

Abstract
Objective
The purpose of this study was to compare the treatment duration and dentoskeletal changes between two different anchorage systems used to treat maxillary dentoalveolar protrusion and to examine the effectiveness of en-masse retraction using two miniscrews placed in the midpalatal suture.
Methods
Fifty-seven patients (9 men, 48 women), who had undergone level anchorage system treatment at Aichi-Gakuin University Dental Hospital (Nagoya, Japan) were divided into two groups according to the method of maxillary posterior anchorage reinforcement: midpalatal miniscrews (25 patients, mean age 22 years) and conventional anchorage (32 patients, mean age 19 years). The en-masse retraction period, overall treatment duration, pre-treatment effective ANB angle, and change in the effective ANB angle were compared with an independent-samples t-test.
Results
Compared to the headgear group, the duration of en-masse retraction was longer by approximately 4 months in the miniscrew group (p < 0.001). However, we found no significant difference in the total treatment duration between the groups. Moreover, a greater change in the effective ANB angle was observed in patients treated with miniscrews than in those treated with the conventional method (p < 0.05).
Conclusions
The level anchorage system treatment using miniscrews placed in the midpalatal area will allow orthodontists more time to control the anterior teeth during en-masse retraction, without increasing the total treatment duration. Furthermore, it achieves better dentoskeletal control than does the conventional anchorage method, thereby improving the quality of the treatment results.
Keywords: Orthodontic mini-implant, Appliances, Diagnosis and treatment planning, Orthodontic treatment
INTRODUCTION
Maxillary dentoalveolar protrusion is one of the chief complaints in adult orthodontic patients. For the correction of dentoalveolar protrusion, the bilateral premolars are commonly extracted to provide space for anterior retraction.1 When the extraction of maxillary premolars is indicated for Class II or Class I malocclusion, the technique must be designed to maximize anterior tooth retraction2 and to minimize mesial movements of the maxillary molars, until dental crowding and dentoalveolar protrusion are corrected.3
Several attempts have been made to develop stable anchorage. However, it has been difficult to establish absolute anchorage with traditional extraoral or intraoral appliances such as high-pull headgear and intermaxillary elastics. Most intraoral anchorage devices were associated with some loss of anchorage. Extraoral appliances, on the other hand, can provide reliable anchorage, but only for patients who cooperate properly.
Recently, miniscrews have been used for skeletal anchorage. Even without patient cooperation, it is now possible to prevent anchorage loss of the maxillary posterior teeth during en-masse retraction and close the extraction spaces completely by anterior tooth retraction.4,5 Midpalatal miniscrews are especially useful for orthodontic tooth movements with minimal anatomic limitations on placement, lower medical costs, and simpler placement with less traumatic surgery.6,7,8
There have been several reports about patients treated with incisor retraction with miniscrews after premolar extractions.4,9 However, there is little accurate scientific evidence pertaining to the treatment effectiveness of skeletal anchorage. Although recent advances in orthodontic techniques, such as orthodontic miniscrews, allow maximum anchorage and further simplify the procedure,10,11 biomechanical considerations and special concerns regarding facial esthetics should be addressed for efficient orthodontic treatment of patients with maxillary dentoalveolar protrusion. Moreover, to determine the overall treatment effectiveness, it is important to evaluate the entire treatment duration, from appliance placement to removal on completion. Success in orthodontic practice is also related to accurate prediction of the treatment duration, which is dependent on several factors.12,13,14 Moreover, the time effect of miniscrew anchorage remains controversial.15,16
The purposes of this study were to compare treatment duration and dentoskeletal changes between two different anchorage systems used to treat adult patients with maxillary dentoalveolar protrusion and to evaluate the effectiveness of en-masse retraction using midpalatal miniscrews and a modified transpalatal arch.
MATERIALS AND METHODS
Samples
The clinical records of consecutive patients, who had undergone level anchorage system treatment at Aichi-Gakuin University Dental Hospital (Nagoya, Japan), between 2008 and 2011, were searched to identify appropriate subjects. A total of 57 subjects (9 men and 48 women) met the inclusion and exclusion criteria, which were described in our previous study.17 The common feature of these patients was maxillary dentoalveolar protrusion, which required the extraction of bilateral maxillary first premolars and maximum anchorage during en-masse retraction. The subjects were divided into two groups according to the method of maxillary posterior anchorage reinforcement (Table 1). There was no significant age difference between the two groups.
Table 1.
Demographic information for the 57 subjects in this study
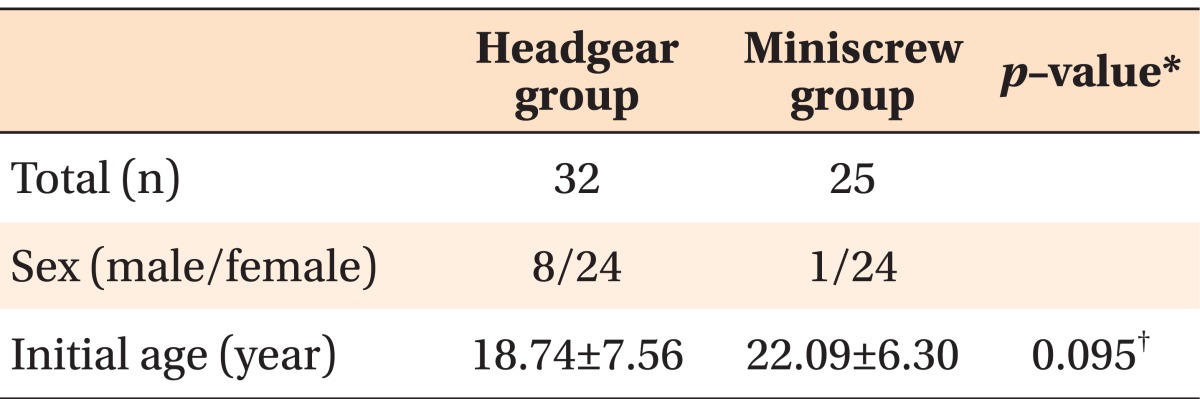
*Independent-samples t-test.
†Not significant.
The high-pull headgear group included 32 patients who received traditional anchorage reinforcement with a high-pull headgear, a traditional transpalatal arch, and intermaxillary elastics (Figure 1). After the initial leveling and aligning in the maxillary arch, maxillary posterior anchorage was reinforced with a high-pull headgear, and Class III elastics were used to perform anchorage preparation to upright the mandibular molars. After stabilization of the mandibular arch, high-pull headgear and Class II elastics were used during the maxillary en-masse retraction. All subjects were instructed to wear the high-pull headgear for 10-12 hours per day throughout the treatment period and to record the time when the headgears were worn in the daily charts. A force of approximately 250 gm on each side was applied at the level of the buccal trifurcation (center of resistance) of the maxillary first molars. The importance of wearing the extraoral appliance as anchorage was explained at the initial stage and reiterated throughout active treatment.
Figure 1.
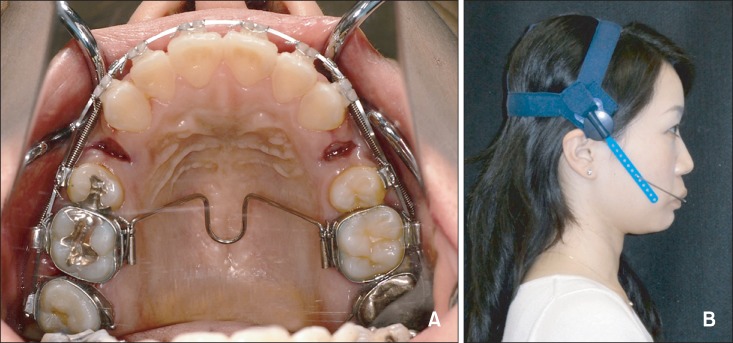
The anchorage reinforcing appliances in the headgear group. A, The maxillary first molars were stabilized with a conventional transpalatal arch. B, High-pull headgear.
The miniscrew group consisted of 25 patients who received implantation of two self-drilling miniscrews (Induce MS-II, GC Ortholy, Tokyo, Japan; diameter, 1.8 mm, length, 6.0 mm; and Dual-Top Anchor, Jeil Medical, Seoul, Korea; diameter, 2.0 mm, length, 6.0 mm) in the midpalatal suture. Only one experienced orthodontist (K.M.) placed all the miniscrews without flap elevation under local anesthesia according to the manufacturer's guidelines. In this study, a midpalatal surgical guide stent was used, and cone-beam computed tomography was performed before and after miniscrew surgery to ensure the correct position and direction for insertion.18 After two weeks of healing, the two midpalatal miniscrews were connected with a horizontal 0.030-inch stainless steel ligature wire (Figure 2A). The horizontal ligature wire provided support where the vertical ligature wires were firmly tied, enabling them to fasten a modified transpalatal arch (M-TPA). After the initial leveling and aligning in the maxillary arch, the maxillary posterior anchorage was reinforced with the miniscrew-supported M-TPA (Figure 2B).
Figure 2.

The anchorage reinforcing appliances in the miniscrew group. A, Two miniscrews were placed about 5-8 mm apart in the midpalatal suture area and fixed with a stainless steel ligature wire. B, The maxillary first molars were held with a modified transpalatal arch, and were assisted with skeletal anchorage during en-masse retraction.
Treatment protocol
The appliances and protocol used for en-masse retraction are described in Figures 3 and 4. All subjects were treated with preadjusted edgewise appliances, 0.018 × 0.025-inch slot level anchorage system prescription brackets (3M Unitek, Monrovia, CA, USA).19 The same treatment protocol was applied to both the groups, with the exception of the method of anchorage reinforcement. Maxillary posterior anchorage was reinforced with high-pull headgear or miniscrew-supported M-TPA in each group. In both the groups, six maxillary anterior teeth were retracted on a 0.017 × 0.025-inch nickeltitanium archwire with 0.010 × 0.036-inch stainless steel closed coil springs, which were stretched two-thirds of the distance from the maxillary first molars to the crimpable hooks located mesial to the canines. Gable bends of 45 degrees were placed in the extraction sites to prevent tipping of the maxillary incisors lingually during the en-masse retraction. When the extraction space measured 2.3 mm, a 0.018 × 0.025-inch stainless steel archwire with keyhole loops was used for root control in the extraction sites, torque control of the maxillary anterior teeth, and final space closure. Anchorage reinforcement was continued until the extraction space was closed.
Figure 3.

The maxillary en-masse retraction in the headgear group. A, The mandibular arch was stabilized for the use of Class II elastics. B and C, The maxillary first premolar extraction space closure with Class II elastics. D, Post-treatment photograph.
Figure 4.

The maxillary en-masse retraction in the miniscrew group. A, The mandibular arch was not yet stabilized. B and C, The maxillary first premolar extraction space closure without Class II elastics. D, Posttreatment photograph.
Statistical analyses
To evaluate the effectiveness of orthodontic treatment in subjects who had undergone level anchorage system treatment with two different anchorage systems, the en-masse retraction period, overall treatment duration, pre-treatment effective ANB angle, and change in the effective ANB angle were compared with an independent-samples t-test. All statistical analyses were performed using GraphPad Prism v.4 (GraphPad Software, San Diego, CA, USA). The levels of statistical significance were p < 0.05, p < 0.01, and p < 0.001, respectively.
RESULTS
Treatment duration
The mean durations required for en-masse retraction were 343.41 ± 99.80 days in the headgear group and 462.32 ± 134.78 days in the miniscrew group (Table 2). The time taken for en-masse retraction was increased by approximately 4 months in the miniscrew group. The period of maxillary anterior retraction was significantly longer in the miniscrew group than in the headgear group (p < 0.001). Although the mean time of retraction in the miniscrew group was significantly longer than that in the headgear group, there was no significant difference in the total treatment duration between the two groups (Table 2). The total treatment duration was shorter in the miniscrew group than in the headgear group (1,096.20 ± 228.88 days vs. 1,143.37 ± 303.69 days). However, we found no significant difference between the two groups.
Table 2.
Comparison of treatment duration between two groups

*Independent-samples t-test.
†p < 0.01; ‡not significant.
Dentoskeletal changes (effective ANB angle)
The change in the effective ANB angle was used as an outcome measure for the degree of improvement. The pre-treatment effective ANB angle provided an estimate for the severity of the initial malocclusion. The difference in the effective ANB angle between pre-treatment and post-treatment stages reflected the degree of improvement and therefore the effectiveness of treatment.
The pre-treatment effective ANB angle was significantly larger in the miniscrew group than in the headgear group (8.93 ± 2.43° vs. 5.62 ± 2.13°) (p < 0.001). The changes in the effective ANB angle, achieved by treatment, in the headgear group and in the miniscrew group were 0.94 ± 0.54° and 2.14 ± 0.32°, respectively (Table 3). A greater change in the effective ANB angle was observed in patients treated with miniscrews than in those treated with the conventional method (p < 0.05).
Table 3.
Comparison of dentoskeletal measurements between two groups
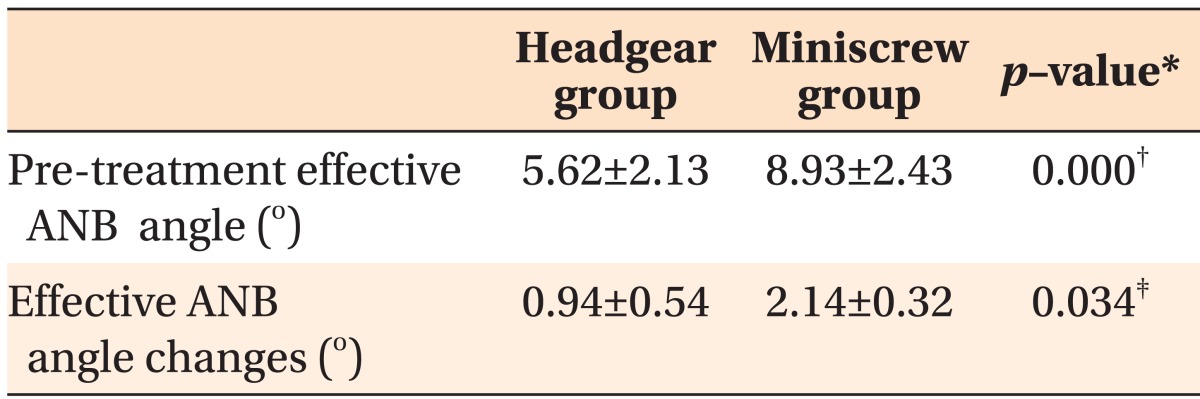
*Independent-samples t-test.
ANB angle, A point-Nasion-B point angle.
†p < 0.001; ‡p < 0.05.
DISCUSSION
Conventionally, various anchorage reinforcement appliances have been used, including headgear, lingual arch, transpalatal arch, and intermaxillary elastics. These auxiliaries help to achieve acceptable interincisal relationships and reduce overjet with good patient cooperation. In this study, orthodontic treatment combined with either miniscrew anchorage or high-pull headgear has been shown to achieve acceptable results with reduction of overjet and improvement in facial profile in patients with lip protrusion.
However, en-masse retraction with miniscrew anchorage did not require patient cooperation to reinforce the anchorage and provided more significant improvement in the effective ANB angle than that with traditional anchorage mechanics such as high-pull headgear combined with a transpalatal arch. Successful orthodontic treatment depends on a variety of factors. Although the knowledge and skills of the clinician remain significant, the cooperation of the patient plays a major role in achieving the desired results.20,21 In fact, the effectiveness and duration of orthodontic treatment is considered to depend largely on patient cooperation.22,23,24
The conventional level anchorage system treatments require the use of Class II elastics and high-pull headgear to help maintain the anchorage of the maxillary posterior teeth (Figure 5A). The use of intermaxillary elastics has been a standard procedure for the correction of Class II, Division 1 malocclusion since the early days of orthodontic treatment. However, it is well documented in the literature that although intermaxillary elastics are effective in correcting the anteroposterior relationship of the dentition, undesirable side effects can occur. Class II elastics have been associated with some undesirable side effects such as loss of mandibular anchorage, proclination of mandibular incisors, and extrusion of maxillary incisors.25,26 The horizontal vector of Class II elastic force has been shown to cause the mandibular first molars to rotate or tip mesially, procline the mandibular anterior teeth, and displace the entire lower dental arch anteriorly.25,27 Moreover, the use of high-pull headgear has its inherent disadvantages related to compliance and duration of wear, non-compliance in many adults, and risks of potential injury. Therefore, M-TPA supported by two midpalatal miniscrews is used to prevent anchorage loss when retracting the maxillary anterior teeth. It is thus possible to make maximum use of the extraction space without wearing Class II elastics in the miniscrew group (Figure 5B).
Figure 5.

The maxillary en-masse retraction. A, Headgear group. Extraction space is closed partially by maxillary molar loss. Class II elastics are used to correct the anteroposterior relationship of the dentition. B, Miniscrew group. The combination of two midpalatal miniscrews and a modified transpalatal arch serve as a skeletal anchorage. This miniscrew anchorage system allows the maxillary anterior teeth to be retracted effectively without undesirable side-effects such as anchorage loss. There is no need to wear Class II elastics to retract the maxillary incisors and to maintain the molar relationship.
Treatment duration
The period of maxillary en-masse retraction was significantly longer in the miniscrew group than in the conventional anchorage group. A possible explanation could be that, with miniscrews, closure of the extraction space was mostly done by distalization of the anterior teeth, whereas, in the headgear group, the anterior and posterior teeth moved simultaneously in the extraction space. Therefore, the en-masse retraction distance increased in the conventional anchorage group. In addition, the en-masse retraction force decreased as a result of not using class II elastics, resulting in increased en-masse retraction duration. Miniscrew anchorage, because of less anchorage loss and increased extraction space, allows for greater orthodontic incisor movement in more severe patients. On the other hand, the treatment duration needed for the greater amount of en-masse retraction in the miniscrew group was also significantly longer. The miniscrew anchorage enabled greater en-masse retraction but required a longer en-masse retraction time in more severe cases.
Nevertheless, we found no significant difference in the total treatment duration between the two groups. For minimizing anchorage loss and maximizing en-masse retraction during extraction space closure, Tweed28 emphasized anchorage preparation as the first step in orthodontic treatment. In the headgear group, stabilization in the lower arch as well as anchorage preparation should be established to use Class II elastics during en-masse retraction. Stabilization of the mandibular arch involved full appliances, a well-aligned mandibular arch, and placement of a rectangular ideal arch. After the stabilization, extra- or intraoral appliances.such as high-pull headgear, transpalatal arch, and Class II elastics.were used for anchorage control during en-masse retraction. However, in the miniscrew group, it was possible to begin en-masse retraction before stabilization of the mandibular arch because Class II elastics were not used during en-masse retraction. This might explain why there was no significant difference in the total treatment duration between the two groups.
Dentoskeletal changes
Treatment outcome can be assessed in many ways, but effective ANB angle gives a clear and simple indication of the anteroposterior relationship.19 In more severe cases, the effective ANB angle showed a greater change in the miniscrew group. Furthermore, we found that the maxillary anterior teeth show a significantly larger amount of bodily retraction in the miniscrew group. In a previous study, we have reported cephalometric comparisons, between the same two groups, of treatment changes in vertical and anteroposterior skeletodental variables.17 That study also showed that the miniscrew group achieves better dentoskeletal control than does the high-pull headgear group.
In the treatment of premolar extraction in patients with traditional anchorage, the maxillary molars were usually mesialized approximately 30% into the extraction space, with excellent cooperation for maximum anchorage.29 In this study, the amount of overjet reduction was significantly different between the two groups, because the maxillary incisors were more retracted in the miniscrew group than in the conventional anchorage group. In other words, the treatment results in the miniscrew group showed more bialveolar dental protruded profiles than those in the headgear group. Therefore, from an esthetic viewpoint, treatment with traditional anchorage might be a compromise compared to treatment with miniscrew anchorage.
Compared with the headgear group, in the miniscrew group, as a result of reinforced anchorage with midpalatal miniscrews, the incisors were sufficiently retracted with less mesial movement of the maxillary molars. Minimum mesial movement of the maxillary molars would have occurred during leveling and alignment, because we usually implanted the miniscrews after the leveling phase.
We concluded that orthodontic treatment with miniscrew anchorage is simpler and more effective than traditional anchorage for patients with maxillary dentoalveolar protrusion. Because of sufficient retraction of the maxillary incisors, the upper lip in the miniscrew group was significantly retracted, and the facial profile was improved. In addition, miniscrews do not require patient cooperation for the attainment of stable anchorage.
CONCLUSION
The findings of this study show the effectiveness of miniscrew anchorage for en-masse retraction compared with traditional anchorage such as high-pull headgear and Class II elastics.
Miniscrew anchorage, used in level anchorage system treatment, will give orthodontists more time to control the maxillary anterior segments during en-masse retraction, without extending the total treatment duration.
Miniscrew anchorage achieves better dentoskeletal control than does the conventional anchorage method of level anchorage system treatment, thus improving the quality of the treatment results.
Footnotes
This study was supported by the Grant-in-Aid for Scientific Research from the Ministry of Education, Science and Culture of Japan (Subject No. 25463207).
The authors report no commercial, proprietary, or financial interest in the products or companies described in this article.
References
- 1.Bills DA, Handelman CS, BeGole EA. Bimaxillary dentoalveolar protrusion: traits and orthodontic correction. Angle Orthod. 2005;75:333–339. doi: 10.1043/0003-3219(2005)75[333:BDPTAO]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 2.Feldmann I, Bondemark L. Orthodontic anchorage: a systematic review. Angle Orthod. 2006;76:493–501. doi: 10.1043/0003-3219(2006)076[0493:OA]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 3.Braun S, Sjursen RC, Jr, Legan HL. On the management of extraction sites. Am J Orthod Dentofacial Orthop. 1997;112:645–655. doi: 10.1016/s0889-5406(97)70230-0. [DOI] [PubMed] [Google Scholar]
- 4.Park HS, Kwon TG. Sliding mechanics with microscrew implant anchorage. Angle Orthod. 2004;74:703–710. doi: 10.1043/0003-3219(2004)074<0703:SMWMIA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 5.Park YC, Chu JH, Choi YJ, Choi NC. Extraction space closure with vacuum-formed splints and miniscrew anchorage. J Clin Orthod. 2005;39:76–79. [PubMed] [Google Scholar]
- 6.Kyung SH. A study on the bone thickness of midpalatal suture area for miniscrew insertion. Korean J Orthod. 2004;34:63–70. [Google Scholar]
- 7.Kim YH, Yang SM, Kim S, Lee JY, Kim KE, Gianelly AA, et al. Midpalatal miniscrews for orthodontic anchorage: factors affecting clinical success. Am J Orthod Dentofacial Orthop. 2010;137:66–72. doi: 10.1016/j.ajodo.2007.11.036. [DOI] [PubMed] [Google Scholar]
- 8.Lee JS, Kim DH, Park YC, Kyung SH, Kim TK. The efficient use of midpalatal miniscrew implants. Angle Orthod. 2004;74:711–714. doi: 10.1043/0003-3219(2004)074<0711:TEUOMM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 9.Chae JM. A new protocol of Tweed-Merrifield directional force technology with microimplant anchorage. Am J Orthod Dentofacial Orthop. 2006;130:100–109. doi: 10.1016/j.ajodo.2005.10.020. [DOI] [PubMed] [Google Scholar]
- 10.Bae SM, Park HS, Kyung HM, Kwon OW, Sung JH. Clinical application of micro-implant anchorage. J Clin Orthod. 2002;36:298–302. [PubMed] [Google Scholar]
- 11.Thiruvenkatachari B, Pavithranand A, Rajasigamani K, Kyung HM. Comparison and measurement of the amount of anchorage loss of the molars with and without the use of implant anchorage during canine retraction. Am J Orthod Dentofacial Orthop. 2006;129:551–554. doi: 10.1016/j.ajodo.2005.12.014. [DOI] [PubMed] [Google Scholar]
- 12.Beckwith FR, Ackerman RJ, Jr, Cobb CM, Tira DE. An evaluation of factors affecting duration of orthodontic treatment. Am J Orthod Dentofacial Orthop. 1999;115:439–447. doi: 10.1016/s0889-5406(99)70265-9. [DOI] [PubMed] [Google Scholar]
- 13.Fisher MA, Wenger RM, Hans MG. Pretreatment characteristics associated with orthodontic treatment duration. Am J Orthod Dentofacial Orthop. 2010;137:178–186. doi: 10.1016/j.ajodo.2008.09.028. [DOI] [PubMed] [Google Scholar]
- 14.Skidmore KJ, Brook KJ, Thomson WM, Harding WJ. Factors influencing treatment time in orthodontic patients. Am J Orthod Dentofacial Orthop. 2006;129:230–238. doi: 10.1016/j.ajodo.2005.10.003. [DOI] [PubMed] [Google Scholar]
- 15.Upadhyay M, Yadav S, Nagaraj K, Patil S. Treatment effects of mini-implants for en-masse retraction of anterior teeth in bialveolar dental protrusion patients: a randomized controlled trial. Am J Orthod Dentofacial Orthop. 2008;134:18–29. doi: 10.1016/j.ajodo.2007.03.025. [DOI] [PubMed] [Google Scholar]
- 16.Yao CC, Lai EH, Chang JZ, Chen I, Chen YJ. Comparison of treatment outcomes between skeletal anchorage and extraoral anchorage in adults with maxillary dentoalveolar protrusion. Am J Orthod Dentofacial Orthop. 2008;134:615–624. doi: 10.1016/j.ajodo.2006.12.022. [DOI] [PubMed] [Google Scholar]
- 17.Lee J, Miyazawa K, Tabuchi M, Kawaguchi M, Shibata M, Goto S. Midpalatal miniscrews and high-pull headgear for anteroposterior and vertical anchorage control: cephalometric comparisons of treatment changes. Am J Orthod Dentofacial Orthop. 2013;144:238–250. doi: 10.1016/j.ajodo.2013.03.020. [DOI] [PubMed] [Google Scholar]
- 18.Miyazawa K, Kawaguchi M, Tabuchi M, Goto S. Accurate pre-surgical determination for self-drilling miniscrew implant placement using surgical guides and cone-beam computed tomography. Eur J Orthod. 2010;32:735–740. doi: 10.1093/ejo/cjq012. [DOI] [PubMed] [Google Scholar]
- 19.Root TL. The level anchorage system for correction of orthodontic malocclusions. Am J Orthod. 1981;80:395–410. doi: 10.1016/0002-9416(81)90174-3. [DOI] [PubMed] [Google Scholar]
- 20.Nanda RS, Kierl MJ. Prediction of cooperation in orthodontic treatment. Am J Orthod Dentofacial Orthop. 1992;102:15–21. doi: 10.1016/0889-5406(92)70010-8. [DOI] [PubMed] [Google Scholar]
- 21.Bartsch A, Witt E, Sahm G, Schneider S. Correlates of objective patient compliance with removable appliance wear. Am J Orthod Dentofacial Orthop. 1993;104:378–386. doi: 10.1016/S0889-5406(05)81337-X. [DOI] [PubMed] [Google Scholar]
- 22.Slakter MJ, Albino JE, Fox RN, Lewis EA. Reliability and stability of the orthodontic Patient Cooperation Scale. Am J Orthod. 1980;78:559–563. doi: 10.1016/0002-9416(80)90306-1. [DOI] [PubMed] [Google Scholar]
- 23.Allan TK, Hodgson EW. The use of personality measurements as a determinant of patient cooperation in an orthodontic practice. Am J Orthod. 1968;54:433–440. doi: 10.1016/0002-9416(68)90198-x. [DOI] [PubMed] [Google Scholar]
- 24.Starnbach HK, Kaplan A. Profile of an excellent orthodontic patient. Angle Orthod. 1975;45:141–145. doi: 10.1043/0003-3219(1975)045<0141:POAEOP>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 25.Bien SM. Analysis of the components of force used to effect distal movement of teeth. Am J Orthod. 1951;37:508–521. doi: 10.1016/0002-9416(51)90071-1. [DOI] [PubMed] [Google Scholar]
- 26.Hanes RA. Bony profile changes resulting from cervical traction compared with those resulting from intermaxillary elastics. Am J Orthod. 1959;45:353–364. [Google Scholar]
- 27.Meikle MC. The dentomaxillary complex and overjet correction in Class II, division 1 malocclusion: objectives of skeletal and alveolar remodeling. Am J Orthod. 1980;77:184–197. doi: 10.1016/0002-9416(80)90006-8. [DOI] [PubMed] [Google Scholar]
- 28.Tweed CH. The application of the principles of the edge-wise arch in the treatment of malocclusions: II. Angle Orthod. 1941;11:12–67. [Google Scholar]
- 29.Kocadereli I. The effect of first premolar extraction on vertical dimension. Am J Orthod Dentofacial Orthop. 1999;116:41–45. doi: 10.1016/s0889-5406(99)70301-x. [DOI] [PubMed] [Google Scholar]