

Abstract
Objective
This study was designed to define the Korean norm values for the Ricketts analysis.
Methods
In this longitudinal study, lateral cephalograms of 31 subjects with normal occlusion were taken biennially from ages 9-19 years. Cephalometric measurements were performed. Parameters for which the 10-year change did not exceed one standard deviation were defined as unchanged. The means and standard deviations for the measured parameters were determined for each age group.
Results
No significant changes in growth were observed in the molar relationship, incisor overjet, incisor overbite, mandibular incisor extrusion, interincisor angle, lower incisor tip (B1) to A point-Pogonion (A-PO) plane, upper incisor tip (A1) to A-PO plane, B1 inclination to A-PO, A1 inclination to A-PO, B1 inclination to Frankfurt plane (FH), convexity, lower facial height, facial axis, maxillary depth, maxillary height, palatal plane to FH, cranial deflection, ramus Xi position, or porion location. Continual changes over the 10 years of growth were observed in the maxillary first molar distal position to pterygoid true vertical plane, facial depth, mandibular plane to FH, anterior cranial length, mandibular arc, and corpus length.
Conclusions
Clinicians can apply the Korean norms at age 9 as determined in this study when using the Ricketts analysis. The patient's age at the beginning of treatment and their sex should be taken into consideration when drawing visual treatment objectives.
Keywords: Growth and development, Cephalometrics, Korean norms, Ricketts analysis
INTRODUCTION
The purpose of orthodontic treatment is to accomplish aesthetic restoration through the acquisition of a functional occlusion and balanced facial features. Accurate diagnosis is necessary to determine the prognosis and to choose the proper treatment. Treatment planning requires precise prediction of the amount and direction of craniofacial growth. Optimal craniofacial references by age should thus be made available for clinical application.
Early studies of craniofacial growth used conventional craniometry, the measurement of dry skulls as conducted by anthropologists. However, this methodology was limited in subject selection. The development of biometry allowed the direct measurement of the living body, but also had limits, as the soft tissues caused measurement errors that prevented accurate measurement of the changes occurring during craniofacial growth. Since Broadbent1 introduced lateral cephalometric radiography in 1931, studies on craniofacial growth and development have increased, and many researchers have suggested definitions and norms for the normal skeleton and occlusion.
In 1948, Downs2 suggested an analytical method for assessing the craniofacial bones and dentition of the normal occlusion. Later research then led to the development and clinical application of cephalometric analyses using lateral cephalometric radiography.3,4,5,6,7 However, most of this research targeted Caucasian patients. Downs,8 Sassouni,9 and Ricketts10 reported significant differences in cephalometric parameters between races and ethnic groups. In Korea, Hamm and Sohn11 studied the lateral cephalometric radiographs of 159 male and 206 female subjects with normal occlusions, aged 10-19 years. The authors reported the standards for 7 angular measurements and 9 linear measurements based on gender and age and calculated the regression equations by age for each measurement. However, the cross-sectional design of this study prevented the acquisition of accurate or predictive information on growth patterns. Variability in growth and development due to genetics, environment, and lifestyle requires the use of longitudinal studies when determining predictive factors. Park12 reported the growth changes in Korean children aged 6-9 years in a longitudinal study using the Ricketts analysis, but data on adolescent growth was not included. Kim et al.13 measured 10 parameters for the Ricketts analysis using biennial cephalometric radiographs from subjects aged 9-17 years. These authors reported the annual amount of growth and observed that some values did not change while others showed gradual changes in accordance with age. They also drew the visual norm using the mean values for each sex. Studies on the additional parameters needed for comprehensive Ricketts analysis have not yet been performed.
The purpose of this study was to obtain Korean norms for the Ricketts analysis among 9-year-old children. Using biennial lateral cephalometric radiographs, this study also aimed to determine the longitudinal growth changes in 9-19-year-old subjects with normal occlusions to be applied as a reference in clinical orthodontics.
MATERIALS AND METHODS
Subjects
In May 1983, an orthodontist selected the subjects of this study among third graders attending an elementary school in Daegu, South Korea. The selection criteria included good facial balance, normal dentitional development, and a normal molar relationship. Authorization and consent were obtained from the parents of the children for every aspect of participation in this study, which included a total of 6 lateral cephalometric radiographs taken biennially over a period of 10 years.
We started with 68 subjects (36 male, 32 female); due to inconsistent participation, 31 subjects (18 male, 13 female) remained at the end of the study. The mean age of the final group of subjects was 9 years at the beginning and 19 years at the end.
Tracing of cephalograms and data entry
Cephalograms were taken with the subject's Frankfurt (FH) plane parallel to the horizontal plane while in centric occlusion. The target-subject distance was 152.4 cm, and the subject-film distance was 14 cm. All radiographs were traced by the same researcher to minimize differences in the tracing process. All serial radiographs for each participant were superimposed. A different researcher entered and digitized the traced acetate sheets using a computer program (Orthococktail; Kyungpook National University, Daegu, Korea). We set up craniometric points for the Ricketts analysis and computed the angles to the nearest 0.1° and distances to the nearest 0.1 mm for each measurement (Figure 1).
Figure 1.

Anatomic and cephalometric landmarks. NA, Nasion; OR, orbitale; PR, porion; BA, basion; PT, pterygoid point; DC, condyle center point; CC, center of cranium point; CF, center of face point; ANS, anterior nasal spine; PNS, posterior nasal spine; AP, A point; XI, Xi point; PM, protuberance menti; P, pogonion; GN, gnathion; GO, gonion; A1, upper incisor tip; AR, upper incisor root tip; A6, upper first molar distal; B1, lower incisor tip; BR, lower incisor root tip; B6, lower first molar distal. FH, Frankfurt.
Measurements
The parameters measured for each reference were as follows. Dental relationship: molar relationship, incisor overjet, incisor overbite, mandibular incisor extrusion, and interincisor angle (Figure 2); Dental to skeletal relationship: A6 molar position to PTV, B1 to A-PO plane, A1 to A-PO plane, B1 inclination to A-PO, A1 inclination to A-PO, and B1 inclination to FH (Figure 3); Skeletal relationship: convexity and lower facial height (Figure 4); Jaw to cranium: facial depth, facial axis, maxillary depth, maxillary height, palatal plane to FH, and mandibular plane to FH (Figure 5); Internal structure: cranial deflection, anterior cranial length, ramus Xi position, porion location, mandibular arc, and corpus length (Figure 6).
Figure 2.

Measurements of dental relationships. A, Molar relationship; B, incisor overjet; C, incisor overbite; D, mandibular incisor extrusion; E, interincisor angle. A1, Maxillary incisor; B1, mandibular incisor; A6, maxillary first molar; B6, mandibular first molar.
Figure 3.

Measurements of dental to skeletal relationship. A, Distance of A6 to PTV, parallel to the occlusal plane; B, perpendicular distance of B1 to A-PO plane; C, perpendicular distance of A1 to A-PO plane; D, B1 inclination to A-PO and A1 inclination to A-PO; E, B1 inclination to FH.
PTV, Pterygoid true vertical plane; A-PO plane, A point-Pogonion plane.
See Figure 1 for the definitions of all the landmarks and measurements.
Figure 4.

Measurements of skeletal relationships. A, Convexity, which indicates a perpendicular distance of A point to the facial plane; B, lower facial height, which indicates an angle between ANS-XI and XI-PM. Facial plane indicates a Nasion-Pogonion line.
See Figure 1 for the definitions of all the landmarks and measurements.
Figure 5.

Measurements of the jaw to cranium relationship. A, Facial depth; B, facial axis; C, maxillary depth; D, maxillary height; E, palatal plane to FH.
See Figure 1 for the definitions of all the landmarks and measurements.
Figure 6.

Measurements of internal structures. A, Cranial deflection; B, anterior cranial length; C, ramus Xi position; D, porion location; E, mandibular arc and corpus length.
See Figure 1 for the definitions of all the landmarks and measurements.
Data analysis and statistical treatment
Statistical analysis was conducted using the SPSS program ver. 17.0 (SPSS Inc., Chicago, IL, USA). The means and standard deviations for each measurement of the subjects at age 9 were determined; changes in measurements over the 10 years that did not exceed one standard deviation (SD) of the 10-year change were defined as unchanged.10 For the parameters that showed gradual changes with age, we used the Kolmogorov-Smirnov test to determine normality; once normality was proven, the annual average growth was calculated.14 The measurements were compared according to sex using the t-test. To avoid intraobserver error, 20 lateral cephalometric radiographs were randomly selected and the same examiner conducted the tracings twice, with 20 days between the measurements; a test for normality followed. To verify inter-observer reliability, 20 lateral cephalometric radiographs were randomly selected, and a different examiner repeated the tracing and measuring. The measurements proven to have normality were analyzed using the paired t-test, while those without normality were analyzed using the Wilcoxon signed rank test.14 The intra- and inter-observer errors had no statistical significance. The ranges of intra- and inter-observer errors were calculated using Dahlberg's formula. The intraobserver error was 0.3 mm linearly and 0.3° angularly, while the inter-observer error was 0.3 mm linearly and 0.2° angularly.
RESULTS
The norms and standard deviations of the subjects' measurements at age 9 are shown in Table 1. The molar relationship was -1.8±1.1 mm, with the negative value indicating that the upper first molar was located distal to the lower first molar. The porion location also showed a negative value, indicating that porion was located posterior to PTV.
Table 1.
Clinical norms of Koreans for the Ricketts' analysis (age 9 years)

See Figure 1 for the definitions of all the landmarks and measurements.
The parameters that exhibited no change with age included: molar relationship, incisor overjet, incisor overbite, mandibular incisor extrusion, interincisor angle, B1 to A-PO plane, A1 to A-PO plane, B1 inclination to A-PO, A1 inclination to A-PO, B1 inclination to FH, convexity, lower facial height, facial axis, maxillary depth, maxillary height, palatal plane to FH, cranial deflection, ramus Xi position, and porion location. The mean 10-year changes in these parameters were less than one SD of the mean 10-year changes. The mean values and standard deviations at each age are shown in Table 2.
Table 2.
Unchanged cephalometric values in the Ricketts' analysis

Data are presented as value (standard deviation).
M, Male; F, female.
*Significant difference between males and females at 0.05% level by t-test; †significant difference between males and females at 0.01% level by t-test.
See Figure 1 for the definitions of all the landmarks and measurements.
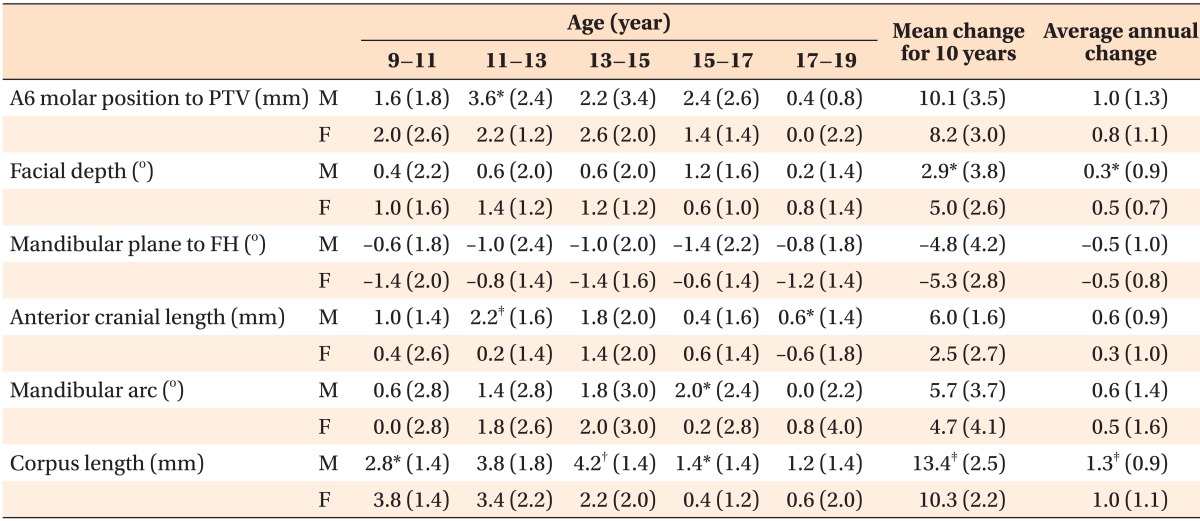
The parameters that showed gradual changes in growth with age were the A6 molar position to PTV, facial depth, mandibular plane to FH, anterior cranial length, mandibular arc, and corpus length (Table 3). We estimated the growth increment (SD), mean change in 10 years (SD), and the mean annual growth (SD) (Table 4).
Table 3.
Changes in cephalometric values for the Ricketts analysis

Data are presented as value (standard deviation).
M, Male; F, female.
*Significant difference between males and females at 0.05% level by t-test; †significant difference between males and females at 0.01% level by t-test.
See Figure 1 for the definitions of all the landmarks and measurements.
Table 4.
Comparison of parameters with changed cephalometric values between males and females
Data are presented as value (standard deviation).
*Significant difference between males and females at 0.05% level by t-test; †significant difference between males and females at 0.01% level by t-test; ‡significant difference between males and females at 0.001% level by t-test.
See Figure 1 for the definitions of all the landmarks and measurements.
DISCUSSION
Observation of our subjects over a period of 10 years revealed significant changes in the A6 molar position to PTV, facial depth, mandibular plane to FH, anterior cranial length, mandibular arc, and corpus length.
Because the development of the craniofacial region varies with age, accurate prediction of the changes that will occur with growth is critical for the establishment of a treatment plan.12 Such predictions are especially important during adolescence, when the majority of growth takes place and most treatment of malocclusions are administered. References for measuring growth with respect to age are necessary when predicting the changes that will occur with growth. Visual treatment objectives, used to set treatment goals that take growth into consideration, were developed by Ricketts et al.15,16 The present study sought to determine Korean norms for these Ricketts measurements by observing growth in our subjects throughout adolescence, which had not yet been longitudinally studied.
Ricketts15 noted that craniofacial growth takes place primarily in the anteroposterior and vertical directions while horizontal maxillofacial growth is minimal. Furthermore, he reported that since the direction of orthodontic treatment is anteroposterior and vertical, lateral cephalometric radiography should be used for assessment of these dimensions. Many investigators3,4,5,6,7 have also used lateral cephalometric radiography for orthodontic analysis. We thus used lateral cephalometric radiography in this investigation, and studies using frontal cephalometric radiographs were excluded from our discussion.
There were statistically significant differences between male and female subjects at age 9 (Table 2). Females had a higher value than males for incisal overjet and convexity. This indicates that the female profile was more protrusive than that of males. On the contrary, according to the interincisal angle and distance of B1 to A-PO and the inclination of B1 to A-PO, the male profile was more protrusive. The small sample size used in this study might have contributed to this conflicting data.
Ricketts10 reported in his 10-year longitudinal study on 50 subjects that the amount of growth during 10 years is sufficient to negate measurement errors and to make a judgment whether actual growth has taken place; therefore, if the 10-year growth has a lesser value than the SD of the 10-year growth change, it is hard to say whether growth has taken place. Using this principle, we identified parameters that were unchanged with age, including the molar relationship, incisor overjet, incisor overbite, mandibular incisor extrusion, interincisor angle, B1 to A-PO plane, A1 to A-PO plane, B1 inclination to A-PO, A1 inclination to A-PO, B1 inclination to FH, convexity, lower facial height, facial axis, maxillary depth, maxillary height, palatal plane to FH, cranial deflection, ramus Xi position, and porion location (Table 2).
We identified that the molar relationship did not change in either sex. Overall, the rest of the measurements tended to increase negatively, which appears to be due to the late mesial shift of the mandibular first molar that takes place throughout the mixed dentition phse.
Downs2 defined the A-PO plane as the line between the most anterior part of the basal bone of the maxilla and mandible. Accordingly, Ricketts17 set this plane as the reference line for determining the position of the anterior teeth. The position of the mandibular anterior teeth with respect to the A-PO plane particularly affects the facial aesthetics and is thus an important measurement for making extraction decisions. Our results indicate that the distance and angle between A-PO and B1 did not change with age, supporting the findings of previous studies.11,15,18,19
Downs2,8 used the Y-axis angle (the angle between S-Gn and FH) to indicate the direction of mandibular growth. He noted that there was little difference in this parameter between age groups. Brodie20 used SNGn (Sella-nasion plane-gnathion) and also reported no difference with age. Ricketts21,22 suggested that the facial axis is the most reliable reference for forecasting mandibular growth and noted that there is little change in this parameter with age. Together with our observation indicating little change in mandibular growth, these data suggest that the direction of mandibular growth is uniform over time.
Brodie20 reported that the growth of the nasal floor maintains an almost constant angle to the SN line or the craniofacial base, and that anterior nasal spine (ANS) tends to grow slightly inferior to posterior nasal spine (PNS). Ricketts23 noted that the angle of the palatal plane to the FH plane remains at 1.0 ± 3.0°, changing very little with age. In this study, the mean palatal plane angle at age 9 was 0.4 ± 2.5°, similar to that of the Caucasian counterpart. This angle remained the same throughout the growth span, with a mean palatal plane angle for all ages of 0.6 ± 2.6°.
In a study of facial bone changes with growth, Nanda24 reported that the change in SNA over 12 years was less than 1 degree, a negligible change. Williams25 reported that the distance from A to SN (X) and from A to the baseline (Y), passing through S and perpendicular to SN, remains stable in adolescents with normal occlusions. The horizontal position of the maxilla, as represented by maxillary depth, did not change with age in this study. This observation corresponds with the results of studies using Caucasian and Japanese subjects.
A study of Caucasian subjects by Ricketts15 reported that the convexity was 2.0 ± 2.0 mm, with an annual change of -0.33 mm, while Nezu et al.18 found that in the Japanese, the convexity was 4.0 ± 2.0 mm with a -0.2 mm annual change. Both studies thus indicate that this parameter changes with age. In this study, we observed a convexity of 1.9 ± 2.2 mm in males and 2.7 ± 2.9 mm in females. The SD for the 10-year change was greater than the 10-year change and was therefore defined as unchanged.
In this study, the parameters showing continuous change with age were the A6 molar position to PTV, facial depth, mandibular plane to FH, anterior cranial length, mandibular arc, and corpus length. We determined the means and standard deviations for the 10-year change and the average annual growth. The A6 molar position to PTV differed significantly between males and females at the ages of 11-13 years. The greatest incremental growth was 3.6 mm, occurring at ages 11-13 years in males. It should be noted that the growth increment rapidly diminishes after the age of 17 in both sexes. Therefore, a male aged 11-13 years experiences the greatest incremental growth in the A6 molar position to PTV. After age 17, space formation by additional growth of the maxillary posterior area is minimal. These factors should be taken into account when the maxillary molar distalization was needed in case of class II malocclusion.
Facial depth refers to the facial angle used in Downs' analysis2 and indicates the anteroposterior position of the mental region. Downs8 concluded from studies of facial bone growth in subjects aged 9-14 years that normal growth changes in the lower part of the face or mandible occurs more rapidly than in the maxilla; thus, the facial angle gradually increases from 82° to 88°. This conclusion corresponds with previous reports11,15,18,19 and with our results as well.
Ricketts22 suggested that once the position of the symphysis is decided by the facial axis and facial angle, the mandibular plane angle represents the vertical height of the ramus. Therefore, a high mandibular plane angle indicates that the ramus has a short vertical height, which occasionally occurs due to disease of the condyle head, changes in growth potential, or inappropriate musculature. A lower mandibular plane angle indicates a sound condyle and musculature. Therefore, "low angle cases" respond better to deep bite treatment involving eruption of the posterior teeth. In this study, the mandibular plane was observed to have a decreasing tendency over ten years in both sexes. A similar tendency was reported by Hamm and Sohn11 and in studies of Caucasian15 and Japanese18,19 subjects. In patients with normal skeletal growth, the continual decrease in the mandibular plane angle takes place until the age of 19. The application of the bite turbo or anterior bite plate to erupt the posterior teeth is thus more effective than intruding the anterior teeth when treating deep bites.
In his study of implants, Björk26 reported that because of resorptive changes to the lower border of the mandible, the mandibular plane is not suitable to serve as a reference line for mandibular growth. Enlow27 noted that because severe remodeling takes place to the ramal surface, the center of the ramus is not a reliable reference line. To investigate growth of the mandible, Ricketts28 therefore used the condyle axis and corpus axis, defined as the line connecting Xi (the center of the ramus) and Pm (a stable suprapogonion of the mandibular symphysis) and the line between Xi and DC, a bisecting point of the condylar neck.
Ricketts22 reported that the mandibular arc gradually increases with age because the distal growth of Xi is greater than the growth of the condyle. Such a pattern was also observed in this study and in studies on Japanese subjects.18,19 A significant difference in the mandibular arc was observed between males and females aged 15-17 years, indicating that growth of the mandibular arc continues to change for a longer period of time in males.
According to this study, the corpus length increases with age, as observed in studies on Caucasian and Japanese subjects. We observed a significant difference in corpus length changes between males and females at ages 9-11, 13-15, and 15-17 years. This observation indicates that the pubertal growth peak in males starts later and continues longer than that of females.
Nezu et al.18 reported that the completion of growth occurs at different ages in males and females-age 15 years in females and 18 years in males. We observed no significant difference in the growth increment between the sexes after 15 years of age in the A6 molar position to PTV, facial depth, or mandibular plane to FH. However, a significant difference in the growth increment between the sexes after age 15 was observed in the anterior cranial length, mandibular arc, and corpus length.
This longitudinal study is limited by the small sample size. Thus, further studies on growth completion differences between the sexes are needed. Ricketts29 reported that a size difference occurs when linearly measuring a 3-dimensional cephalic region and that other factors should be assessed to make size corrections. Such corrections were not performed in this study. Therefore, further studies that include size corrections or use computed tomography for 3-dimensional growth analysis are needed.
CONCLUSION
A total of 31 Korean subjects aged 9 to 19 years with normal occlusions were assessed using biennial lateral cephalometric radiographs to determine the parameters to use when applying the Ricketts analysis. The Korean norms for the Ricketts analysis at age 9 were determined. Some parameters did not change in value, while others changed continuously over the ten-year study period. The parameters that changed with age showed different growth rates between the sexes. A patient's age at the beginning of treatment and their sex should be taken into consideration when drawing visual treatment objectives.
Footnotes
This research was supported by the Kyungpook National University Research Fund, 2012.
The authors report no commercial, proprietary, or financial interest in the products or companies described in this article.
References
- 1.Broadbent BH. A new X-ray technique and its application to orthodontia. Angle Orthod. 1931;1:45–66. [Google Scholar]
- 2.Downs WB. Variations in facial relationships; their significance in treatment and prognosis. Am J Orthod. 1948;34:812–840. doi: 10.1016/0002-9416(48)90015-3. [DOI] [PubMed] [Google Scholar]
- 3.Steiner CC. Cephalometrics for you and me. Am J Orthod. 1953;39:729–755. [Google Scholar]
- 4.Sassouni V. A roentgenographic cephalometric analysis of cephalo-facio-dental relationships. Am J Orthod. 1955;41:735–764. [Google Scholar]
- 5.Ricketts RM. A foundation for cephalometric communication. Am J Orthod. 1960;46:330–357. [Google Scholar]
- 6.Tweed CH. Was the development of the diagnostic facial triangle as an accurate analysis based on fact or fancy? Am J Orthod. 1962;48:823–840. doi: 10.1016/0002-9416(62)90002-7. [DOI] [PubMed] [Google Scholar]
- 7.Jarabak JR. Technique and treatment with light wire edgewise appliance. 2nd ed. St. Louis: C.V. Mosby; 1972. pp. 128–166. [Google Scholar]
- 8.Downs WB. Analysis of the dentofacial profile. Angle Orthod. 1956;26:191–212. [Google Scholar]
- 9.Sassouni V. The face in five dimensions. Philadelphia: Growth Center Publication; 1960. [Google Scholar]
- 10.Ricketts RM. A four-step method to distinguish orthodontic changes from natural growth. J Clin Orthod. 1975;9:208–215. 218–228. [PubMed] [Google Scholar]
- 11.Hamm SM, Sohn BH. Roentgenocephalometric study of craniofacial growth by Ricketts analysis on teen-ager with normal occlusion in Korean. Korean J Orthod. 1985;15:313–326. [Google Scholar]
- 12.Park TS. A longitudinal cephalometric study of craniofacial growth of Korean children. Korean J Orthod. 1984;14:217–231. [Google Scholar]
- 13.Kim YJ, Park KD, Kwon OW. A longtudinal cephalometric study of the craniofacial growth changes of adolescence with normal occlusion. Korean J Orthod. 1995;25:287–297. [Google Scholar]
- 14.Houston WJ. The analysis of errors in orthodontic measurements. Am J Orthod. 1983;83:382–390. doi: 10.1016/0002-9416(83)90322-6. [DOI] [PubMed] [Google Scholar]
- 15.Ricketts RM. Orthodontic diagnosis and planning. Philadelphia: Saunders; 1982. [Google Scholar]
- 16.Ricketts RM, Bench RW, Gugino CF, Hilgers JJ, Schulhof RJ. Bioprogressive therapy. Denver: Rocky Mountain/Orthodontics; 1979. [Google Scholar]
- 17.Ricketts RM. Cephalometric analysis and synthesis. Angle Orthod. 1961;31:141–156. [Google Scholar]
- 18.Nezu H, Nagata K, Yoshida Y, Kosaka H, Kikuchi M. Cephalometric comparison of clinical norms between the Japanese and Caucasians. Nihon Kyosei Shika Gakkai Zasshi. 1982;41:450–465. [PubMed] [Google Scholar]
- 19.Engel G, Spolter BM. Cephalometric and visual norms for a Japanese population. Am J Orthod. 1981;80:48–60. doi: 10.1016/0002-9416(81)90195-0. [DOI] [PubMed] [Google Scholar]
- 20.Brodie AG. Late growth changes in the human face. Angle Orthod. 1953;23:146–157. [Google Scholar]
- 21.Ricketts RM. The influence of orthodontic treatment on facial growth and development. Angle Orthod. 1960;30:103–133. [Google Scholar]
- 22.Ricketts RM. Perspectives in the clinical application of cephalometrics. The first fifty years. Angle Orthod. 1981;51:115–150. doi: 10.1043/0003-3219(1981)051<0115:PITCAO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 23.Ricketts RM. Cephalometric synthesis. Am J Orthod. 1960;46:647–673. [Google Scholar]
- 24.Nanda RS. Growth changes in skeletal-facial profile and their significance in orthodontic diagnosis. Am J Orthod. 1971;59:501–513. doi: 10.1016/0002-9416(71)90085-6. [DOI] [PubMed] [Google Scholar]
- 25.Williams BH. Craniofacial proportionality in a horizontal and vertical plane, a study in norma lateralis. Angle Orthod. 1953;23:26–34. [Google Scholar]
- 26.Björk A. Prediction of mandibular growth rotation. Am J Orthod. 1969;55:585–599. doi: 10.1016/0002-9416(69)90036-0. [DOI] [PubMed] [Google Scholar]
- 27.Enlow DH. The human face; an account of the postnatal growth and development of the craniofacial skeleton. New York: Hoeber; 1968. [Google Scholar]
- 28.Ricketts RM. A principle of arcial growth of the mandible. Angle Orthod. 1972;42:368–386. doi: 10.1043/0003-3219(1972)042<0368:APOAGO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 29.Ricketts RM. The value of cephalometrics and computerized technology. Angle Orthod. 1972;42:179–199. doi: 10.1043/0003-3219(1972)042<0179:TVOCAC>2.0.CO;2. [DOI] [PubMed] [Google Scholar]