

Abstract
Purpose
This study was performed to investigate the effect of image enhancement of periapical radiographs according to the diagnostic task.
Materials and Methods
Eighty digital intraoral radiographs were obtained from patients and classified into four groups according to the diagnostic tasks of dental caries, periodontal diseases, periapical lesions, and endodontic files. All images were enhanced differently by using five processing techniques. Three radiologists blindly compared the subjective image quality of the original images and the processed images using a 5-point scale.
Results
There were significant differences between the image quality of the processed images and that of the original images (P<0.01) in all the diagnostic task groups. Processing techniques showed significantly different efficacy according to the diagnostic task (P<0.01).
Conclusion
Image enhancement affects the image quality differently depending on the diagnostic task. And the use of optimal parameters is important for each diagnostic task.
Keywords: Image Enhancement; Radiography, Dental, Digital
Introduction
Since the development of digital radiography, many changes have taken place in the field of diagnostic imaging, and digital radiography has become widely accepted in dental radiography. Digital radiography has several advantages over film radiography. To begin with, digital radiography has a wider dynamic range, and therefore, the radiation exposure to the patient can be reduced. The elimination of chemical processing and processing errors saves time and reduces the radiation exposure. In addition, images can be stored permanently without any degradation of image quality.
One of the important advantages of digital radiography is the easy access to image processing. Image processing can reduce retakes caused by processing or exposure errors, because the contrast and density of digital images can be manipulated by image processing.1 Because of these benefits, digital radiography has replaced film radiography in dental practice.
In conventional film radiography, the adjustment of acquired images is impossible. In contrast, after obtaining the raw data, digital images can be manipulated by various techniques and viewed on the. There are many processing techniques that can enhance digital images and make them more suitable for diagnosis, such as contrast optimization, noise reduction, and artifact reduction.2 Depending on the application of image processing techniques, various digital images with different image characteristics can be obtained. The enhancement of image contrast through these various processes can improve the diagnostic performance and subjective image quality.3,4,5,6 However, an increase in the image contrast does not always lead to a better outcome.7,8,9,10 For example, increased contrast between enamel and dentin can help to detect dental caries, but excessive contrast will result in the false positive diagnosis of dental caries or create an unfavorable image for the diagnosis of periodontal diseases when the density of images increases too much to identify the outline of the enamel or the alveolar bone level. Similarly, important anatomic structures for the diagnosis differ according to the diagnostic task; therefore, the optimal contrast of an image may differ according to the diagnostic task.
Most of the studies conducted thus far have focused on the effect of image enhancement of periapical radiographs with a single diagnostic task of mainly proximal caries or periapical lesions.3,4,5,6,7,8,9 However, the diagnostic task of a periapical radiograph may affect the results of a study; therefore, the study should be conducted with a classification of periapical radiographs according to the diagnostic task. The aim of this study was to confirm the different outcomes of the image enhancement of periapical radiographs according to the diagnostic task and to identify a suitable image enhancement technique for each diagnostic task.
Materials and Methods
Clinical radiographs
The images were obtained from patients who had to undergo periapical radiography of the molar or premolar areas. All periapical radiographs were taken by using a paralleling technique with the use of an extension cone paralleling (XCP) device. A complementary metal-oxide semi-conductor (CMOS) system (EZ Sensor P, Vatech, Hwaseong, Korea) was used. The pixel size of the receptor was 20 µm, and the receptor had a theoretical resolution of 25 lp/mm.
Poor-quality images exposure errors such as cone-cut, over or underexposure, and overlapping were excluded. The images were carefully reviewed, and the presence of lesions was identified under the consensus of three radiologists. The images with lesions were selected and classified into four groups, namely dental caries, periodontal diseases, periapical lesions, and endodontic files according to the diagnostic task. A total of 80 digital periapical radiographs were collected, that is, 20 images for each diagnostic task.
Image enhancement
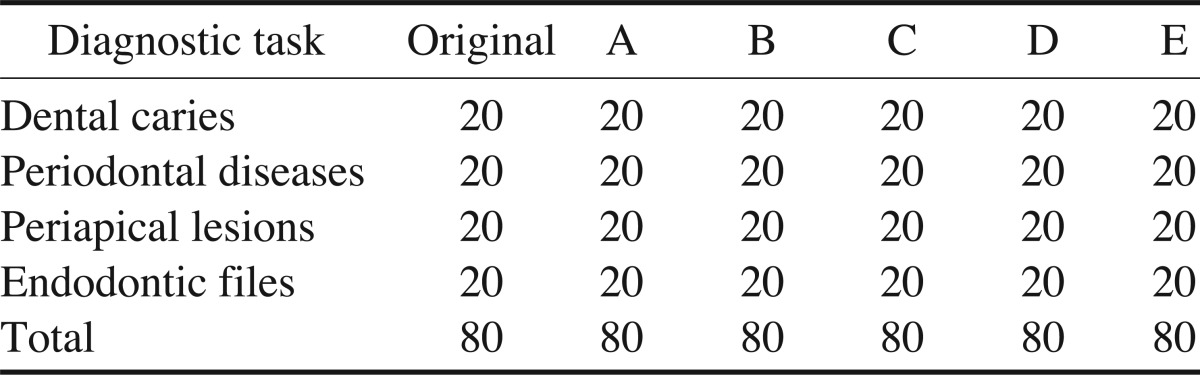
Raw data of the original images were processed as illustrated in Figure 1. To start with, the dynamic range of the images was controlled by using a histogram to maintain the range of the signal area constantly, in order to reduce the differences between images caused by the differences in dose or attenuation by patients. Secondly, the contrast-limited adaptive histogram equalization (CLAHE) technique was used to enhance the local contrast of the images. In this stage, five sets of processing techniques were developed with different local contrast levels to identify the suitable enhancement technique according to the diagnostic task (Fig. 2). Five processing techniques were distinguished as follows: technique A with low contrast, technique B with moderate contrast, technique C with slightly high contrast, technique D with high contrast, and technique E with very high contrast. Finally, a modified unsharp-masking technique was used to enhance the sharpness of the images. In short, 80 original images were enhanced by the five different processing techniques, and a total of 400 images divided into the 5 sets were obtained (Table 1).
Fig. 1.

Stages of image enhancement.
Fig. 2.

Original and processed images. A. image enhanced by processing technique A. B. image enhanced by processing technique B. C. image enhanced by processing technique C. D. image enhanced by processing technique D. E. image enhanced by processing technique E. F. original image.
Table 1.
Classification and number of images
Evaluation of the subjective image quality
Three radiologists participated in the evaluation as observers. Images were displayed on two sets of high-resolution mono-display monitors (IF2105M, Wide Corp., Yongin, Korea). The room was dimly lit, and the sunlight was blocked. Ahead of the evaluation, the observers were instructed about the anatomic structures of images in order to focus on the diagnostic tasks. The anatomic structures were enamel, dentin, dentinoenamel junction, and pulp chamber for the diagnostic task of dental caries; alveolar crest, lamina dura, and trabecular bone for the diagnostic task of periodontal diseases; and lamina dura, periodontal ligament space, trabecular bone, root apex, and tip of endodontic file for the diagnostic task of periapical lesions and endodontic files.
An original and its processed image were displayed on each monitor in a randomized order, and the observers were not informed about the application or kind of enhancement of the images. The observers were not allowed to manipulate the images manually during their evaluation. The observers comparatively evaluated the subjective image quality on a confidence scale of 1-5: (1) The left image has a better image quality than the right one for detecting dental caries. (2) The left image seems to have a better image quality than the right one for detecting dental caries. (3) Both images have no differences in image quality with respect to the detection of dental caries. (4) The right image seems to have a better image quality than the left one for detecting dental caries. (5) The right image has a better image quality than the left one for detecting dental caries. As there were 5 different processing techniques and 4 classifications of diagnostic tasks, a total of 20 sets and 400 pairs of images were evaluated at a time, and the evaluation was repeated 2 times with an interval of a week.
Statistical analysis
The ratings of the processed images of each observer were averaged and then analyzed by using one sample t-test, to identify the differences from confidence scale of 3, which indicates that both images have no differences in image quality. The differences in the ratings of each processing technique were evaluated by using the one-way analysis of variance test(ANOVA) and a post-hoc Scheffe's post comparison by using IBM SPSS Statistics version 21 (IBM Corp., Somers, NY, USA). The statistical significance level of P<0.01 was used.
Results
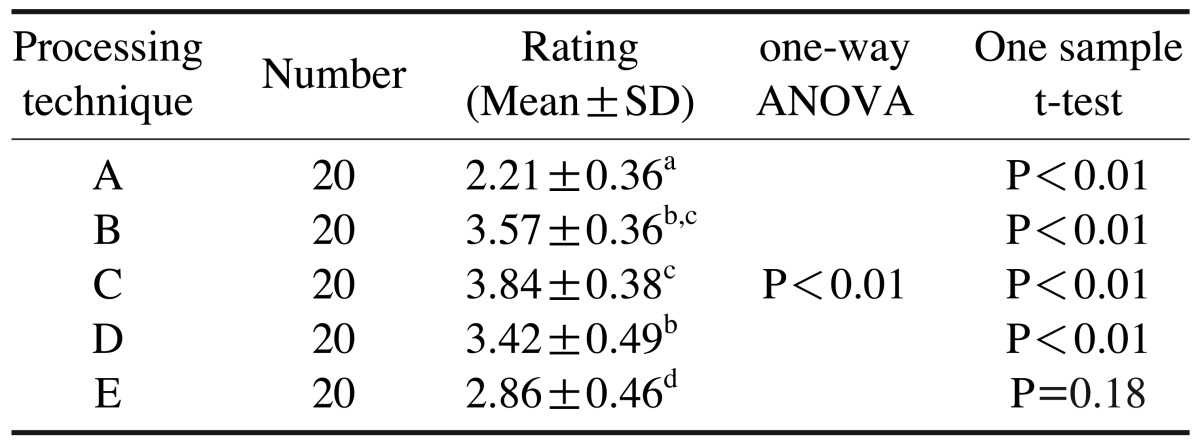
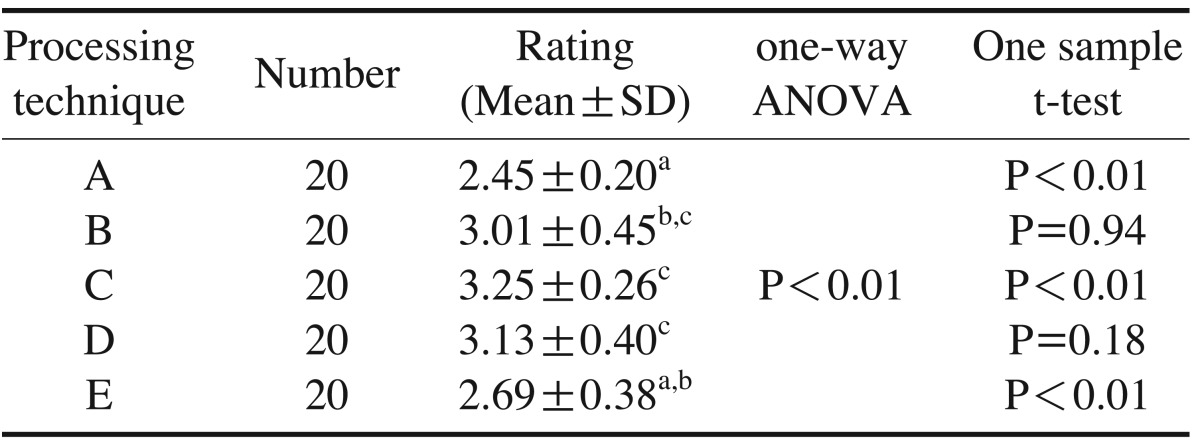
The rating scores of images enhanced by processing technique B showed the highest score in the diagnostic task of dental caries, and the differences between processing techniques were statistically significant. Processing technique B was the only significant method to enhance image quality on the diagnostic task of dental caries (Table 2). The ratings of all image groups had significantly lower scores than the original images on the diagnostic task of periodontal diseases (Table 3) The rating scores of enhanced images by processing techniques B, C, and D recorded significantly higher scores than the original images in the diagnostic task of periapical lesions. Processing technique A was the only method that showed a lower score than the original images (Table 4). The rating score of mages enhanced by processing technique C was significantly higher than that of the original images in the diagnostic task of endodontic files. Processing technique C was the only significant method for the enhancement of image quality in the diagnostic task of endodontic files (Table 5).
Table 2.
Descriptive statistics of the rating scores of enhanced images by processing techniques on the diagnostic task of dental caries
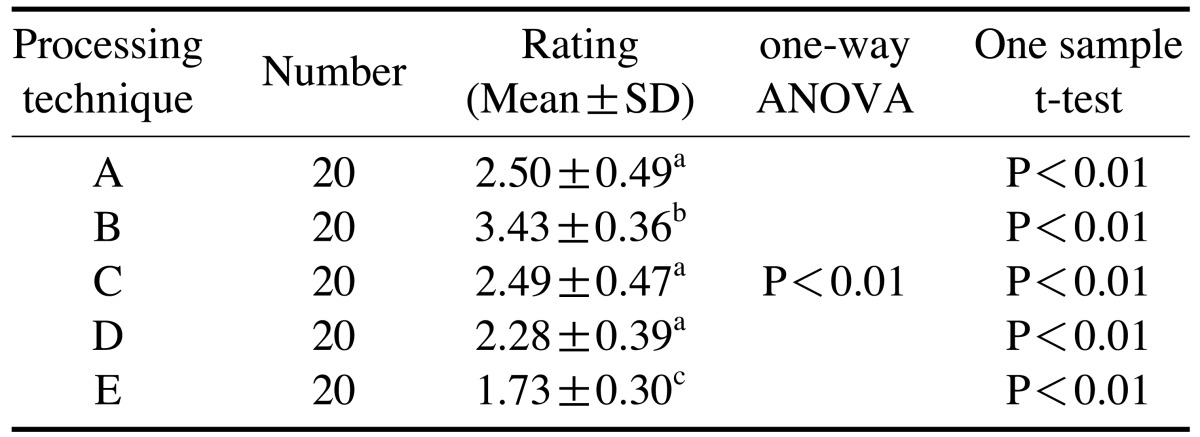
a,b,cThe different characters shows statistically significant deference between groups by Scheffe's post comparison. SD: standard deviation
Table 3.
Descriptive statistics of the rating scores of enhanced images by processing techniques on the diagnostic task of periodontal diseases
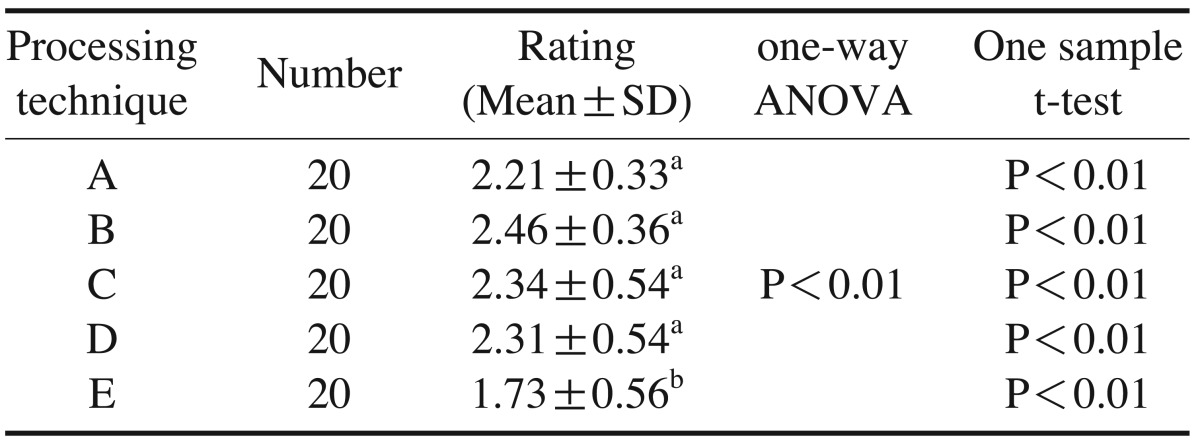
a,bThe different characters shows statistically significant deference between groups by Scheffe's post comparison. SD: standard deviation
Table 4.
Descriptive statistics of the rating scores of enhanced images by processing techniques on the diagnostic task of periapical lesions
a,b,c,dThe different characters shows statistically significant deference between groups by Scheffe's post comparison. SD: standard deviation
Table 5.
Descriptive statistics of the rating scores of enhanced images by processing techniques on the diagnostic task of endodontic files
a,b,cThe different characters shows statistically significant deference between groups by Scheffe's post comparison. SD: standard deviation
Discussion
As we hypothesized, processing techniques affected image quality differently according to the diagnostic task, and we found effective parameters to improve the local contrast for dental caries, periapical lesions, and endodontic files.
To begin with dental caries, there is a controversy about the effectiveness of image enhancement on the detection of dental caries and there are contradictory reports about it. Some researchers have reported positive effects, and others have reported negative or no effects of image enhancement on the detection of dental caries.4,5,6,7,10,11 In this study, we revealed that image enhancement certainly improves the subjective image quality, allowing the clinician to identify dental caries more readily. However, only image processing technique B showed a good result, and the other four techniques recorded lower ratings due to improper local contrast, although all images were processed by the same technical procedure. This result indicates that the processing parameters are as important as the use of the processing technique itself, and this corresponds with the result of an earlier study.4 The results of the other diagnostic tasks also suggested the importance of the processing parameters as there were significant differences between processing techniques in the same diagnostic task.
In the diagnostic task of periodontal diseases, all processing techniques could not improve the image quality, and this result is in agreement with the results of previous studies.12,13,14 However, we cannot conclude that image enhancement is not efficient in the diagnosis of periodontal diseases as the abovementioned results could just be because we could not find the optimal parameters. In addition, we excluded poor-quality images and there may be no room for improvement of good-quality images.
In the diagnostic tasks of periapical lesions and endodontic files, processing technique C recorded the highest ratings and proved to be an effective method for enhancing the image quality of periapical radiographs. This result is consistent with that of a previous study that reported the usefulness of enhancement in the size measurement of periapical lesions on periapical radiographs.3
These results suggest that there are optimal ranges of contrast according to the diagnostic task, and this is in accordance with the results of a previous study.15 We speculated that the optimal ranges of local contrast could be narrow for dental caries and endodontic files, and wide for periapical lesions. Further studies will be required to reveal the objective parameters compatible with multiple intraoral X-ray systems.
Although the image enhancement used in this study increases subjective image quality, this study does not prove that image enhancement can improve the diagnostic performance because only images with specific lesions were included and we do not have the gold standard of an invivo study with clinical radiographs. However, it known that image quality is related to observer performance.3,6,16
In conclusion, image enhancement affects image quality differently depending on the diagnostic task, and the use of optimal parameters is important for each diagnostic task.
Footnotes
This research was supported by a grant from Vatech company group 2012.
References
- 1.Körner M, Weber CH, Wirth S, Pfeifer KJ, Reiser MF, Treitl M. Advances in digital radiography: physical principles and system overview. Radiographics. 2007;27:675–686. doi: 10.1148/rg.273065075. [DOI] [PubMed] [Google Scholar]
- 2.Wenzel A. Current trends in radiographic caries imaging. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;80:527–539. doi: 10.1016/s1079-2104(05)80152-0. [DOI] [PubMed] [Google Scholar]
- 3.Farman AG, Avant SL, Scarfe WC, Farman TT, Green DB. In vivo comparison of Visualix-2 and Ektaspeed Plus in the assessment of periradicular lesion dimensions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85:203–209. doi: 10.1016/s1079-2104(98)90427-9. [DOI] [PubMed] [Google Scholar]
- 4.Sund T, Møystad A. Sliding window adaptive histogram equalization of intraoral radiographs: effect on image quality. Dentomaxillofac Radiol. 2006;35:133–138. doi: 10.1259/dmfr/21936923. [DOI] [PubMed] [Google Scholar]
- 5.Møystad A, Svanaes DB, Risnes S, Larheim TA, Gröndahl HG. Detection of approximal caries with a storage phosphor system. A comparison of enhanced digital images with dental X-ray film. Dentomaxillofac Radiol. 1996;25:202–206. doi: 10.1259/dmfr.25.4.9084274. [DOI] [PubMed] [Google Scholar]
- 6.Li G, Yoshiura K, Welander U, Shi XQ, McDavid WD. Detection of approximal caries in digital radiographs before and after correction for attenuation and visual response. An in vitro study. Dentomaxillofac Radiol. 2002;31:113–116. doi: 10.1038/sj/dmfr/4600675. [DOI] [PubMed] [Google Scholar]
- 7.Shi XQ, Li G. Detection accuracy of approximal caries by black-and-white and color-coded digital radiographs. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107:433–436. doi: 10.1016/j.tripleo.2008.07.008. [DOI] [PubMed] [Google Scholar]
- 8.Scarfe WC, Czerniejewski VJ, Farman AG, Avant SL, Molteni R. In vivo accuracy and reliability of color-coded image enhancements for the assessment of periradicular lesion dimensions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:603–611. doi: 10.1016/s1079-2104(99)70093-4. [DOI] [PubMed] [Google Scholar]
- 9.Kullendorff B, Petersson K, Rohlin M. Direct digital radiography for the detection of periapical bone lesions: a clinical study. Endod Dent Traumatol. 1997;13:183–189. doi: 10.1111/j.1600-9657.1997.tb00036.x. [DOI] [PubMed] [Google Scholar]
- 10.Dove SB, McDavid WD. A comparison of conventional intraoral radiography and computer imaging techniques for the detection of proximal surface dental caries. Dentomaxillofac Radiol. 1992;21:127–134. doi: 10.1259/dmfr.21.3.1397467. [DOI] [PubMed] [Google Scholar]
- 11.Tyndall DA, Ludlow JB, Platin E, Nair M. A comparison of Kodak Ektaspeed Plus film and the Siemens Sidexis digital imaging system for caries detection using receiver operating characteristic analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85:113–118. doi: 10.1016/s1079-2104(98)90408-5. [DOI] [PubMed] [Google Scholar]
- 12.Alves WE, Ono E, Tanaka JL, Medici Filho TE, de Moraes LC, de Moraes ME, et al. Influence of image filters on the reproducibility measurements of alveolar bone loss. J Appl Oral Sci. 2006;14:415–420. doi: 10.1590/S1678-77572006000600006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wolf B, von Bethlenfalvy E, Hassfeld S, Staehle HJ, Eickholz P. Reliability of assessing interproximal bone loss by digital radiography: intrabony defects. J Clin Periodontol. 2001;28:869–878. doi: 10.1034/j.1600-051x.2001.028009869.x. [DOI] [PubMed] [Google Scholar]
- 14.Li G, Engström PE, Welander U. Measurement accuracy of marginal bone level in digital radiographs with and without color coding. Acta Odontol Scand. 2007;65:254–258. doi: 10.1080/00016350701452089. [DOI] [PubMed] [Google Scholar]
- 15.Güneri P, Lomçali G, Boyacioğlu H, Kendir S. The effects of incremental brightness and contrast adjustments on radiographic data: a quantitative study. Dentomaxillofac Radiol. 2005;34:20–27. doi: 10.1259/dmfr/85029529. [DOI] [PubMed] [Google Scholar]
- 16.Yoshiura K. Image quality assessment of digital intraoral radiography - perception to caries diagnosis. Jpn Dent Sci Rev. 2012;48:42–47. [Google Scholar]