

Abstract
In vitreoretinal surgery, application of excessive forces and unintentional motion due to hand-tremor can easily result in serious complications. Robotic assistance when combined with tool-to-tissue force sensing capabilities has significant potential to improve such practice. In this paper, we evaluate the membrane peeling performance of a single user for two distinct robotic systems with integrated force sensing capabilities: Micron and the Steady-Hand Robot. We show that these systems provide promising performance improvement with similar impact on peeling forces and comparable tremor cancellation trends.
I. Introduction
Retinal microsurgery involves the manipulation of extremely delicate tissues, which requires various micron scale maneuvers, precise manual dexterity, fine visual-motor coordination, and application of forces that are well below human tactile sensation. Among the vitreoretinal procedures, membrane peeling is a standard task, where the surgeon delaminates a very thin fibrous membrane on the retina surface by using either a hook or forceps. During this operation, the instruments are moved very slowly, within a range of 0.1–0.5 mm/s. Unintentional inaccurate tool motion and application of excessive forces can easily give rise to serious complications such as iatrogenic retinal breaks [2–4], vitreous hemorrhage as well as subretinal hemorrhage [5]. Hence for a successful operation, controlled tremor-free tool motion and limitation of applied forces on the retina are two highly desired features.
In order to reduce physiological hand tremor, provide fine motion control, and consequently enhance microsurgical accuracy, several robotic systems have been developed by different researchers [6–13]. In contrast to these teleoperated approaches, the Steady-Hand Robot was developed at JHU based on a cooperative control scheme between the surgeon and a stiff non-backdrivable robot arm [14–16]. Unlike any of these table-mounted systems, Micron was designed as a fully handheld instrument by Riviere et al. at CMU [17]. This robot could actively compensate for the motion due to hand-tremor in real time. On the other hand, focusing on the lack of force feedback problem, a family of instruments with force sensing capabilities was developed at JHU using fiber Bragg grating (FBG) strain sensors for measuring the forces directly at the tool tip [18–21].
In this paper, we integrate our force sensing tools on Micron and the Steady-Hand Robot to compare the performance and identify the limitations of these assistive systems. In the following sections, we will first present the structure of each system. This will be followed by the experiments on two types of phantoms, and our performance assessment based on measured peeling forces. The paper concludes with discussion of the results.
II. INSTRUMENTS
A. Micron
Micron is a handheld actively stabilized 3-DOF micromanipulator developed at the Robotics Institute at Carnegie Mellon University [17]. The device operates by activating three piezoelectric actuators based on the sensed motion of the handle. The position of the handle is determined by ASAP optical sensors. After sensing the tool motion, Micron separates it into involuntary components, such as hand tremor, and desired components. Then Micron moves its tip to counteract the involuntary motion component. The workspace of Micron is a 1×1×0.5 mm volume centered on the handle position. The device has about 1 N force capability, and bandwidth over 100 Hz.
B. Steady-Hand Robot
The Steady-Hand Robot is a cooperatively controlled, table mounted device, where the surgical tool is held simultaneously by the operator and an actively controlled robot arm. The robot utilizes XYZ linear stages for translation, a rotary stage for rolling, a tilting mechanism and a tool adaptor with a force sensor. By sensing the forces exerted by the operator on the tool, the robot actuates its arm in the direction of forced sensing to provide tremor-free precise motion control.
C. Force Sensing Tools
In order to measure forces in vitreoretinal microsurgery, a sensing instrument with sub-mN accuracy is required. The limited space and biocompatibility issues also need to be addresses in sensor selection. The force sensor has to be able to pass through a 23 Ga or 25 Ga sclerotomy opening so that the sensor can be located close to the tool tip. Only in this way can force measurements pertain solely to the instrument’s tip, with no contribution from the sclera. Under these limitations, we chose using FBGs, which are robust optical fibers capable of detecting changes in strain. A force sensing hook for Micron and micro-forceps for the Steady-Hand Robot were built integrating 3 FBG strain sensors on the tool shaft [19, 23]. Due to relative motion of Micron handle and its tool tip, designing a micro-forceps for this device is quite a challenge, and such a tool is not available yet.
The complete system is illustrated in Fig. 1. During the operation, the sensor data are collected and processed at 2 kHz and transmitted over TCP/IP. The sensed forces are converted into auditory signals [20]. Depending on the frequency of the auditory feedback (AF), the user adjusts tool motion so that the applied forces do not exceed 7.5 mN, which we define as the border for the danger zone based on our prior in-vivo experience [21].
Figure 1.
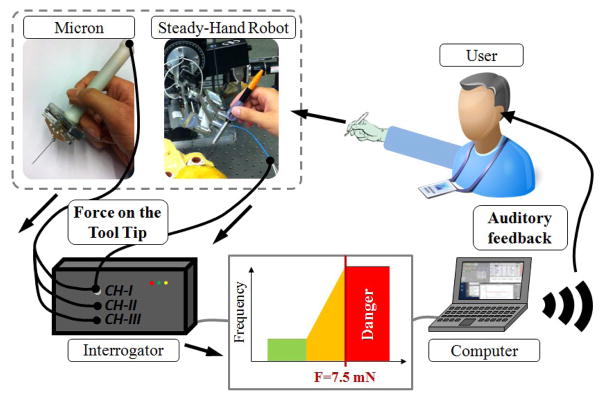
System overview with robotic assistance and integrated force sensing. Auditory feedback (AF) is provided to the user based on sensed forces on the tool tip.
III. Experiments
A. Setup
In order to assess the performance of the Steady-Hand Robot and Micron, a series of membrane peeling experiments were conducted. The setup for each device is presented in Fig. 2a and 2b respectively. Being a table mounted system, the Steady-Hand Robot has a larger footprint as compared to the hand-held Micron. On the other hand, Micron requires additional equipment, ASAP optical sensors, for tracking the tool motion. In both systems, the applied forces are monitored by using an FBG optical sensing interrogator, sm130–700 from Micron Optics Inc. (Atlanta GA). The tests were done on two types of phantoms, which have previously been reported to be suitable surrogates for an epiretinal membrane (Fig. 3): bandage phantom [20], and inner shell membrane (ISM) of 12-day old chicken embryo [21].
Figure 2.

Setup for membrane peeling experiments using (a) the Steady-Hand Robot, and (b) Micron.
Figure 3.
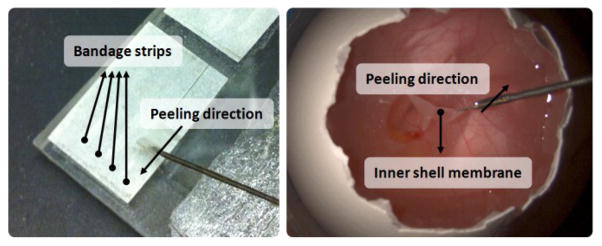
Membrane peeling procedure using bandage phantom (left) and inner shell membrane in chicken embryo (right).
Bandage Phantom
This phantom has 2 mm wide strips that are produced by slicing sticky tabs from 19 mm Clear Bandages (RiteAid brand). At the end of each strip, there is a flap for holding/grasping. Each strip can be used several times without significant change in the required force.
ISM of Chicken Embryo
The eggshell is removed gently to access the ISM chicken embryo. Under the thin ISM layer, there is chorioallantoic membrane (CAM), which serves as a good surrogate for retina. Peeling the ISM off without breaking the CAM is similar to the challenge involved in the epiretinal membrane peeling surgery.
B. Procedure
In this study, we tested the performance of a single novice non-surgeon researcher for different cases on two different phantom types. The studied cases are summarized in Table I.
TABLE I.
Membrane Peeling Performance Test Cases
| Phantom | Tool | Case | Tremor Suppression | Auditory Feedback |
|---|---|---|---|---|
| Bandage Phantom | Hook | (1) Freehand | No | No |
| (2) Only with AF | No | Yes | ||
| (3) Micron aided with AF | Yes | Yes | ||
| Forceps | (4) Freehand | No | No | |
| (5) Only with AF | No | Yes | ||
| (6) Steady-Hand Robot aided with AF | Yes | Yes | ||
| Embryo ISM of Chicken | Hook | (7) Only with AF | No | Yes |
| (8) Micron aided with AF | Yes | Yes | ||
| Forceps | (9) Only with AF | No | Yes | |
| (10) Steady-Hand Robot aided with AF | Yes | Yes |
Procedure on Bandage Phantom
The subject was asked to peel a 10 mm section of the bandage strip steadily and without stopping while holding the tool perpendicular to the peeling direction so that the task is completed with pure transverse loading on the tool tip. 3 cases were studied and 10 trials per case were conducted in random order.
Procedure on ISM of Chicken Embryo
The subject was asked to peel off the ISM without breaking into the CAM by following a linear trajectory. The tool was again held perpendicular to the peeling direction to minimize axial forces. 2 cases were studied and 2 tests were done per case. A new embryo was used for each trial and it is assumed that there is no significant difference between embryos.
For each case, an extensive training period (~3 hrs) was allowed before data collection. The challenge in all cases was to complete the peeling task by moving the tool with a uniform velocity (~0.5 mm/s) and by applying forces below the danger threshold (~7.5 mN). Robot assisted and freehand tests were done in random order. Only in some cases, the user was provided with auditory feedback whereas force sensing was used only for data acquisition purposes in the rest. During the experiments, we recorded the tool tip force, position, speed and video. Based on the video timestamp, we identified the delaminating periods. The forces measured during these delaminating periods form the basis of our performance evaluation.
IV. Results
A. Membrane Peeling on Bandage Phantom
Measured forces on bandage phantom are shown for all trials in Fig. 4. Consistent characteristics were visible among the trials in each case. In free hand trials, highly oscillatory forces exceeding the safety threshold were observed. When the user was supplied with force information through auditory feedback, some of these forces could be reduced below the safety limit. In this case, although the user clearly knew the applied force, there were challenges in controlling the tool motion precisely due to physiological hand tremor. The assistance of either Micron or the Steady-Hand Robot was able to eliminate this problem. Compensating for the unintentional high frequency motion, tool control of the user was greatly improved. In this case, knowing the force level through auditory feedback, the user was able to complete the task very precisely such that in the delaminating period, almost all of the forces were kept below 7.5 mN free of high frequency vibrations.
Figure 4.

Measured peeling forces (blue) using bandage phantom for all trials (10 trials/case). Auditory feedback helps in keeping forces below the safety threshold (red horizontal line). Robotic assistance helps in eliminating oscillations. Additional effort and longer duration in grasping the bandage while using micro-forceps with the Steady-Hand Robot due to additional system inertia.
Despite the improvement in tool control while peeling, difficulty in initial grasping was observed at the beginning of each trial when micro-forceps were used with the Steady-Hand Robot. The additional inertia introduced on the user hand makes certain maneuvers more challenging for a novice user. This extra effort can clearly be seen from the first 10 seconds of case 6 in Fig. 4. On the other hand, being a hand-held tool, Micron has better dexterity but a more limited workspace. The user can still perform similar maneuvers as a manual tool, but while paying attention to stay within the boundaries of the workspace. For this reason, the manipulation problem in case 6 does not exist in case 3.
The hand tremor reduction characteristics for each device can better be seen when the measured forces are analyzed in frequency domain as shown in Fig. 5. Accordingly, presence of auditory force feedback does not change the frequency distribution of forces very much for either the hook or the micro-forceps. However, utilizing robotic assistance has great impact on the characteristics. The bandwidth of human eye-hand feedback is usually from 0.5 Hz to 2 Hz [22]. Thus, the region below 0.5 Hz in Fig. 5 represents controlled actions, whereas frequencies above 2 Hz indicate the unintentional motion of the user. The postural hand tremor frequency in normal humans is at about 8–10 Hz [22]. The prominence of a peak at 10 Hz in all freehand trials is primarily due to this reason. When Micron is used, this peak is eliminated and the high frequency components (2–15 Hz) are overall reduced by 60–80%. The reduction zone for the Steady-Hand Robot is slightly broader with a similar reduction ratio as compared to Micron.
Figure 5.

Frequency analysis on forces applied in all trials on bandage phantom. 60–80% reduction in 2–15 Hz oscillations by using Micron (upper), Steady-Hand Robot (lower).
B. Membrane Peeling on ISM of Chicken Embryo
Having proven the benefits of force sensing capabilities in the first part of our experiments, we did all of the trials in this section with auditory feedback. The aim was to account for heterogeneous tissue properties in our comparison between Micron and the Steady-Hand Robot by using a more realistic biological phantom. Consequently, we observed significantly different characteristics for each device as compared with the bandage phantom.
The measured forces for all trials are shown in Fig. 6. Since all tests were done under auditory feedback, most of the measured forces were remained successfully below the safety threshold. However as opposed to our bandage phantom trials, the user had to grasp the membrane and peel it several times to complete the task, which can be attributed to two main reasons: First, it is not possible to remove the whole ISM in a single linear peel. Second, the ISM is more slippery and deformable than the bandage phantom, which makes it hard to hold firmly. This fact is most apparent while using hook in cases 7 and 8 due to inability to grasp ISM with this type of tool. Micro-forceps have performed better in this respect with only 1–3 delaminating periods in cases 9 and 10.
Figure 6.
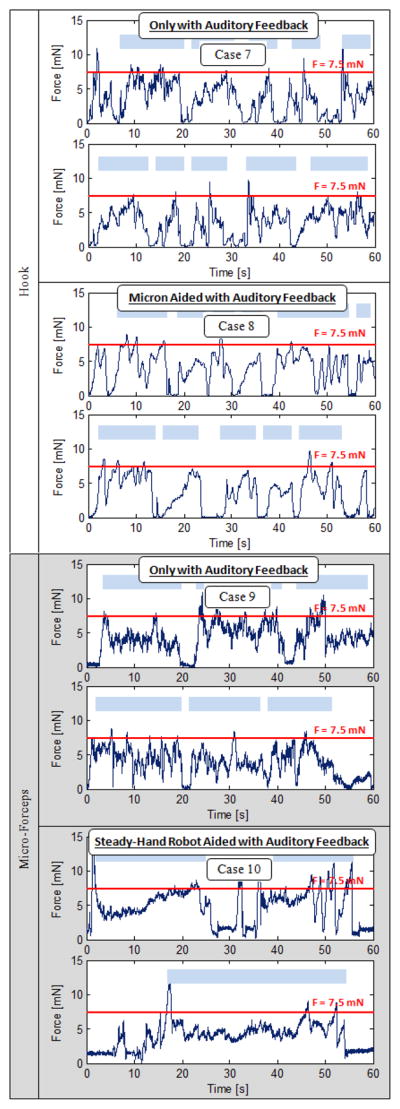
Measured peeling forces (dark blue) using ISM of chicken embryo for all trias (2 trials/case). Shorter multiple peeling periods (light blue rectangles) as opposed to bandage phantom trials.
Frequency analysis of measured forces on ISM is shown in Fig. 7. In all results, an increase in low frequency oscillations as compared to bandage phantom results is prominent. This is an expected result of using biological phantom with non-uniform tissue properties. By using a hook manually in case 7, high frequency oscillations were observed in Fig. 6. However, 10 Hz peak corresponding to the physiological hand tremor is not visible for this case in Fig. 7. This is mainly due to poor grasping and slippage of the tissue, and resulting disturbance on the force measurement. But still 40–50% reduction in high frequency oscillations was recorded with Micron assistance. Using micro-forceps, a behavior that is similar to the results on bandage phantom is obtained. 10 Hz peak is clearly visible in manual use of micro-forceps. Utilizing Steady-Hand Robot assistance with this tool has decreased 2–15 Hz oscillations by 50–60%.
Figure 7.

Frequency analysis on forces applied in all trials on ISM of chicken embryo. Reduction in 2–15 Hz oscillations: 40–50% by Micron (upper), 50–60% by the Steady-Hand Robot (lower). 10 Hz peak corresponding to physiological hand tremor is not visible while using hook (upper) due to poor tissue grasping.
V. DISCUSSION
The acquired force data for each case was analyzed based on average values of five main criteria, which are summarized in Table II. On the bandage phantom, using either Micron or the Steady-Hand Robot have provided similar improvements, which are significant in terms of reducing the standard deviation of forces (by 63% with Micron and 60% with the Steady-Hand Robot) and the danger zone percentage (4.97% with Micron and 4.26% with the Steady-Hand Robot). Hence, a more consistent and safe operation was provided through the assistance of either robotic system.
TABLE II.
Evaluation Of Cases Based On Average Of All Trials
| Phantom | Tool | Case | Max. Force [mN] | Mean Force [mN] | Standard Deviation [mN] | Duration in Danger Zone [sec] | Danger Zone Percentage |
|---|---|---|---|---|---|---|---|
| Bandage Phantom | Hook | (1) Freehand | 14.81 | 7.63 | 1.68 | 9.30 | 46.51% |
| (2) Only with AF | 9.91 | 6.46 | 0.98 | 2.94 | 14.71% | ||
| (3) Micron aided with AF | 8.65 | 6.38 | 0.62 | 0.99 | 4.97% | ||
| Forceps | (4) Freehand | 12.11 | 6.85 | 1.59 | 6.60 | 33.02% | |
| (5) Only with AF | 8.96 | 6.20 | 0.79 | 1.25 | 6.24% | ||
| (6) Steady-Hand Robot aided with AF | 8.20 | 6.26 | .64 | 0.85 | 4.26% | ||
| ISM of Chciken Embryo | Hook | (7) Only with AF | 8.27 | 4.55 | 1.56 | 0.32 | 0.74% |
| (8) Micron aided with AF | 7.58 | 4.81 | 1.35 | 0.44 | 0.54% | ||
| Forceps | (9) Only with AF | 9.05 | 4.93 | 1.46 | 1.26 | 2.11% | |
| (10) Steady-Hand Robot aided with AF | 7.96 | 4.87 | 1.33 | 1.11 | 1.85% |
In contrast to the consistent peeling environment provided by the bandage phantom, the ISM of chicken embryo exhibited non-uniform tissue properties. It was more challenging to manipulate the ISM due to these variations and its slippery deformable structure. For this reason, the success in decreasing the standard deviation was drastically reduced on ISM (by 13% with Micron and 8.9% with the Steady-Hand Robot). The danger zone percentage was already low in all trials as compared to the previous cases. Thus, the robotic assistance on ISM did not provide much benefit in terms of keeping the forces below the safety threshold. This could be either a difference between the two types of phantoms, or a matter of the user’s learning curve since ISM tests were done after completion of the bandage experiments which need to be addressed in future tests.
VI. Conclusion
This paper has reported a performance comparison between two distinct robotic systems: Micron and the Steady-Hand Robot. Both of these systems were developed for assisting vitreoretinal surgery, but they differ in numerous important aspects such as size, cost, control strategy, learning curve and operational performance. In this study, we demonstrated the performance of a single user for each system in membrane peeling. By measuring the peeling forces, we analyzed the behavior on two types of phantoms (bandage phantom and ISM of chicken embryo) in terms of applied forces, physiological hand-tremor reduction characteristics, and consistency. While both systems have provided similar tremor reduction and consistency improvement on bandage phantom, Micron performance on ISM was challenged by the unavailability of forceps tool for this system. Using micro-forceps with the Steady-Hand Robot has revealed superior performance by holding the tissue firmly and manipulating it much easily.
The results of our single-user pilot study in this paper are encouraging and provide the basis for a multi-user study in order to assess the influence of various system parameters, and inspect the existence of optimal values for different tasks. Upon optimal tuning of each system, our future work aims at performance analyses on both surgeons and non-surgeons with extensive comparison criteria including ergonomics, feasibility, workflow, and the learning curves.
Acknowledgments
The authors thank Prof. Cameron Riviere and his team at Carnegie Mellon University for providing the Micron robot.
Footnotes
Research supported in part by the National Institutes of Health under R01 EB007969, and R01 EB000526, and in part by Johns Hopkins internal funds.
Contributor Information
Berk Gonenc, Email: bgonenc1,rht@jhu.edu, CISST ERC at Johns Hopkins University, Baltimore, MD 21218 USA.
James Handa, Email: jthanda@jhmi.edu, Wilmer Eye Institute at The Johns Hopkins School of Medicine, Baltimore, MD 21287 USA.
Peter Gehlbach, Email: pgelbach@jhmi.edu, Wilmer Eye Institute at The Johns Hopkins School of Medicine, Baltimore, MD 21287 USA.
Russell H. Taylor, CISST ERC at Johns Hopkins University, Baltimore, MD 21218 USA
Iulian Iordachita, Email: iordachita@jhu.edu, CISST ERC at Johns Hopkins University, Baltimore, MD 21218 USA.
References
- 1.Wilkins JR, Puliafito CA, Hee MR, Duker JS, Reichel E, Coker JG, Schuman JS, Swanson EA, Fujimoto JG. Characterization of epiretinal membranes using optical coherence tomography. Ophthalmology. 1996 Dec;103(12):2142–2151. doi: 10.1016/s0161-6420(96)30377-1. [DOI] [PubMed] [Google Scholar]
- 2.Sjaarda RN, Glaser BM, Thompson JT, Murphy RP, Hanham A. Distribution of iatrogenic retinal breaks in macular hole surgery. Ophthalmology. 1995 Sep;102(9):1387–1392. doi: 10.1016/s0161-6420(95)30859-7. [DOI] [PubMed] [Google Scholar]
- 3.Carter JB, Michels RG, Glaser BM, DeBustros S. Iatrogenic retinal breaks complicating pars plana vitrectomy. Ophthalmology. 1990 Jul;97(7):848–853. doi: 10.1016/s0161-6420(90)32492-2. [DOI] [PubMed] [Google Scholar]
- 4.Grigorian RA, Castellarin A, Fegan R, Seery C, Del Priore LV, von Hagen S, Zarbin MA. Epiretinal membrane removal in diabetic eyes: Comparison of viscodissection with conventional methods of membrane peeling. Br J Ophthalmology. 2003 Jun;87:737–741. doi: 10.1136/bjo.87.6.737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Nakata K, Ohji M, Ikuno Y, Kusaka S, Gomi F, Tano Y. Sub-retinal hemorrhage during internal limiting membrane peeling for a macular hole. Graefes Arch Clin Exp Ophthalmol. 2003 Jul;241:582–584. doi: 10.1007/s00417-003-0676-y. [DOI] [PubMed] [Google Scholar]
- 6.Das H, Zak H, Johnson J, Crouch J, Frambach D. Evaluation of a telerobotic system to assist surgeons in microsurgery. Comput Aided Surg. 1999;4(1):15–25. doi: 10.1002/(SICI)1097-0150(1999)4:1<15::AID-IGS2>3.0.CO;2-0. [DOI] [PubMed] [Google Scholar]
- 7.Schenker PS, Barlow EC, Boswell CD, Das H, Lee S, Ohm TR, Paljug ED, Rodriguez G, Charles ST. Development of a telemanipulator for dexterity enhanced microsurgery. Proc. 2nd Int Symp Med Rob Comput Asst Surg; 1995. pp. 81–88. [Google Scholar]
- 8.Hunter IW, Doukoglou TD, Lafontaine SR, Charette PG, Jones LA, Sagar MA, Mallinson GD, Hunter PJ. A teleoperated microsurgical robot and associated virtual environment for eye surgery. Presence. 1993;2(4):265–280. [Google Scholar]
- 9.Hunter IW, Jones LA, Sagar MA, Lafontaine SR, Hunter PJ. Opthalmic microsurgical robot and associated virtual environment. Comput Biol Med. 1995 Mar;25(2):173–182. doi: 10.1016/0010-4825(94)00042-o. [DOI] [PubMed] [Google Scholar]
- 10.Ueta T, Yamaguchi Y, Shirakawa Y, Nakano T, Ideta R, Noda Y, Morita A, Mochizuki R, Sugita N, Mituishi M, Tamaki Y. Robot-assisted vitreoretinal surgery: Development of a prototype and feasibility studies in an animal model. Ophthalmology. 2009 Aug;116(8):1538–1543. doi: 10.1016/j.ophtha.2009.03.001. [DOI] [PubMed] [Google Scholar]
- 11.Das H, Zak H, Johnson J, Crouch J, Frambach D. Evaluation of a telerobotic system to assist surgeons in microsurgery. Comput Aided Surg. 1999;4(1):15–25. doi: 10.1002/(SICI)1097-0150(1999)4:1<15::AID-IGS2>3.0.CO;2-0. [DOI] [PubMed] [Google Scholar]
- 12.Jensen PS, Grace KW, Attariwala R, Colgate JE, Glucksberg MR. Toward robot-assisted vascular microsurgery in the retina. Graefes Arch Clin Exp Ophthalmol. 1997 Nov;235(11):696–701. doi: 10.1007/BF01880668. [DOI] [PubMed] [Google Scholar]
- 13.Mulgaonkar AP, Hubschman JP, Bourges JL, Jordan BL, Cham C, Wilson JT, Tsao TC, Culjat MO. A prototype surgical manipulator for robotic intraocular micro surgery. Stud Health Technol Inform. 2009;142:215–217. [PubMed] [Google Scholar]
- 14.Uneri A, Balicki MA, Handa J, Gehlbach P, Taylor RH, Iordachita I. New steady-hand Eye Robot with micro-force sensing for vitreoretinal surgery. Proc. 3rd IEEE RAS EMBS Int Conf Biomed Robot Biomechatron (BioRob); 2010. pp. 814–819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Taylor R, Jensen P, Whitcomb L, Barnes A, Kumar R, Stoianovici D, Gupta P, Wang Z, deJuan E, Kavoussi L. A steady-hand robotic system for microsurgical augmentation. Proc. MICCAI; 1999. pp. 1031–1041. [Google Scholar]
- 16.Mitchell B, Koo J, Iordachita M, Kazanzides P, Kapoor A, Handa J, Hager G, Taylor R. Development and application of a new steady-hand manipulator for retinal surgery. Proc. IEEE ICRA; 2007. pp. 623–629. [Google Scholar]
- 17.MacLachlan RA, Becker BC, Cuevas Tabars J, Podnar GW, Lobes LA, Riviere CN. Micron: an actively stabilized handheld tool for microsurgery. IEEE Trans Robot. 2012 Feb;28(1):195–212. doi: 10.1109/TRO.2011.2169634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sun Z, Balicki M, Kang J, Handa J, Taylor R, Iordachita I. Development and preliminary data of novel integrated optical micro-force sensing tools for retinal microsurgery. IEEE Int. Conf. on Robotics and Automation ICRA’09; 2009. pp. 1897–1902. [Google Scholar]
- 19.Gonenc B, Balicki MA, Handa J, Gehlbach P, Riviere CN, Taylor RH, Iordachita I. Evaluation of a Micro-Force Sensing Handheld Robot for Vitreoretinal Surgery. Proc. IROS 2012; Vilamoura, Algarve, Portugal. October 7–12, 2012; pp. 4125–4130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Balicki M, Uneri A, Iordachita I, Handa J, Gehlbach P, Taylor R. Micro-force sensing in robot assisted membrane peeling for vitreoretinal surgery. In: Jiang T, Navab N, Pluim J, Viergever M, editors. Medical Image Computing and Computer-Assisted Intervention (MICCAI 2010) vol. 6363 of Lecture Notes in Computer Science. Springer; Berlin/Heidelberg: 2010. pp. 303–310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.He X, Balicki MA, Kang JU, Gehlbach PL, Handa JT, Taylor RH, Iordachita II. Force sensing micro-forceps with integrated fiber bragg grating for vitreoretinal surgery. Proceedings of SPIE. 2012 Feb;8218:82180W–82180W–7. [Google Scholar]
- 22.Stiles RN. Mechanical and neural feedback factors in postural hand tremor of normal subjects. J Neurophysiol. 1980 Jul;44:40–59. doi: 10.1152/jn.1980.44.1.40. [DOI] [PubMed] [Google Scholar]
- 23.Kuru I, Gonenc B, Balicki M, Handa J, Gehlbach P, Taylor RH, Iordachita I. Force Sensing Micro-Forceps for Robot Assisted Retinal Surgery. Proc. EMBC 2012; San Diego, CA. Aug 28–Sep 1, 2012; pp. 1401–1404. [DOI] [PMC free article] [PubMed] [Google Scholar]