions of 11q and TP53 were associated with short PFS and OS, as found in larger studies of prognostic markers in this trial (Table 2 model A).9,20,28,29,33 Specifically, 11q deleted patients exhibited a median OS and PFS of 53 months (95%CI:36–69; P=0.004) and 20 months (95%CI: 6–33; P<0.001), respectively.9,20,28,29,33 Inclusion of BIRC3 deletion and mutation into the model (Table 2 model B) showed that BIRC3 deleted/mutated cases had a reduced survival compared to non-11q deleted cases, with a median OS of 53 months (95%CI: 39–67) and PFS of 17 (95%CI: 4–30). As expected, there was no detectable difference (OS: P=0.52 and PFS: P=0.42) in outcome between all cases with del11q and those with BIRC3 deletion/mutation, consistent with the high incidence of BIRC3 loss in del 11q cases (Table 2 model B and Figure 2A and B).
Table 2.
Survival models of TP53, ATM and BIRC3 disruption in CLL4 cases.
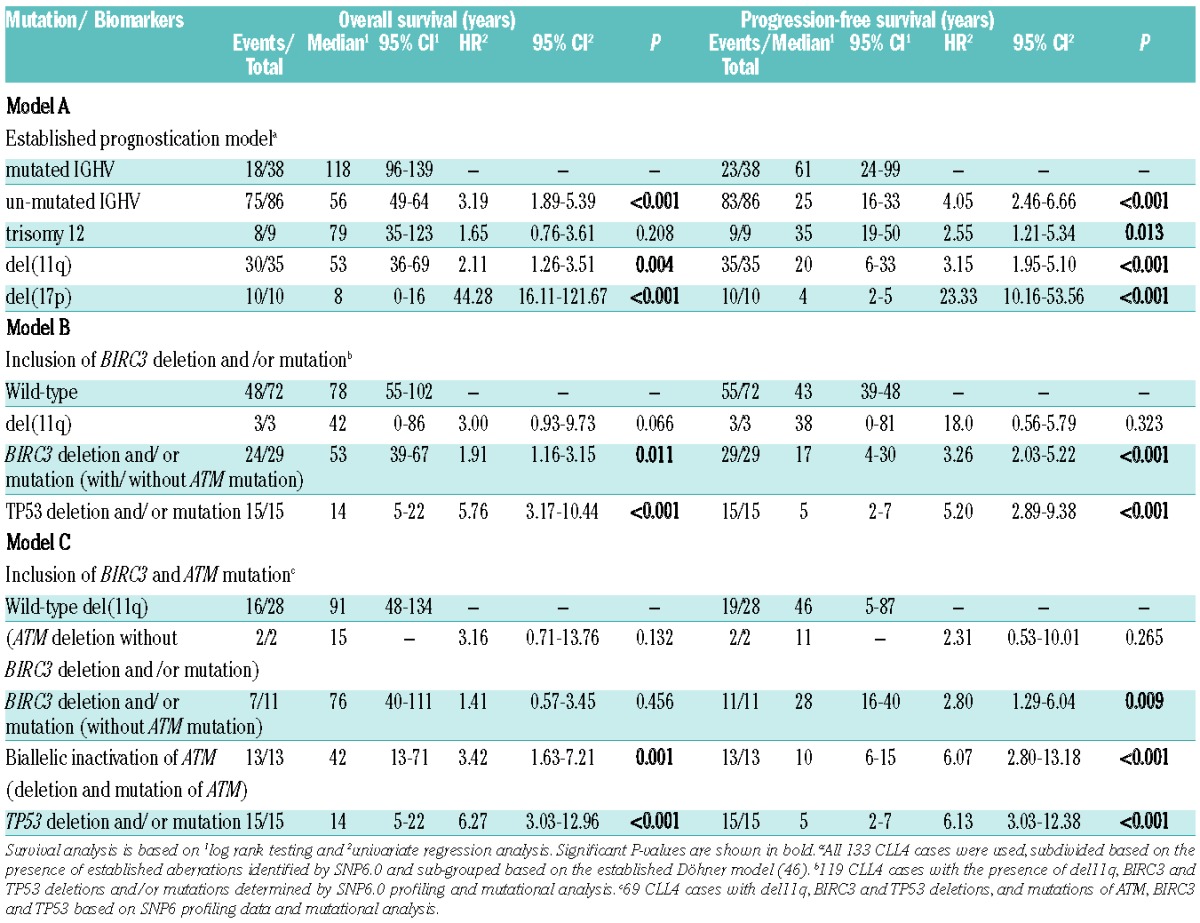
Figure 2.
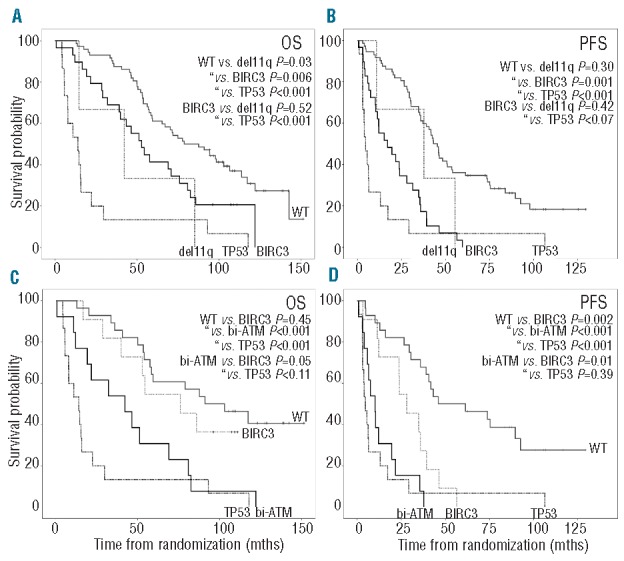
Overall and progression-free survival in CLL4 cases (A) and (B) show CLL4 overall and progression-free survival, respectively; for cases sub-grouped by TP53 deletion/SNV (dashed black line), BIRC3 deletion and/or mutation (black line), 11q deletion without BIRC3 (dashed gray line) or wild-type (gray line) for TP53, BIRC3 genes (no deletion or mutation) and 11q-deletions. (C) and (D) show CLL4 overall and progression-free survival, respectively; for the cases sub-divided into TP53 deletion/mutated (dashed black line), biallelic inactivation of ATM (black line), BIRC3 deletion and/or mutation (dashed gray line) and wild-type (gray line) for TP53, BIRC3, ATM genes (no deletion or mutation) and 11q deletion. The survival curve for del11q (without an ATM mutation or BIRC3 deletion and/or mutation) was precluded due to only two survival events.
Finally, we demonstrated that the most significant reduction in OS and PFS in 11q-deleted patients was observed in patients with mutations targeting the ATM gene. These patients exhibited a median OS and PFS of 42 (95%CI: 13–71) and 10 months (95%CI: 6–15), respectively. Importantly, cases with a BIRC3 deletion/mutation that did not have an ATM mutation had significantly longer survival times for OS (76 vs. 42 months; P=0.05) and PFS (28 vs. 10 months; P=0.01) than cases with biallelic inactivation of ATM (Table 2 model C).
Discussion
This study extends recent observations on the incidence and clinical significance of ATM and BIRC3 loss and/or mutation (SNV) in CLL patients with an 11q deletion. We had previously shown that the combination of an 11q deletion encompassing the ATM gene and mutation of the remaining ATM allele was associated with shorter progression-free and overall survival than a del11q with wild-type ATM in patients receiving first-line chemotherapy in the UK LRF CLL4 trial.20 This observation is consistent with the importance of functional ATM protein in the response to DNA damage.17,34–36 While several smaller studies have not identified an impact of ATM mutational status on patient survival, they did not differentiate ATM mutated individuals into those with and without deletion of 11q23.37,38 Rossi and colleagues independently reported that BIRC3 disruption resulting from complete or partial BIRC3 loss with or without mutation of the remaining allele is common in patients who are refractory to, but not in those sensitive to, fludarabine-containing regimens.26 Specifically, they noted that: 1) recurrent mutations target BIRC3 in CLL, albeit at low frequencies; 2) BIRC3 is recurrently deleted principally due to large genomic deletions on 11q; 3) in a single CLL case the BIRC3 gene was deleted without concomitant loss of ATM; and 4) the gene-body of BIRC3 is targeted by rare proximal 11q-deletion breakpoints. These data are consistent with the tumor suppressor role of BIRC3 as a negative regulator of the non-canonical NF-KB pathway and the known importance of NK-KB pathway activation in CLL by multiple mechanisms.
By studying a relatively large cohort of patients with del 11q screened for both ATM and BIRC3 abnormalities, we confirm the high incidence of BIRC3 deletion in cases with del 11q and the lack of BIRC3 deletion in the absence of ATM deletion. In support of previously published work,26 our data also show that BIRC3 mutations are rare in a cohort of untreated CLL patients with progressive disease, suggesting limited clonal selection of these mutations prior to treatment. Our most important observation is the high frequency of missense or nonsense ATM mutations in BIRC3 deleted cases (40%).
Investigating the clinical significance of these findings in patients entered into the UK LRF CLL4 trial confirmed that patients with bi-allelic ATM abnormalities had a shorter PFS and OS than cases with del 11q and wild-type ATM. Although 11q-deleted cases with BIRC3 deletion and/or mutation did exhibit reduced OS and PFS compared to non-11q deleted cases, this was not significantly different from 11q-deleted cases without BIRC3 deletion and/or mutation and much superior to cases with bi-allelic ATM abnormalities and TP53 deletion/mutation. Furthermore, when we stratified the CLL4 cases that have large 11q23 deletions encompassing both BIRC3 and ATM genes (n=24) by presence or absence of ATM mutation, we were able to identify that patients with an ATM mutation had a shorter PFS (HR=3.03, 95%CI: 1.22–7.49; P=0.017), but not OS, when compared to the patients with only BIRC3 deletion/mutation (data not shown). Our negative finding for CLL4 overall survival in this sub-group analysis must be interpreted with caution due to the lack of power (29%) (Online Supplementary Methods).
Several limitations to this study are noted. 1) In view of the frequency with which ATM and BIRC3 deletions coexist, a much larger study would be required to identify differences in outcome between patients with ATM deletion compared to those with ATM and BIRC3 deletion. 2) Given that the UK LRF CLL4 trial compared different chemotherapy regimens in previously untreated patients, it will be important to validate these observations in the context of chemo-immunotherapy trials, in studies of novel agents, such as B-cell receptor (BCR) signaling inhibitors, and in patients with relapsed or refractory disease. 3) Our study has focused on ATM and BIRC3 abnormalities. However, deletion of 11q frequently results in the loss of many other genes involved in key regulatory pathways that could impact on CLL pathogenesis.8 As an example, MRE11A and H2AFX, both of which are involved in DNA damage response, are also deleted in 58% (n=40) and 26% (n=18), respectively. Indeed, 53% (17 of 31) of our BIRC3-deleted cases also lost H2AFX and/or MRE11A. Furthermore, although we identified recurrent deletion breakpoints within the gene body of BIRC3, we also identified recurrent breakpoints in the bodies of other 11q genes (Online Supplementary Table S4), including CEP164, which encodes a mediator protein required for the maintenance of genomic instability.39 Similarly we have not investigated the potential clinical consequences of the elevated genomic complexity associated with del 11q nor the incidence of epigenetic silencing of genes on the retained 11q allele. As some previous studies have noted an association between del 11q and SF3B1 gene mutations we considered whether the incidence of SF3B1 mutations, and the presence of CLL-specific ATM splice forms in SF3B1 mutated cases.40 might differ between cases with or without an ATM mutation but observed no significant enrichment of SF3B1 mutations in either the 11q-deleted, ATM mutated or patients with biallelic ATM abnormalities suggesting that this mutation does not contribute to the poor prognosis associated with 11q abnormalities (data not shown).
In conclusion, we confirm that in patients treated with chemotherapy as part of the UK LRF CLL4 trial, the presence of an ATM mutation subdivided 11q-deleted CLL into a sub-group with significantly shorter overall and progression-free survival. BIRC3 deletion/mutation did not identify an 11q-deleted patient subgroup with dismal outcome comparable to TP53 deletion/mutation. In fact, within 11q-deleted patients, BIRC3 deletion/mutation was associated with significantly longer survival times than ATM mutation. We would caution against interpreting the clinical impact of BIRC3 abnormalities without knowledge of ATM mutational status.
Acknowledgments
The authors gratefully acknowledge all patients and clinicians who participated in the trial. The authors would also like to thank Professor Nick Cross for help with the preparation of this manuscript.
Footnotes
The online version of this article has a Supplementary Appendix.
Funding
The authors would like to thank Leukaemia and Lymphoma Research, the Kay Kendall Leukaemia Fund and Wessex Medical Research for funding this study. The UK LRF CLL4 trial was funded by a core grant from Leukaemia and Lymphoma Research, with associated research work supported by the MRC (G8223452) and Cancer Research UK, and laboratory studies by the Arbib Foundation, Schering Healthcare UK, Schering AG, Germany and Leukaemia and Lymphoma Research.
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Fegan C, Robinson H, Thompson P, Whittaker JA, White D. Karyotypic evolution in CLL: identification of a new subgroup of patients with deletions of 11q and advanced or progressive disease. Leukemia. 1995;9(12):2003–8 [PubMed] [Google Scholar]
- 2.Döhner H, Stilgenbauer S, James MR, Benner A, Weilguni T, Bentz M, et al. 11q deletions identify a new subset of B-cell chronic lymphocytic leukemia characterized by extensive nodal involvement and inferior prognosis. Blood. 1997;89(7):2516–22 [PubMed] [Google Scholar]
- 3.Neilson JR, Auer R, White D, Bienz N, Waters JJ, Whittaker JA, et al. Deletions at 11q identify a subset of patients with typical CLL who show consistent Cytogenetic analysis. Leukemia. 1997;11(11):1929–32 [DOI] [PubMed] [Google Scholar]
- 4.Trbusek M, Malcikova J, Smardova J, Kuhrova V, Mentzlova D, Francova H, et al. Inactivation of p53 and deletion of ATM in B-CLL patients in relation to IgVH mutation status and previous treatment. Leukemia. 2006;20(6):1159–61 [DOI] [PubMed] [Google Scholar]
- 5.Hallek M, Fischer K, Fingerle-Rowson G, Fink AM, Busch R, Mayer J, et al. Addition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocytic leukaemia: a randomised, open-label, phase 3 trial. Lancet. 2010;376(9747):1164–74 [DOI] [PubMed] [Google Scholar]
- 6.Saiya-Cork K, Collins R, Parkin B, Ouillette P, Kuizon E, Kujawski L, et al. A pathobiological role of the insulin receptor in chronic lymphocytic leukemia. Clin Cancer Res. 2011;17(9):2679–92 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Britt-Compton B, Lin TT, Ahmed G, Weston V, Jones RE, Fegan C, et al. Extreme telomere erosion in ATM-mutated and 11q-deleted CLL patients is independent of disease stage. Leukemia. 2012;26(4):826–30 [DOI] [PubMed] [Google Scholar]
- 8.Ouillette P, Fossum S, Parkin B, Ding L, Bockenstedt P, Al-Zoubi A, et al. Aggressive chronic lymphocytic leukemia with elevated genomic complexity is associated with multiple gene defects in the response to DNA double-strand breaks. Clin Cancer Res. 2010;16(3):835–47 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Catovsky D, Richards S, Matutes E, Oscier D, Dyer MJS, Bezares RF, et al. Assessment of fludarabine plus cyclophosphamide for patients with chronic lymphocytic leukaemia (the LRF CLL4 Trial): a randomised controlled trial. Lancet. 2007;370(9583):230–9 [DOI] [PubMed] [Google Scholar]
- 10.Tsimberidou A-M, Tam C, Abruzzo LV, O’Brien S, Wierda WG, Lerner S, et al. Chemoimmunotherapy may overcome the adverse prognostic significance of 11q deletion in previously untreated patients with chronic lymphocytic leukemia. Cancer. 2009;115(2):373–80 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Schwaenen C, Nessling M, Wessendorf S, Salvi T, Wrobel G, Radlwimmer B, et al. Automated array-based genomic profiling in chronic lymphocytic leukemia: development of a clinical tool and discovery of recurrent genomic alterations. Proc Natl Acad Sci USA. 2004;101(4):1039–44 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Pfeifer D, Pantic M, Skatulla I, Rawluk J, Kreutz C, Martens UM, et al. Genome-wide analysis of DNA copy number changes and LOH in CLL using high-density SNP arrays. Blood. 2007;109(3):1202–10 [DOI] [PubMed] [Google Scholar]
- 13.Lehmann S, Ogawa S, Raynaud SD, Sanada M, Nannya Y, Ticchioni M, et al. Molecular allelokaryotyping of early-stage, untreated chronic lymphocytic leukemia. Cancer. 2008;112(6):1296–305 [DOI] [PubMed] [Google Scholar]
- 14.Edelmann J, Holzmann K, Miller F, Winkler D, Bühler A, Zenz T, et al. High-resolution genomic profiling of chronic lymphocytic leukemia reveals new recurrent genomic alterations. Blood. 2012;120(24):4783–94 [DOI] [PubMed] [Google Scholar]
- 15.Austen B, Powell JE, Alvi A, Edwards I, Hooper L, Starczynski J, et al. Mutations in the ATM gene lead to impaired overall and treatment-free survival that is independent of IGVH mutation status in patients with B-CLL. Blood. 2005;106(9):3175–82 [DOI] [PubMed] [Google Scholar]
- 16.Wang L, Lawrence MS, Wan Y, Stojanov P, Sougnez C, Stevenson K, et al. SF3B1 and other novel cancer genes in chronic lymphocytic leukemia. N Engl J Med. 2011;365(26):2497–506 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Austen B, Skowronska A, Baker C, Powell JE, Gardiner A, Oscier D, et al. Mutation status of the residual ATM allele is an important determinant of the cellular response to chemotherapy and survival in patients with chronic lymphocytic leukemia containing an 11q deletion. J Clin Oncol. 2007;25(34):5448–57 [DOI] [PubMed] [Google Scholar]
- 18.Pettitt AR, Sherrington PD, Stewart G, Cawley JC, Taylor AM, Stankovic T. p53 dysfunction in B-cell chronic lymphocytic leukemia: inactivation of ATM as an alternative to TP53 mutation. Blood. 2001;98(3):814–22 [DOI] [PubMed] [Google Scholar]
- 19.Best OG, Gardiner AC, Majid A, Walewska R, Austen B, Skowronska A, et al. A novel functional assay using etoposide plus nutlin-3a detects and distinguishes between ATM and TP53 mutations in CLL. Leukemia. 2008;22(7):1456–9 [DOI] [PubMed] [Google Scholar]
- 20.Skowronska A, Parker A, Ahmed G, Oldreive C, Davis Z, Richards S, et al. Biallelic ATM inactivation significantly reduces survival in patients treated on the United Kingdom Leukemia Research Fund Chronic Lymphocytic Leukemia 4 trial. J Clin Oncol. 2012;30(36):4524–32 [DOI] [PubMed] [Google Scholar]
- 21.Auer RL, Starczynski J, McElwaine S, Bertoni F, Newland AC, Fegan CD, et al. Identification of a potential role for POU2AF1 and BTG4 in the deletion of 11q23 in chronic lymphocytic leukemia. Genes Chromosomes Cancer. 2005;43(1):1–10 [DOI] [PubMed] [Google Scholar]
- 22.Visone R, Rassenti LZ, Veronese A, Taccioli C, Costinean S, Aguda BD, et al. Karyotype-specific microRNA signature in chronic lymphocytic leukemia. Blood. 2009;114(18):3872–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Marasca R, Maffei R, Martinelli S, Fiorcari S, Bulgarelli J, Debbia G, et al. Clinical heterogeneity of de novo 11q deletion chronic lymphocytic leukaemia : prognostic relevance of extent of 11q deleted nuclei inside leukemic clone. Hematol Oncol. 2013;31(2):348–55 [DOI] [PubMed] [Google Scholar]
- 24.Kalla C, Scheuermann MO, Kube I, Schlotter M, Mertens D, Döhner H, et al. Analysis of 11q22-q23 deletion target genes in B-cell chronic lymphocytic leukaemia: evidence for a pathogenic role of NPAT, CUL5, and PPP2R1B. Eur J Cancer. 2007;43(8):1328–35 [DOI] [PubMed] [Google Scholar]
- 25.Landau Da, Carter SL, Stojanov P, McKenna A, Stevenson K, Lawrence MS, et al. Evolution and impact of subclonal mutations in chronic lymphocytic leukemia. Cell. 2013;152(4):714–26 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rossi D, Fangazio M, Rasi S, Vaisitti T, Monti S, Cresta S, et al. Disruption of BIRC3 associates with fludarabine chemorefractoriness in TP53 wild-type chronic lymphocytic leukemia. Blood. 2012;119(12):2854–62 [DOI] [PubMed] [Google Scholar]
- 27.Rossi D, Rasi S, Spina V, Bruscaggin A, Monti S, Ciardullo C, et al. Integrated mutational and cytogenetic analysis identifies new prognostic subgroups in chronic lymphocytic leukemia. Blood. 2013;121(8):1403–12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Gonzalez D, Martinez P, Wade R, Hockley S, Oscier D, Matutes E, et al. Mutational status of the TP53 gene as a predictor of response and survival in patients with chronic lymphocytic leukemia: results from the LRF CLL4 trial. J Clin Oncol. 2011;29(16):2223–9 [DOI] [PubMed] [Google Scholar]
- 29.Oscier DG, Rose-Zerilli MJJ, Winkelmann N, Gonzalez de Castro D, Gomez B, Forster J, et al. The clinical significance of NOTCH1 and SF3B1 mutations in the UK LRF CLL4 trial. Blood. 2013;121(3):468–75 [DOI] [PubMed] [Google Scholar]
- 30.Best OG, Ibbotson RE, Parker AE, Davis ZA, Orchard JA, Oscier DG. ZAP-70 by flow cytometry: a comparison of different antibodies, anticoagulants, and methods of analysis. Cytometry B Clin Cytom 2006;70(4):235–241 [DOI] [PubMed] [Google Scholar]
- 31.Hamblin TJ, Davis Z, Gardiner a, Oscier DG, Stevenson FK. Unmutated Ig V(H) genes are associated with a more aggressive form of chronic lymphocytic leukemia. Blood. 1999;94(6):1848–54 [PubMed] [Google Scholar]
- 32.Parker H, Rose-Zerilli MJJ, Parker A, Chaplin T, Wade R, Gardiner A, et al. 13Q Deletion Anatomy and Disease Progression in Patients With Chronic Lymphocytic Leukemia. Leukemia. 2011;25(3):489–97 [DOI] [PubMed] [Google Scholar]
- 33.Oscier DG, Gardiner AC, Mould SJ, Glide S, Davis ZA, Ibbotson RE, et al. Multivariate analysis of prognostic factors in CLL: clinical stage, IGVH gene mutational status, and loss or mutation of the p53 gene are independent prognostic factors. Blood. 2002;100(4):1177–84 [PubMed] [Google Scholar]
- 34.Starostik P, Manshouri T, Brien SO, Leukemia BCL, Lerner S, Keating M. Deficiency of the ATM protein expression defines an aggressive subgroup of B-cell chronic lymphocytic leukemia. Cancer Res 1998;58(20):4552–7 [PubMed] [Google Scholar]
- 35.Grossmann V, Kohlmann A, Schnittger S, Weissmann S, Jeromin S, Kienast J, et al. Recurrent ATM and BIRC3 mutations in patients with chronic lymphocytic leukemia (CLL) and deletion 11q22-q23. Blood. 2012;115 n. 35 ASH Annual Meeting Abstracts. (Abstract):1771 [Google Scholar]
- 36.Stankovic T. Ataxia telangiectasia mutated-deficient B-cell chronic lymphocytic leukemia occurs in pregerminal center cells and results in defective damage response and unrepaired chromosome damage. Blood. 2002;99(1):300–9 [DOI] [PubMed] [Google Scholar]
- 37.Ouillette P, Li J, Shaknovich R, Li Y, Melnick A, Shedden K, et al. Incidence and Clinical Implications of ATM Aberrations in Chronic Lymphocytic Leukemia. Genes Chromosomes Cancer. 2012;51(12):1125–32 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Lozanski G, Ruppert AS, Heerema N a, Lozanski A, Lucas DM, Gordon A, et al. Variations of the ataxia telangiectasia mutated gene in patients with chronic lymphocytic leukemia lack substantial impact on progression-free survival and overall survival: a Cancer and Leukemia Group B study. Leuk Lymphoma. 2012;53(9):1743–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Sivasubramaniam S, Sun X, Pan Y-R, Wang S, Lee EY-HP. Cep164 is a mediator protein required for the maintenance of genomic stability through modulation of MDC1, RPA, and CHK1. Genes Dev. 2008;22(5):587–600 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ferreira PG, Jares P, Rico D, Gómez-López G, Martínez-Trillos A, Villamor N, et al. Transcriptome characterization by RNA sequencing identifies a major molecular and clinical subdivision in chronic lymphocytic leukemia. Genome Res. 2014;24(2):212–26 [DOI] [PMC free article] [PubMed] [Google Scholar]