

Abstract
Aims: With this study protocol, a research program is introduced. Its overall aim is to prepare the instruments and to conduct the first monitoring of nursing service context factors at three university and two cantonal hospitals in Switzerland prior to the introduction of the reimbursement system based on Diagnosis Related Groups (DRG) and to further develop a theoretical model as well as a methodology for future monitoring following the introduction of DRGs.
Background: DRG was introduced to all acute care hospitals in Switzerland in 2012. In other countries, DRG introduction led to rationing and subsequently to a reduction in nursing care. As result, nursing-sensitive patient outcomes were seriously jeopardised. Switzerland has the opportunity to learn from the consequences experienced by other countries when they introduced DRGs. Their experiences highlight that DRGs influence nursing service context factors such as complexity of nursing care or leadership, which in turn influence nursing-sensitive patient outcomes. For this reason, the monitoring of nursing service context factors needs to be an integral part of the introduction of DRGs. However, most acute care hospitals in Switzerland do not monitor nursing service context data. Nursing managers and hospital executive boards will be in need of this data in the future, in order to distribute resources effectively.
Methods/Design: A mixed methods design in the form of a sequential explanatory strategy was chosen. During the preparation phase, starting in spring 2011, instruments were selected and prepared, and the access to patient and nursing data in the hospitals was organized. Following this, online collection of quantitative data was conducted in fall 2011. In summer 2012, qualitative data was gathered using focus group interviews, which helped to describe the processes in more detail. During 2013 and 2014, an integration process is being conducted involving complementing, comparing and contrasting quantitative and qualitative findings.
Conclusion: The research program will produce baseline data on nursing service context factors in Swiss acute care hospitals prior to DRG introduction as well as a theoretical model and a methodology to support nursing managers and hospital executive boards in distributing resources effectively.
The study was approved by the ethics committees of Basel, Bern, Solothurn and Zürich.
Keywords: DRG, nursing service context factors, nursing monitoring
Zusammenfassung
Ziel: Mit diesem Studienprotokoll wird ein Forschungsprogramm eingeführt. Dessen Ziel ist das Vorbereiten der Instrumente und das Durchführen des ersten Monitorings von Pflegekontextfaktoren an drei Universitäts- und zwei Kantonsspitälern in der Schweiz noch vor Einführung der DRG-basierten Finanzierung, sowie darauf aufbauend das Weiterentwickeln des theoretischen Modells und der dazu gehörenden Methodologie für zukünftige Monitorings nach Einführung der DRGs.
Hintergrund: Die DRG-basierte Finanzierung wurde 2012 in der Schweiz eingeführt. In anderen Ländern führte die Einführung der DRGs zu einer Leistungsbeschränkung und folglich auch zu einer Reduktion der Pflege. Dadurch werden das Erreichen erwünschter pflegesensitiver Patientenergebnisse und die Patientensicherheit gefährdet. Die Schweiz hat die Chance, aus den Erfahrungen anderer Länder im Zusammenhang mit der Einführung der DRG-basierten Finanzierung zu lernen. Deren Erfahrungen unterstreichen den Einfluss der DRGs auf Pflegekontextfaktoren wie die Komplexität der Pflege oder das Führungsverhalten, die ihrerseits pflegesensitive Patientenergebnisse beeinflussen. Vor diesem Hintergrund ist ein begleitendes Monitoring von Pflegekontextfaktoren als integraler Bestandteil der DRG Einführung angemessen. Aktuell werden jedoch in den meisten Schweizer Akutspitälern die Daten solcher Kontextfaktoren nicht regelmässig erhoben. Damit in Zukunft Ressourcen sinnvoll verteilt werden können, sind Spitaldirektionen und Pflegeleitungen jedoch verstärkt auf solche Kennzahlen angewiesen.
Methode/Design: Zur Durchführung dieser Evaluationsstudie wurde ein sequentiell-explanatives Mixed Methods Design gewählt. Während der Vorbereitungsphase, die im Frühjahr 2011 begann, wurden die notwendigen Instrumente ausgewählt und vorbereitet. Zudem wurde der Zugang zu den benötigten Patienten- und Pflegedaten gesichert, welche aus anderen Informationssystemen ins Monitoring übernommen wurden. Im Herbst 2011 konnte die quantitative Datensammlung durchgeführt werden. Daran anschliessend wurden im Sommer 2012 die qualitativen Daten mittels Fokusgruppeninterviews gesammelt, die dabei halfen, die den quantativen Daten zugrunde liegenden Prozesse besser zu verstehen. Dazu wird 2013 und 2014 der Integrationsprozess durchgeführt, mit dem die quantitativen und qualitativen Daten ergänzend, vergleichend und kontrastierend betrachtet werden.
Schlussfolgerung: Die Studie hat bezüglich den interessierenden Pflegekontextfaktoren eine Datenbasis geschaffen, die die Ausgangslage vor der Einführung der DRG-basierten Finanzierung in Schweizer Akutspitälern wiederspiegelt. Zudem konnte ein theoretisches Monitoringmodell mitsamt seiner Methodologie erarbeitet werden, dessen Daten inskünftig Spitaldirektionen und Pflegeleitungen dabei unterstützen kann, Ressourcen effektiv zu verteilt.
Die Studie wurde von den Ethikkommissionen der Kantone Basel, Bern, Solothurn und Zürich geprüft.
Background
In 2012, the DRG-based reimbursement system was introduced to all acute care hospitals in Switzerland. The experiences of other countries showed that, in addition to other factors, the introduction of DRGs decreased patient length of stay (LOS) considerably, due to earlier discharge [1]. It is expected that in Switzerland, as in other countries, there will be an increase in the severity of illness in patients undergoing treatment at acute care hospitals since a great deal of treatment and care will be shifted to the outpatient sector and to long-term care institutions. As a consequence, there will be a burgeoning demand for competent nurses who can manage highly complex patient situations in less time than was available before DRGs were introduced. It is well known that the DRG-payment system does not sufficiently address nursing care, as the latter is subsumed under the umbrella of “treatment costs” [2]. While DRGs are exclusively dependent on medical diagnoses, patients belonging to a single DRG group differ in the nursing care they require due to high variability in support of activities of daily living [2], [3], [4]. As a result, acute care hospitals may not be sufficiently reimbursed for the nursing care provided to their patients.
In other countries, DRG introduction led to rationing, with a decrease in the nursing work force, a decline in the quality of nursing care and a deterioration in nursing-sensitive patient outcomes, as well as a dearth of innovative nursing projects and a reduction in clinical research due to limited finances. These developments negatively affected nurses’ work environment [5], [6], [7], [8], [9], [10]. Research has shown that an unappealing work environment impacts nurse job satisfaction [11], [12], [13], [14], [15], [16]. This may lead to an increase in job attrition amongst nurses and diminish the attractiveness of nursing as a profession; thus compounding the difficulty of recruiting and retaining nurses in an environment already strained by epidemiological and demographic changes. As a result, equitable and comprehensive patient service and patient safety would be seriously jeopardized, resulting in an increase in complications and corresponding patient mortality [5]. These consequences may raise moral concerns and conflicts regarding the ethical principles of nursing. International research shows that a lack of resources or inadequate nurse staffing lead to moral distress in nurses [17], [18]. Moral distress causes decreased job satisfaction and increased staff turnover and negatively impacts the quality of nursing care [19] and nursing-sensitive patient outcomes [5], [6].
With the recent introduction of DRGs, Switzerland has the opportunity to learn from the consequences experienced by other countries, which show far-reaching effects on nursing in acute care hospitals [20]. Their experiences point to factors influenced by DRGs that impact nurses as well as nursing care and consequently effect nursing-sensitive patient outcomes. For the further development of nursing and to ensure high quality nursing care, nurse leaders and hospital executive boards will need data on these factors in order to distribute limited resources effectively. Currently, such data are not available in most acute care hospitals in Switzerland. With this research program, our aim is to provide these crucial data by establishing a monitoring system of nursing service context factors, i.e., factors that may have an impact on nurses and on nursing care, and thus on nursing-sensitive patient outcomes. Consequently, continuous monitoring of nursing service context factors and their impact on patient outcomes needs to be an integral part of the introduction of DRGs.
In 2007, we conducted an initial pilot study at one university hospital, assessing certain nursing service context factors, which provided the basis for the current research program [21]. This program has the advantage of being part of the Sinergia project “Impact of Diagnosis Related Groups on patient care and professional practice” [22] which is supported by the Swiss National Research Foundation. Under the guidance of the Institute of Biomedical Ethics at the University of Zurich, five groups are investigating the impact of DRGs from a medical, ethical, legal and nursing perspective. This interprofessional approach enables the monitoring of nursing service context factors to inform other disciplines such as medicine, law, and ethics. Other disciplines can learn about the nursing perspective and all can gain from the exchange with the other disciplines, be it through content or methods.
Guiding theoretical model
Figure 1 (Fig. 1) depicts our theoretical model, which functions as a guide to examining the impact of the DRG-payment system on nursing service context factors and on nursing-sensitive patient outcomes. Based on the literature, we postulate effects as indicated by arrows. Related nursing service context factors are shown en bloc. While in fact relationships between single factors will be explored, the arrows in the model are simplified to improve the overview, and they show the direction of effects, which we examine with our actual study.
Figure 1. Monitoring model of the nursing service context factors.
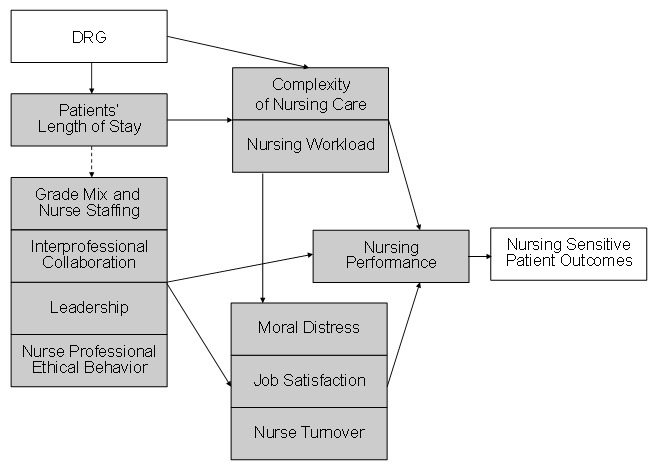
According to our model, in addition to other factors, the DRG payment system decreases patients’ LOS. Patients’ LOS may influence the complexity of nursing care and nurses’ workload, which in turn may impact nurse performance (an element of quality of care) and nursing-sensitive patient outcomes. However, patients’ LOS may also have an influence on nurse staffing and grade mix as well as on factors in nurses’ work environment such as interprofessional collaboration and leadership. Additionally, patients’ LOS may pose a challenge to leadership, and nurses’ professional ethics. These nursing service context factors may affect experiences of moral distress, job satisfaction, and nurse turnover, which, for their part, also impact nurse performance and nursing-sensitive patient outcomes [23], [24].
For our research program, we describe the nursing service context factors as follows.
Patients’ LOS
Evidence shows that due to shortened LOS under DRGs, complexity of nursing care and nurse workload increase [25], [26], [27]. Consequently, there is a growing need for competent nurses who are able to manage complex patient situations within a compressed timeframe. Current literature has found that higher registered nurse-patient ratios reduced LOS [28]. This indicates that registered nurses may be more effective than other nursing staff as they can use their range of knowledge and skills without supervision [29]. LOS was determined by the number of midnight bed occupancy days [30].
Grade mix and nurse staffing
Grade mix describes the mix of the entire nursing staff on a patient unit, with registered and auxiliary nurses, and nursing aids. Since Aiken’s landmark study in 1994, evidence has been building that higher nurse staffing levels in acute care hospitals are associated with better quality of patient care [31]. Several authors have found that as the proportion of registered nurses increased, adverse outcomes decreased [6], [32], [33], [34]. Multiple studies have shown that patients were more satisfied with nursing care on units with a higher proportion of registered nurses [14], [35], [36]. Moreover, the results of a current Swiss study indicate a similar line of reasoning [37].
Interprofessional collaboration
Interprofessional collaboration between nurses and physicians is an important aspect of nurses’ work environment [38], [39]. Better collaboration between nurses and physicians is associated with higher job satisfaction in nurses [40]. More specifically, improved communication and relationships among nurses and other providers, including physicians, is associated with increased quality of patient care [41]. An additional aspect is that a lack of autonomy for nurses in their collaborative work with physicians increases moral distress in nurses [42], [43].
Leadership
Leadership describes the process of unifying people around shared values and inspiring them to work toward a shared vision. Effective leadership is essential to high-quality nursing care, more specifically to patient-centred, evidence-based care and improved nursing-sensitive patient outcomes [39], [44], [45], [46]. There is increased pressure to develop effective leadership that will facilitate meaningful practice. Transformational leadership is an approach that aims to build successful working teams. A meta-analysis revealed that transformational leadership was associated with increased effectiveness of workers [47]. Transformational leaders had staff members who reported higher satisfaction levels, identified more strongly with the workplace, showed more dedication to their jobs and changed jobs less frequently [24]. Our pilot data indicate the existence of strong transformational leadership and underline the value of maintaining this under DRGs [21].
Nurses’ professional ethics
The term nurses’ professional ethics relates to the extent to which nurses consider ethical principles in their daily practice. In Switzerland, the ethical guidelines of the Swiss Nurses Association require nurses to offer professional, safe, and equitable nursing care, which protects patients from harm, respects their autonomy, their needs, preferences and resources and supports their health-related goals [48]. While nurses are expected to act according to these ethical guidelines, the degree to which individual nurses internalize or apply them may vary. DRGs may engender more ethically challenging situations in nursing practice. Nurses with a high sensitivity regarding ethical issues may experience more moral distress [49].
Complexity of nursing care
Complexity of nursing care describes the demands on professional nursing in the acute care hospital setting. It refers to a patient’s situation and the related decision making process regarding planning and subsequent interventions. The extent of the complexity is determined by the degree of instability, variability and uncertainty that exist in a patient’s situation. These factors are influenced by consequences of disease and associated therapies on the patient and his or her everyday life situation. They are also influenced by decisions made regarding care and interventions to achieve the best possible outcome for the patient.
As a consequence of DRGs, only the most complex patients are admitted to acute care hospitals, where treatment and care are highly multifaceted. Patients’ safety may be at risk regarding preventable conditions such as pressure sores and urinary tract infections, since these conditions are related to nurse staffing per patient acuity and complexity [50]. Research has shown a significant correlation between LOS and complexity of nursing care [25].
Nursing workload
Nursing workload includes both nursing work undertaken on behalf of the patient and non-patient related work, e.g. education of team members and organisational and administrative work [51]. Nurses’ perception of workload is mediated by the presence of experienced nurses on the unit and is worsened by the use of excessive overtime [52]. Workload is also influenced by patient turnover which increases with reduced LOS (due to the introduction of DRGs or new medical treatments, for example) [27], [53]; and it is also dependant on adequate staffing [54], [55]. High workload appears to compromise quality of nursing care [56], [57], [58]. Additionally, nurse workload has an impact on moral distress, job satisfaction and nurse turnover [6], [56], [59], [60].
Moral distress
Moral distress describes the burden experienced by a nurse who believes he or she knows the ethically appropriate course of action to take regarding nursing care, but feels constrained from taking that action. Moral distress can trigger emotional and physical reactions in nurses and can cause them to withdraw emotionally from patients. It can also lead them to change their place of work or even cause them to leave the nursing profession altogether [19], [61], [62]. The literature shows that high moral distress decreases job satisfaction and consequently increases nurse turnover [59]. Currently, there is a lack of evidence regarding the relationship between moral distress and quality of care or nursing-sensitive patient outcomes, indicating a need for further research in the field of nursing [17], [63].
Job satisfaction
Job satisfaction refers to both, satisfaction with the nursing profession in general as well as to satisfaction with the current workplace. The latter includes satisfaction with salary, work, supervision, professional opportunities, organisational practices and relationships within the interprofessional team [64]. Research has shown that greater visibility, responsiveness, and better support by nurse leaders are linked to higher job satisfaction amongst nurses [11]. Leadership behaviour affects job satisfaction, productivity, and organisational commitment. Nurses’ job satisfaction is related to environmental characteristics such as adequate staffing. In the pilot study, the majority of nurses were somewhat satisfied (55%) or very satisfied (28.7%) with their workplace and these results were even higher for satisfaction with the nursing profession, i.e. 48.7% somewhat satisfied and 44.8% very satisfied (N=636). However, in spite of this high level of satisfaction, only 10.6% of the nurses would recommend nursing as a profession to others [21].
Nurse turnover
Nurse turnover is the process whereby nurses resign or change positions. A high or continuous rate of nurse turnover jeopardises experienced teams [24]. A meta-analysis found that the best predictors of nurse turnover are job satisfaction, organisational commitment, job alternatives, withdrawal cognitions, and intention to leave [65]. Only a few studies have linked nurse turnover to quality of nursing care but the results suggest that nurse turnover might also affect quality of nursing care [66]. In our pilot, the turnover rate ranged from 5.8% up to 12.3% throughout all hospital departments [21]. However, it is unknown which turnover rate negatively influences quality of care. It is hoped that the monitoring will provide data in this regard.
Nursing performance
Nursing performance is a heterogeneously defined concept comprising various organizational frameworks and measurements. However, there is consensus that Donabedian’s model of quality identifying structure, process and outcomes should be taken into account in nursing performance research [67], [68].
We define nursing performance as the extent to which those nursing care interventions deemed to be necessary for achieving desirable patient outcomes, have been fully carried out for a particular patient. The necessity of an intervention is based on a professional assessment and judgment of each individual patient’s care needs and preferences, the defined care and treatment goals and current best nursing practice. Studies show that a wide range of factors such as nurse training and competencies, structures, nursing organization, leadership and interprofessional collaboration influence nursing performance. Studies also indicate that nursing performance influences service outcomes and ultimately patient outcomes [67], [68], [69]. Several studies indicate a link between the omission of necessary nursing care and a decrease in quality of care and/or the occurrence of negative nursing-sensitive patient outcomes (adverse events) [37], [70], [71], [72], [73], [74], [75], [76].
Nursing sensitive patient outcomes
The measurement of nursing sensitive patient outcomes in our research program is limited to the available outcome data in Swiss acute care hospitals; that is falls and pressure ulcers as measured by the National Association for Quality Development in Hospitals and Clinics (ANQ), the official Swiss institution that measures quality indicators on a yearly basis [77]. This national prevalence measurement takes place in cooperation with the Maastricht University [78]. In it falls are defined as an event that causes the patient to unintentionally fall to the ground or some lower level, regardless of the cause [78]. Pressure ulcers are defined according to the definition of the National Pressure Ulcer Advisory Panel and European Pressure Ulcer Advisory Panel [78], [79]. Studies show that falls and pressure ulcers are nursing sensitive patient outcomes [80], [81].
In summary, there is currently a dearth of knowledge regarding the impact of the DRG payment system on nursing service context factors and consequently on the influence of these factors on nursing performance and nursing-sensitive patient outcomes in Swiss acute care hospitals. There is little data on nursing service context factors in Switzerland or other German-speaking countries and no monitoring of these factors in this context. For certain relevant nursing service context factors, measurement instruments are not yet available in German. Within our research program, an initial survey of nursing service context factors has been conducted at three university hospitals and two cantonal hospitals. With its mixed methods approach, this research program will generate new and complementary insights with quantitative and qualitative data, allowing us to develop and validate instruments and to test the theoretical model for future use. Accordingly, it is hoped that our findings will provide an important starting point with an initial set of data regarding the period prior to DRG introduction, a defined theoretical model, and valid instruments to measure relevant nursing service context factors. Based on this research program, nursing service context factors can be monitored post DRG introduction at regular intervals and changes will become apparent. Nursing leaders and hospital executive boards will have the data necessary to ensure adequate quality of nursing care. Good nursing-sensitive patient outcomes will be achieved through the most effective use of limited resources.
Aim of the research program and research questions
The aim is to prepare and conduct an initial survey of nursing service context factors at three university hospitals and two cantonal hospitals prior to DRG introduction, to explore nurses’ perspectives on nursing service context factors, and to further develop a theoretical model and methodology for future monitoring post DRG introduction.
The overall research questions are:
Which are relevant nursing service context factors to be included in a monitoring model to investigate the impact of DRGs on nursing sensitive patient outcomes in the acute care setting?
What are relevant interactions between these factors?
What are relevant effects between these factors and nursing sensitive outcomes?
What are the elements of a set of reliable, valid and usable instruments to conduct a monitoring of these factors over time?
Methodology and research plan
Design
A mixed methods design (Figure 2 (Fig. 2)) in the form of a sequential explanatory strategy was chosen [82].
Figure 2. Design of the mixed methods study.
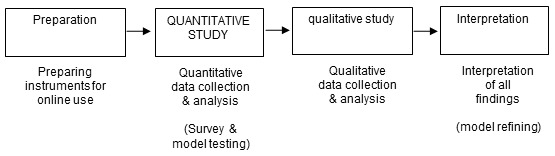
Whilst quantitative data make it possible to identify relevant measures precisely, qualitative data describe processes in detail, thus giving a greater level of insight. This was the reason for supplementing quantitative data with qualitative data gathered through focus group interviews. This method is particularly suited to exploring views on a specific theme within a social context. The results of all analyses will be interpreted by comparing and contrasting qualitative and quantitative findings to strengthen the evidence.
Preparation
After obtaining consent from hospital executive boards and nursing directors, a steering board was established to oversee the progress of the research program and to guarantee financial support. The steering board comprised representatives of the participating hospitals under the supervision of the principle investigator. A project team, including one representative from each hospital, was responsible for day-to-day management under the guidance of the project manager. Since hospitals differ regarding organizational structure, the project team members ensured high quality data by adapting data collection processes to each hospital. During the preparatory phase, a reflection board, with experienced quantitative researchers and statisticians, supported the project manager by scrutinising decisions regarding instruments and data collection. German versions of the instruments for measuring complexity of nursing care and moral distress were developed and pilot tested, given that there were no available instruments suitable for this study.
Quantitative study
The unit of analysis in the quantitative study was the hospital ward. All 204 wards of the study hospitals were invited to participate. The quantitative study had four parts: 1) nurse survey, 2) evaluation of ward managers’ leadership practices, 3) assessment of complexity of nursing care, and 4) collection of hospital data on LOS, nursing-sensitive patient outcomes and grade mix.
Study sample
For the nurse survey, all approximately 5,100 nurses with a nursing diploma and direct involvement in nursing care of all units of the participating three university hospitals and two cantonal hospitals were invited to participate. Regarding self-assessment and observer-assessment of leadership practices, supervisors and team members of all ward managers who agreed to participate were invited. For the assessment of the complexity of nursing care on the same units, based on the experiences of a previous pilot study over one month with approximately 300 patients, we decided to include every newly admitted patient on every unit over a time period of four weeks in our study. Nursing-sensitive patient outcomes were made available by ANQ [77].
Data collection
Questionnaires for the nurse survey and the evaluation of ward managers’ leadership were made available online. Nurses assessed complexity of nursing care on the first and third day of patients’ hospital stay, either online if an electronic patient documentation system was available or on paper. The nursing-sensitive patient outcome ‘fall and pressure ulcer prevalence’ was measured on one specific day at all hospitals. Medical statistics and human resources departments from each hospital provided LOS and nursing staff data.
Measurement variables
In order for our monitoring to be effective in Swiss acute care settings, we aim to produce a set of practical and concise instruments in German that are valid and reliable. To this end, we examined each nursing service context factor to ascertain whether existing hospital data bases could be utilized. If not, available instruments were used and/or adapted as needed. To measure leadership, we used the German version of the Leadership Practice Inventory (LPI) that was translated but not yet validated in our initial pilot study [83]. In the case of moral distress and complexity of nursing care, instruments for the local context were developed based on existing English-language questionnaires. Establishing the validity and reliability of the set of instruments will be part of this study.
Table 1 (Tab. 1) lists the variables and their respective measurement methods. In addition, socio-demographic and professional variables were recorded (age, training, numbers of years of experience, employment grade and length of employment).
Table 1. Variables of the study, their measurement methods and sources of data.

Data analysis
Descriptive analyses: The data were summarized using descriptive statistics. For interval data, central tendency was calculated as mean, median, minimum and maximum. Dispersion was calculated as range, standard deviation and interquartile range. The data were depicted in box plots. Frequencies and proportions were calculated for ordinal and nominal variables. In the case of ordinal variables, mean, median, minimum and maximum were also calculated. These data were depicted in bar charts.
Regression analyses: Multiple regression models will be used to examine the relationships as shown in Figure 1 (Fig. 1). Because our sample consists of wards and nurses within wards, a multilevel structure will be in the data. Nurses in the same ward tend to be more similar to each other than nurses across different wards because of their shared environment. Standard statistical tests do not account for this and, as a result, deliver invalid p values. This can be rectified with multi-level models, which permit an incorporation of explanatory variables both on the individual and ward level. Random class effects for intercepts and slopes will be tested as well as interactions between individual and ward level variables. Variable selection will be based on the Akaike information criterion (AIC).
Qualitative study
The qualitative study was conducted by means of focus group interviews and employing a content analysis approach with knowledge mapping. It consisted of three thematic parts: 1) The meaning of the quantitative study results was explored more extensively. In order to further develop our newly composed measurement instruments, 2) experiences with moral distress and 3) perspectives on complexity of nursing care were explored. A board of experienced qualitative researchers supported each step of the qualitative study section by means of critical reflection.
Study sample and settings
In this research program, focus groups included six to ten participants. Purposive sampling was used to ensure the participation of nurses from different specialities.
To explore the meaning of the quantitative study results, 20 focus group interviews were conducted, with four interviews in each hospital. One interview was conducted per professional group: one group of registered nurses, one of clinical nurse specialists, and one of ward managers. After the preliminary analyses, an additional interview was conducted with registered nurses to explore questions that had arisen in previous interviews. To understand moral distress in the cultural context, four additional focus groups were conducted at University Hospital Zurich: two with registered nurses, one with clinical nurse specialists, and one with ward managers. To further explore complexity of nursing care, four focus groups were conducted at University Hospital Zurich and one additional interview with experienced nurses at each of the other hospitals.
Data collection
Two methods were applied for data collection: focus group interviews and knowledge mapping. Focus group interviews are interviews with groups of approximately five to fifteen people in which participants’ attitudes and opinions are investigated [84]. Knowledge mapping belongs to a content analysis method that begins in the phase of data collection. In this phase, pictures/visual aids are created that represent the mappers' understanding of particular elements of the group discussion. With knowledge mapping, an increased transparency is possible by means of a critical member checking and further developing the maps at the end of each interview [85].
All but one focus group interview were carried out by the same moderator while co-moderators varied. Discussions were stimulated by the moderator offering a brief input regarding quantitative results. The moderator then used specific interview guides with open questions for the nursing context factors of interest. The co-moderators generated knowledge maps from each interview. Towards the end of the interview, the co-moderator presented the knowledge map to the group and asked for feedback. The discussions were tape recorded. Focus group interviews lasted about 120 minutes.
Data analysis
Content analysis techniques, in combination with the technique of knowledge mapping, were used [85], [86] to efficiently reduce the large quantity of material to a manageable size and to extract the significant content. Moreover, the knowledge maps from the interviews underwent further analysis by summarising, explicating and structuring. Summary maps were developed by topic and were checked by listening to tapes. The reflection board met three times to review the maps and to interpret the material according to the relevant research questions. Final structuring provided our theoretical model.
The reliability of the results was ensured by having one moderator who guided all but one of the focus group interviews, by the precise documenting of the data collection procedure and the analysis process, as well as by the reflection board’s in-depth discussions of the maps.
Interpretation
The interpretation of quantitative and qualitative results began in summer 2013 and will be accomplished by complementing, comparing and contrasting all findings. This proceeding is an important aspect of mixed methods research. Recent empirical studies of mixed methods research show a lack of mixing between the two components which limits the knowledge generation of mixed methods studies. Without interpretation, the knowledge is equivalent to that of a qualitative study and a quantitative study undertaken independently, rather than achieving a comprehensive result. The interpretation process in this research program will be conducted by using triangulation and matrix techniques [87], [88].
Triangulation
The quantitative and qualitative findings will be listed on the same pages. Our team of quantitative and qualitative researchers will then consider where findings from each method agree (convergence), offer complementary information on the same issue (complementarity), or appear to contradict each other (discrepancy or dissonance). It is important to look explicitly for dissonances since they may lead to a better understanding of the results. A triangulation protocol will help to achieve so-called meta-themes that cut across the findings from different methods [88].
Mixed methods matrix
Additionally, data from the quantitative and qualitative studies will be integrated in a mixed methods matrix. Within a mixed methods matrix, rows represent nursing service context factors or their respective sub themes, according to our guiding conceptual model. Within these themes, qualitative and quantitative data will be integrated in columns to be studied together. Data can be examined in detail for each theme, for example, responses to a questionnaire with maps or interview transcripts. This will enable us to observe similarities or variations in the data as well as unexpected data or paradoxes between data, and subsequently to look for patterns across all themes [88].
By using triangulation and matrix techniques, we will be able to generate a comprehensive interpretation and representation of monitoring the impact of the DRG-payment system on nursing service context factors in Swiss Hospitals.
Ethical issues
The research program was approved by the ethics committees of Basel, Bern, Solothurn and Zürich as well as the ethics committee of the university and cantonal hospitals. All participating nurses provided informed consent for the interviews, either online or in written form, and were assured of data confidentiality. Ward managers specifically provided permission for their observer feedback to be integrated. Focus group participants agreed to maintain confidentiality. In accordance with ethical approval, patient data and personnel data were collected in an anonymous manner.
Discussion and significance
With this research program, an initial phase of continuous monitoring of relevant nursing service context factors will be achieved. Baseline data prior to DRG introduction will be available and will yield a solid rationale whose use by nursing managers and executive boards of acute care hospitals in Switzerland can support a more effective distribution of limited resources. These data will allow later comparisons with data collected under DRGs. It is hoped that our research program will provide a model of relevant nursing service context factors that, influenced by DRGs, have an impact on nurse performance as well as nursing-sensitive patient outcomes. A methodology for use in German speaking countries to measure nursing service context factors in acute hospitals will be made available, including newly developed and tested scales for moral distress and complexity of nursing care.
Based on the baseline data of nursing service context factors and the model showing how these factors are related, nursing managers and executive boards of Swiss acute care hospitals will be able to use their local data to intervene and support nursing service in various ways. For instance, complexity of nursing care may be very high, indicating a need for changing grade mix in affected nursing teams. A low satisfaction with interprofessional collaboration and high levels of moral distress may call for an improvement in collaboration. Our pilot study showed that existing high leadership competencies in ward managers [21] were a valuable strength worth maintaining. The expected changes due to the implementation of DRGs call for recurrent monitoring that will make nursing managers and executive boards cognizant of changes in nursing service context factors while monitoring the effectiveness of their interventions on their local nursing service.
There are several reasons why the mixed methods approach in our research program is especially important. Quantitative analyses will provide the necessary data on nursing service context factors and how these factors relate to each other. With the qualitative approach, a deeper understanding of the data will be possible. The focus group interviews will allow us to observe subtle changes as experienced by nurses. Interpretation of quantitative and qualitative data will offer complementary information on the same issue, which may finally lead to a better understanding of nursing service context factors. In particular, our adapted and newly-developed instruments will profit from the mixed methods approach. For instance, the adapted items of the moral distress scale might not yet cover all situations causing moral distress in Swiss nurses. In this way, qualitative data will help to further adapt and develop the instruments to our local context.
Since all university hospitals and two cantonal hospitals in German-speaking Switzerland are participating in our research program, data represent a relevant array of Swiss German nursing. Additionally, cantonal hospitals may use our model and methodology in the future. The findings of our research program will also be useful at the political level, first and foremost as a comparison to the results of the multiprofessional Sinergia Project of the Swiss National Research Foundation. Since our five groups are investigating the impact of DRGs from a medical, ethical, legal and nursing perspective, Switzerland will be able to base decisions regarding resource allocation on multiprofessional results prior to and under DRGs. Our adapted or newly-developed instruments for measuring moral distress and complexity of nursing care will engender discussions. For instance, before we started our research program, the term moral distress was not known in nursing within our cultural context. Our research program gives us the opportunity to introduce the new instrument and to raise awareness of this newly-recognized phenomenon. Additionally, the difficulty of measuring complex patient situations shows the promise of the instrument ‘complexity of nursing care’ and calls for further development.
Our research program is a first step toward a monitoring system that would enable acute care hospitals to continuously evaluate the working conditions of their nursing staff. Subsequent monitoring will show the benefit of using the theoretical model and methodology to provide data for reliable management decisions. The study has the potential to provide results that are interesting as a benchmark between hospitals nation-wide within Switzerland as well as internationally, for the purposeful exchange of experiences in different health care contexts and cultures.
Notes
Competing interests
The authors declare that they have no competing interests.
Acknowledgements
This research program received funding from the Swiss National Foundations (CRSII3_132786/1), Käthe-Zingg-Schwichtenberg Fond, Gottfried und Julia Bangerter-Rhyner-Stiftung, and Olga Mayenfisch Stiftung.
Authors’ contributions
RS is the principle investigator of the research program. IAF, JM, ES and MKL are co-investigators. MKL is the day-to-day project and scientific manager. MM is the lead statistician of the research program. RS, MKL, JM, IAF and ES contributed equally to the implementation of the study protocol. RS, ES and MKL drafted the manuscript. All co-authors listed contributed by reading, commenting and providing feedback. All approved the final manuscript.
References
- 1.Borghans I, Heijink R, Kool T, Lagoe RJ, Westert GP. Benchmarking and reducing length of stay in Dutch hospitals. BMC Health Serv Res. 2008;8:220. doi: 10.1186/1472-6963-8-220. Available from: http://dx.doi.org/10.1186/1472-6963-8-220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Baumberger D, Bosshard W, Portenier L, Wittwer M, Bürgin R, Müller M. Projekt SwissDRG und Pflege. Teilaufgabe 1. Quantitative Analyse Pflegeaufwand. 2009. Available from: http://www.netzwerk-pflegediagnosen.ch/default/assets/File/SVPL_SBK_Report-swissDRG-und-Pflege_091014.pdf. [Google Scholar]
- 3.Carpenter I, Bobby J, Kulinskaya E, Seymour G. People admitted to hospital with physical disability have increased length of stay: implications for diagnosis related group re-imbursement in England. Age Ageing. 2007 Jan;36(1):73–78. doi: 10.1093/ageing/afl148. Available from: http://dx.doi.org/10.1093/ageing/afl148. [DOI] [PubMed] [Google Scholar]
- 4.Chuang KH, Covinsky KE, Sands LP, Fortinsky RH, Palmer RM, Landefeld CS. Diagnosis-related group-adjusted hospital costs are higher in older medical patients with lower functional status. J Am Geriatr Soc. 2003 Dec;51(12):1729–1734. doi: 10.1046/j.1532-5415.2003.51556.x. [DOI] [PubMed] [Google Scholar]
- 5.Aiken LH, Clarke SP, Sloane DM, Lake ET, Cheney T. Effects of hospital care environment on patient mortality and nurse outcomes. J Nurs Adm. 2008 May;38(5):223–229. doi: 10.1097/01.NNA.0000312773.42352.d7. Available from: http://dx.doi.org/10.1097/01.NNA.0000312773.42352.d7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA. 2002 Oct 23-30;288(16):1987–1993. doi: 10.1001/jama.288.16.1987. Available from: http://dx.doi.org/10.1001/jama.288.16.1987. [DOI] [PubMed] [Google Scholar]
- 7.Aiken LH. Breaking the shortage cycles. Am J Nurs. 1987;87(12):1616–1620. doi: 10.2307/3425976. Available from: http://dx.doi.org/10.2307/3425976. [DOI] [Google Scholar]
- 8.Aiken LH, Clarke SP, Sloane DM. Hospital restructuring: does it adversely affect care and outcomes? J Nurs Adm. 2000 Oct;30(10):457–465. doi: 10.1097/00005110-200010000-00003. [DOI] [PubMed] [Google Scholar]
- 9.Bartholomeyczik S. Schnellerer Durchlauf kränkerer Patienten im Krankenhaus: Wo bleibt die Pflege? Ethik in der Medizin. 2011 Dec;23(4):315–325. doi: 10.1007/s00481-011-0160-x. Available from: http://dx.doi.org/10.1007/s00481-011-0160-x. [DOI] [Google Scholar]
- 10.Braun B, Klinke S, Müller R, Rosenbrock R. Einfluss der DRGs auf Arbeitsbedingungen und Versorgungsqualität von Pflegekräften im Krankenhaus – Ergebnisse einer bundesweiten schriftlichen Befragung repräsentativer Stichproben von Pflegekräften an Akutkrankenhäusern in den Jahren 2003, 2006 und 2008. Bremen: Universität Bremen, Artec Forschungszentrum Nachhaltigkeit; 2011. (artec-paper; 173). Available from: http://www.uni-bremen.de/fileadmin/user_upload/single_sites/artec/artec_Dokumente/artec-paper/173_paper.pdf. [Google Scholar]
- 11.Hegney D, Plank A, Parker V. Extrinsic and intrinsic work values: their impact on job satisfaction in nursing. J Nurs Manag. 2006 May;14(4):271–281. doi: 10.1111/j.1365-2934.2006.00618.x. Available from: http://dx.doi.org/10.1111/j.1365-2934.2006.00618.x. [DOI] [PubMed] [Google Scholar]
- 12.Kramer M, Schmalenberg C. Magnet hospitals talk about the impact of DRGs on nursing care – Part II. Nurs Manage. 1987 Oct;18(10):33–6, 38. [PubMed] [Google Scholar]
- 13.Zander B, Dobler L, Busse R. The introduction of DRG funding and hospital nurses’ changing perceptions of their practice environment, quality of care and satisfaction: comparison of cross-sectional surveys over a 10-year period. Int J Nurs Stud. 2013 Feb;50(2):219–229. doi: 10.1016/j.ijnurstu.2012.07.008. Available from: http://dx.doi.org/10.1016/j.ijnurstu.2012.07.008. [DOI] [PubMed] [Google Scholar]
- 14.Aiken LH, Sermeus W, Van den Heede K, Sloane DM, Busse R, McKee M, Bruyneel L, Rafferty AM, Griffiths P, Moreno-Casbas MT, Tishelman C, Scott A, Brzostek T, Kinnunen J, Schwendimann R, Heinen M, Zikos D, Sjetne IS, Smith HL, Kutney-Lee A. Patient safety, satisfaction, and quality of hospital care: cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ. 2012 Mar 20;344:e1717. doi: 10.1136/bmj.e1717. Available from: http://dx.doi.org/10.1136/bmj.e1717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Milisen K, Abraham I, Siebens K, Darras E, Dierckx de Casterlé B BELIMAGE group. Work environment and workforce problems: a cross-sectional questionnaire survey of hospital nurses in Belgium. Int J Nurs Stud. 2006 Aug;43(6):745–754. doi: 10.1016/j.ijnurstu.2005.10.008. Available from: http://dx.doi.org/10.1016/j.ijnurstu.2005.10.008. [DOI] [PubMed] [Google Scholar]
- 16.Van Bogaert P, Meulemans H, Clarke S, Vermeyen K, Van de Heyning P. Hospital nurse practice environment, burnout, job outcomes and quality of care: test of a structural equation model. J Adv Nurs. 2009 Oct;65(10):2175–2185. doi: 10.1111/j.1365-2648.2009.05082.x. [DOI] [PubMed] [Google Scholar]
- 17.Schluter J, Winch S, Holzhauser K, Henderson A. Nurses’ moral sensitivity and hospital ethical climate: a literature review. Nurs Ethics. 2008 May;15(3):304–321. doi: 10.1177/0969733007088357. Available from: http://dx.doi.org/10.1177/0969733007088357. [DOI] [PubMed] [Google Scholar]
- 18.Bentzen G, Harsvik A, Brinchmann BS. “Values that vanish into thin air”: nurses’ experience of ethical values in their daily work. Nurs Res Pract. 2013;2013:939153. doi: 10.1155/2013/939153. Available from: http://dx.doi.org/10.1155/2013/939153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hamric AB, Davis WS, Childress MD. Moral distress in health care professionals. Pharos Alpha Omega Alpha Honor Med Soc. 2006;69(1):16–23. [PubMed] [Google Scholar]
- 20.Norrish BR, Rundall TG. Hospital restructuring and the work of registered nurses. Milbank Q. 2001;79(1):55–79. doi: 10.1111/1468-0009.00196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Martin JS, Frei IA, Suter-Hofmann F, Fierz K, Schubert M, Spirig R. Evaluation der Pflege- und Führungskompetenz – eine Ausgangslage für die weitere Praxisentwicklung. [Evaluation of nursing and leadership competencies – a baseline for practice development]. Pflege. 2010 Jun;23(3):191–203. doi: 10.1024/1012-5302/a000039. (Ger). Available from: http://dx.doi.org/10.1024/1012-5302/a000039. [DOI] [PubMed] [Google Scholar]
- 22.Biller-Andorno N, Wild V. Assessing the impact of Diagnosis Related Groups (DRGs) on patient care and professional practice: an interdisciplinary approach. Zürich: Universität Zürich – Ethik-Zentrum – Institut für Biomedizinische Ethik; 2010. [cited 2013 Feb 5]. Available from: http://www.ethik.uzh.ch/ibme/forschung/drg/generalinformation.html. [Google Scholar]
- 23.Currie V, Harvey G, West E, McKenna H, Keeney S. Relationship between quality of care, staffing levels, skill mix and nurse autonomy: literature review. J Adv Nurs. 2005 Jul;51(1):73–82. doi: 10.1111/j.1365-2648.2005.03462.x. Available from: http://dx.doi.org/10.1111/j.1365-2648.2005.03462.x. [DOI] [PubMed] [Google Scholar]
- 24.Houser J. A model for evaluating the context of nursing care delivery. J Nurs Adm. 2003 Jan;33(1):39–47. doi: 10.1097/00005110-200301000-00008. Available from: http://dx.doi.org/10.1097/00005110-200301000-00008. [DOI] [PubMed] [Google Scholar]
- 25.Graf CM, Millar S, Feilteau C, Coakley PJ, Erickson JI. Patients' needs for nursing care: beyond staffing ratios. J Nurs Adm. 2003 Feb;33(2):76–81. doi: 10.1097/00005110-200302000-00003. Available from: http://dx.doi.org/10.1097/00005110-200302000-00003. [DOI] [PubMed] [Google Scholar]
- 26.Hader R, Claudio T. Seven methods to effectively manage patient care labor resources. J Nurs Adm. 2002 Feb;32(2):66–68. doi: 10.1097/00005110-200202000-00002. Available from: http://dx.doi.org/10.1097/00005110-200202000-00002. [DOI] [PubMed] [Google Scholar]
- 27.Duffield C, Diers D, Aisbett C, Roche M. Churn: patient turnover and case mix. Nurs Econ. 2009 May-Jun;27(3):185–191. [PubMed] [Google Scholar]
- 28.Thungjaroenkul P, Cummings GG, Embleton A. The impact of nurse staffing on hospital costs and patient length of stay: a systematic review. Nurs Econ. 2007 Sep-Oct;25(5):255–265. [PubMed] [Google Scholar]
- 29.Burger JL, Parker K, Cason L, Hauck S, Kaetzel D, O'Nan C, White A. Responses to work complexity: the novice to expert effect. West J Nurs Res. 2010 Jun;32(4):497–510. doi: 10.1177/0193945909355149. Available from: http://dx.doi.org/10.1177/0193945909355149. [DOI] [PubMed] [Google Scholar]
- 30.Marik PE, Hedman L. What’s in a day? Determining intensive care unit length of stay. Crit Care Med. 2000 Jun;28(6):2090–2093. doi: 10.1097/00003246-200006000-00071. Available from: http://dx.doi.org/10.1097/00003246-200006000-00071. [DOI] [PubMed] [Google Scholar]
- 31.Aiken L. Good nursing care = lower death rates. N J Nurse. 1994 Oct;24(8):1. [PubMed] [Google Scholar]
- 32.Blegen MA, Goode CJ, Reed L. Nurse staffing and patient outcomes. Nurs Res. 1998 Jan-Feb;47(1):43–50. doi: 10.1097/00006199-199801000-00008. Available from: http://dx.doi.org/10.1097/00006199-199801000-00008. [DOI] [PubMed] [Google Scholar]
- 33.Penoyer DA. Nurse staffing and patient outcomes in critical care: a concise review. Crit Care Med. 2010 Jul;38(7):1521–1528. doi: 10.1097/CCM.0b013e3181e47888. Available from: http://dx.doi.org/10.1097/CCM.0b013e3181e47888. [DOI] [PubMed] [Google Scholar]
- 34.Harless DW, Mark BA. Nurse staffing and quality of care with direct measurement of inpatient staffing. Med Care. 2010 Jul;48(7):659–663. doi: 10.1097/MLR.0b013e3181dbe200. Available from: http://dx.doi.org/10.1097/MLR.0b013e3181dbe200. [DOI] [PubMed] [Google Scholar]
- 35.McGillis Hall L, Doran D, Baker GR, Pink GH, Sidani S, O’Brien-Pallas L, Donner GJ. Nurse staffing models as predictors of patient outcomes. Med Care. 2003 Sep;41(9):1096–1109. doi: 10.1097/01.MLR.0000084180.07121.2B. Available from: http://dx.doi.org/10.1097/01.MLR.0000084180.07121.2B. [DOI] [PubMed] [Google Scholar]
- 36.Needleman J, Buerhaus P, Mattke S, Stewart M, Zelevinsky K. Nurse-staffing levels and the quality of care in hospitals. N Engl J Med. 2002 May;346(22):1715–1722. doi: 10.1056/NEJMsa012247. Available from: http://dx.doi.org/10.1056/NEJMsa012247. [DOI] [PubMed] [Google Scholar]
- 37.Schubert M, Glass TR, Clarke SP, Aiken LH, Schaffert-Witvliet B, Sloane DM, De Geest S. Rationing of nursing care and its relationship to patient outcomes: the Swiss extension of the International Hospital Outcomes Study. Int J Qual Health Care. 2008 Aug;20(4):227–237. doi: 10.1093/intqhc/mzn017. Available from: http://dx.doi.org/10.1093/intqhc/mzn017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Aiken LH, Patrician PA. Measuring organizational traits of hospitals: the Revised Nursing Work Index. Nurs Res. 2000 May-Jun;49(3):146–153. doi: 10.1097/00006199-200005000-00006. Available from: http://dx.doi.org/10.1097/00006199-200005000-00006. [DOI] [PubMed] [Google Scholar]
- 39.Manojlovich M. The effect of nursing leadership on hospital nurses’ professional practice behaviors. J Nurs Adm. 2005 Jul-Aug;35(7-8):366–374. [PubMed] [Google Scholar]
- 40.Gunnarsdóttir S, Clarke SP, Rafferty AM, Nutbeam D. Front-line management, staffing and nurse-doctor relationships as predictors of nurse and patient outcomes. a survey of Icelandic hospital nurses. Int J Nurs Stud. 2009 Jul;46(7):920–927. doi: 10.1016/j.ijnurstu.2006.11.007. Available from: http://dx.doi.org/10.1016/j.ijnurstu.2006.11.007. [DOI] [PubMed] [Google Scholar]
- 41.Havens DS, Vasey J, Gittell JH, Lin WT. Relational coordination among nurses and other providers: impact on the quality of patient care. J Nurs Manag. 2010 Nov;18(8):926–937. doi: 10.1111/j.1365-2834.2010.01138.x. Available from: http://dx.doi.org/10.1111/j.1365-2834.2010.01138.x. [DOI] [PubMed] [Google Scholar]
- 42.Papathanassoglou ED, Karanikola MN, Kalafati M, Giannakopoulou M, Lemonidou C, Albarran JW. Professional autonomy, collaboration with physicians, and moral distress among European intensive care nurses. Am J Crit Care. 2012 Mar;21(2):e41–e52. doi: 10.4037/ajcc2012205. Available from: http://dx.doi.org/10.4037/ajcc2012205. [DOI] [PubMed] [Google Scholar]
- 43.Karanikola MN, Albarran JW, Drigo E, Giannakopoulou M, Kalafati M, Mpouzika M, Tsiaousis GZ, Papathanassoglou ED. Moral distress, autonomy and nurse-physician collaboration among intensive care unit nurses in Italy. J Nurs Manag. 2013 Mar 14; doi: 10.1111/jonm.12046. Available from: http://dx.doi.org/10.1111/jonm.12046. [DOI] [PubMed] [Google Scholar]
- 44.Manojlovich M. Promoting nurses’ self-efficacy: a leadership strategy to improve practice. J Nurs Adm. 2005 May;35(5):271–278. doi: 10.1097/00005110-200505000-00011. [DOI] [PubMed] [Google Scholar]
- 45.Kramer M, Schmalenberg C, Maguire P. Essentials of a magnetic work environment: part 3. Nursing. 2004 Aug;34(8):44–47. doi: 10.1097/00152193-200408000-00050. Available from: http://dx.doi.org/10.1097/00152193-200408000-00050. [DOI] [PubMed] [Google Scholar]
- 46.Alleyne J, Jumaa MO. Building the capacity for evidence-based clinical nursing leadership: the role of executive co-coaching and group clinical supervision for quality patient services. J Nurs Manag. 2007 Mar;15(2):230–243. doi: 10.1111/j.1365-2834.2007.00750.x. Available from: http://dx.doi.org/10.1111/j.1365-2834.2007.00750.x. [DOI] [PubMed] [Google Scholar]
- 47.Lowe KB, Kroeck KG, Sivasubramaniam N. Effectiveness correlates of transformational and transactional leadership: a meta-analytic review of the MLQ literature. Leadership Quarterly. 1996;7(3):385–425. doi: 10.1016/S1048-9843(96)90027-2. Available from: http://dx.doi.org/10.1016/S1048-9843(96)90027-2. [DOI] [Google Scholar]
- 48.Schweizerischer Berufsverband der Pflegefachfrauen und Pflegefachmänner SBK. Ethische Standpunkte 2. Verantwortung und Pflegequalität. Bern: Schweizerischer Berufsverband der Pflegefachfrauen und Pflegefachmänner; 2007. [Google Scholar]
- 49.Austin W. Moral distress and the contemporary plight of health professionals. HEC Forum. 2012 Mar;24(1):27–38. doi: 10.1007/s10730-012-9179-8. Available from: http://dx.doi.org/10.1007/s10730-012-9179-8. [DOI] [PubMed] [Google Scholar]
- 50.McGillis Hall L, Doran D, Pink GH. Nurse staffing models, nursing hours, and patient safety outcomes. J Nurs Adm. 2004 Jan;34(1):41–45. doi: 10.1097/00005110-200401000-00009. [DOI] [PubMed] [Google Scholar]
- 51.Morris R, MacNeela P, Scott A, Treacy P, Hyde A. Reconsidering the conceptualization of nursing workload: literature review. J Adv Nurs. 2007 Mar;57(5):463–471. doi: 10.1111/j.1365-2648.2006.04134.x. Available from: http://dx.doi.org/10.1111/j.1365-2648.2006.04134.x. [DOI] [PubMed] [Google Scholar]
- 52.Capuano T, Bokovoy J, Hitchings K, Houser J. Use of a validated model to evaluate the impact of the work environment on outcomes at a magnet hospital. Health Care Manage Rev. 2005 Jul-Sep;30(3):229–236. doi: 10.1097/00004010-200507000-00007. Available from: http://dx.doi.org/10.1097/00004010-200507000-00007. [DOI] [PubMed] [Google Scholar]
- 53.Unruh LY, Fottler MD. Patient turnover and nursing staff adequacy. Health Serv Res. 2006 Apr;41(2):599–612. doi: 10.1111/j.1475-6773.2005.00496.x. Available from: http://dx.doi.org/10.1111/j.1475-6773.2005.00496.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Kalisch BJ, Friese CR, Choi SH, Rochman M. Hospital nurse staffing: choice of measure matters. Med Care. 2011 Aug;49(8):775–779. doi: 10.1097/MLR.0b013e318222a6df. Available from: http://dx.doi.org/10.1097/MLR.0b013e318222a6df. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Myny D, Van Goubergen D, Gobert M, Vanderwee K, Van Hecke A, Defloor T. Non-direct patient care factors influencing nursing workload: a review of the literature. J Adv Nurs. 2011 Oct;67(10):2109–2129. doi: 10.1111/j.1365-2648.2011.05689.x. Available from: http://dx.doi.org/10.1111/j.1365-2648.2011.05689.x. [DOI] [PubMed] [Google Scholar]
- 56.Holden RJ, Scanlon MC, Patel NR, Kaushal R, Escoto KH, Brown RL, Alper SJ, Arnold JM, Shalaby TM, Murkowski K, Karsh BT. A human factors framework and study of the effect of nursing workload on patient safety and employee quality of working life. BMJ Qual Saf. 2011 Jan;20(1):15–24. doi: 10.1136/bmjqs.2008.028381. Available from: http://dx.doi.org/10.1136/bmjqs.2008.028381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Gurses AP, Carayon P, Wall M. Impact of performance obstacles on intensive care nurses’ workload, perceived quality and safety of care, and quality of working life. Health Serv Res. 2009 Apr;44(2 Pt 1):422–443. doi: 10.1111/j.1475-6773.2008.00934.x. Available from: http://dx.doi.org/10.1111/j.1475-6773.2008.00934.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Pearson A, Pallas LO, Thomson D, Doucette E, Tucker D, Wiechula R, Long L, Porritt K, Jordan Z. Systematic review of evidence on the impact of nursing workload and staffing on establishing healthy work environments. Int J Evid Based Healthc. 2006 Dec;4(4):337–384. doi: 10.1111/j.1479-6988.2006.00055.x. Available from: http://dx.doi.org/10.1111/j.1479-6988.2006.00055.x. [DOI] [PubMed] [Google Scholar]
- 59.Hart SE. Hospital ethical climates and registered nurses’ turnover intentions. J Nurs Scholarsh. 2005;37(2):173–177. doi: 10.1111/j.1547-5069.2005.00030.x. [DOI] [PubMed] [Google Scholar]
- 60.Gaudine A, Thorne L. Ethical conflict in professionals Nurses’ accounts of ethical conflict with organizations. In: Primeaux P, Pava ML, editors. Symposium on Health Care Ethics. JAI/Emerald; 2000. pp. 41–58. (Research in Ethical Issues in Organizations; 2). [Google Scholar]
- 61.Lützén K, Kvist BE. Moral distress: a comparative analysis of theoretical understandings and inter-related concepts. HEC Forum. 2012 Mar;24(1):13–25. doi: 10.1007/s10730-012-9178-9. Available from: http://dx.doi.org/10.1007/s10730-012-9178-9. [DOI] [PubMed] [Google Scholar]
- 62.Corley MC. Moral distress of critical care nurses. Am J Crit Care. 1995 Jul;4(4):280–285. [PubMed] [Google Scholar]
- 63.Hamric AB. Empirical research on moral distress: issues, challenges, and opportunities. HEC Forum. 2012 Mar;24(1):39–49. doi: 10.1007/s10730-012-9177-x. Available from: http://dx.doi.org/10.1007/s10730-012-9177-x. [DOI] [PubMed] [Google Scholar]
- 64.Lu H, While AE, Barriball KL. Job satisfaction among nurses: a literature review. Int J Nurs Stud. 2005 Feb;42(2):211–227. doi: 10.1016/j.ijnurstu.2004.09.003. Available from: http://dx.doi.org/10.1016/j.ijnurstu.2004.09.003. [DOI] [PubMed] [Google Scholar]
- 65.Griffeth RW, Hom PW, Gaertner S. A Meta-Analysis of Antecedents and Correlates of Employee Turnover: Update, Moderator Tests, and Research Implications for the next Millennium. J Manage. 2000;26(3):463–488. doi: 10.1177/014920630002600305. Available from: http://dx.doi.org/10.1177/014920630002600305. [DOI] [Google Scholar]
- 66.Hayes LJ, O’Brien-Pallas L, Duffield C, Shamian J, Buchan J, Hughes F, Spence Laschinger HK, North N, Stone PW. Nurse turnover: a literature review. Int J Nurs Stud. 2006 Feb;43(2):237–263. doi: 10.1016/j.ijnurstu.2005.02.007. Available from: http://dx.doi.org/10.1016/j.ijnurstu.2005.02.007. [DOI] [PubMed] [Google Scholar]
- 67.Needleman J, Kurtzman ET, Kizer KW. Performance measurement of nursing care: state of the science and the current consensus. Med Care Res Rev. 2007 Apr;64(2 Suppl):10S–43S. doi: 10.1177/1077558707299260. Available from: http://dx.doi.org/10.1177/1077558707299260. [DOI] [PubMed] [Google Scholar]
- 68.Dubois CA, D’Amour D, Pomey MP, Girard F, Brault I. Conceptualizing performance of nursing care as a prerequisite for better measurement: a systematic and interpretive review. BMC Nurs. 2013;12:7. doi: 10.1186/1472-6955-12-7. Available from: http://dx.doi.org/10.1186/1472-6955-12-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.O’Brien-Pallas L, Thomson D, McGillis Hall L, Pink G, Kerr M, Wang S, Li X, Meyer R. Evidence-based Standards for Measuring Nurse Staffing and Performance. Report for the Canadian Health Services Research Foundation. Ottawa: Canadian Health Services Research Foundation (CHSRF/FCRSS); 2004. Available from: http://fhs.mcmaster.ca/nru/documents/_VTI_CNF/Evidence%20Based%20Standards%20for%20Measuring%20Nurse%20Staffing%20and%20Performance.pdf. [Google Scholar]
- 70.Sochalski J. Is more better? The relationship between nurse staffing and the quality of nursing care in hospitals. Med Care. 2004 Feb;42(2 Suppl):II67–II73. doi: 10.1097/01.mlr.0000109127.76128.aa. [DOI] [PubMed] [Google Scholar]
- 71.Lucero RJ, Lake ET, Aiken LH. Nursing care quality and adverse events in US hospitals. J Clin Nurs. 2010 Aug;19(15-16):2185–2195. doi: 10.1111/j.1365-2702.2010.03250.x. Available from: http://dx.doi.org/10.1111/j.1365-2702.2010.03250.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Schubert M, Clarke SP, Glass TR, Schaffert-Witvliet B, De Geest S. Identifying thresholds for relationships between impacts of rationing of nursing care and nurse- and patient-reported outcomes in Swiss hospitals: a correlational study. Int J Nurs Stud. 2009 Jul;46(7):884–893. doi: 10.1016/j.ijnurstu.2008.10.008. Available from: http://dx.doi.org/10.1016/j.ijnurstu.2008.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Rochefort CM, Clarke SP. Nurses' work environments, care rationing, job outcomes, and quality of care on neonatal units. J Adv Nurs. 2010 Oct;66(10):2213–2224. doi: 10.1111/j.1365-2648.2010.05376.x. Available from: http://dx.doi.org/10.1111/j.1365-2648.2010.05376.x. [DOI] [PubMed] [Google Scholar]
- 74.Schubert M, Clarke SP, Aiken LH, de Geest S. Associations between rationing of nursing care and inpatient mortality in Swiss hospitals. Int J Qual Health Care. 2012 Jun;24(3):230–238. doi: 10.1093/intqhc/mzs009. Available from: http://dx.doi.org/10.1093/intqhc/mzs009. [DOI] [PubMed] [Google Scholar]
- 75.Kalisch BJ, Tschannen D, Lee KH. Missed nursing care, staffing, and patient falls. J Nurs Care Qual. 2012 Jan-Mar;27(1):6–12. doi: 10.1097/NCQ.0b013e318225aa23. Available from: http://dx.doi.org/10.1097/NCQ.0b013e318225aa23. [DOI] [PubMed] [Google Scholar]
- 76.Hall LM, Doran D. Nurse staffing, care delivery model, and patient care quality. J Nurs Care Qual. 2004 Jan-Mar;19(1):27–33. doi: 10.1097/00001786-200401000-00007. Available from: http://dx.doi.org/10.1097/00001786-200401000-00007. [DOI] [PubMed] [Google Scholar]
- 77.Nationaler Verein für Qualitätsentwicklung in Spitälern und Kliniken ANQ. Nationaler Messtag: Stürze und Wundliegen im Spital. ANQ; 2011. [cited 2013 Feb 5]. Available from: http://www.anq.ch/de/medien/medienmitteilung/nationaler-messtag-sturz-und-dekubitus/ [Google Scholar]
- 78.Halfens RJ, Meesterberends E, van Nie-Visser NC, Lohrmann C, Schönherr S, Meijers JM, Hahn S, Vangelooven C, Schols JM. International prevalence measurement of care problems: results. J Adv Nurs. 2013 Sep;69(9):e5–17. doi: 10.1111/jan.12189. Available from: http://dx.doi.org/10.1111/jan.12189. [DOI] [PubMed] [Google Scholar]
- 79.European Pressure Ulcer Advisory Panel EPUAP; National Pressure Ulcer Advisory Panel NPUAP. Prevention and treatment of pressure ulcers: quick reference guide. Washington DC: National Pressure Ulcer Advisory Panel; 2009. Available from: http://www.npuap.org/wp-content/uploads/2012/02/Final_Quick_Prevention_for_web_2010.pdf. [Google Scholar]
- 80.D’Amour D, Dubois CA, Tchouaket E, Clarke S, Blais R. The occurrence of adverse events potentially attributable to nursing care in medical units. Int J Nurs Stud. 2013 Oct 27;:S0020–7489(13)00325. doi: 10.1016/j.ijnurstu.2013.10.017. Available from: http://dx.doi.org/10.1016/j.ijnurstu.2013.10.017. [DOI] [PubMed] [Google Scholar]
- 81.Chaboyer W, Johnson J, Hardy L, Gehrke T, Panuwatwanich K. Transforming care strategies and nursing-sensitive patient outcomes. J Adv Nurs. 2010 May;66(5):1111–1119. doi: 10.1111/j.1365-2648.2010.05272.x. Available from: http://dx.doi.org/10.1111/j.1365-2648.2010.05272.x. [DOI] [PubMed] [Google Scholar]
- 82.Creswell JW. Research Design. Second ed. Thousand Oaks: Sage; 2003. [Google Scholar]
- 83.Martin JS, McCormack B, Fitzsimons D, Spirig R. Evaluation of a clinical leadership programme for nurse leaders. J Nurs Manag. 2012 Jan;20(1):72–80. doi: 10.1111/j.1365-2834.2011.01271.x. Available from: http://dx.doi.org/10.1111/j.1365-2834.2011.01271.x. [DOI] [PubMed] [Google Scholar]
- 84.Lamnek S. Gruppendiskussion. Weinheim: Beltz; 1998. [Google Scholar]
- 85.Pelz C, Schmitt A, Meis M. Knowledge Mapping als Methode zur Auswertung und Ergebnispräsentation von Fokusgruppen in der Markt- und Evaluationsforschung. Forum Qual Soc Res. 2004 May;5(2):35. Available from: http://nbn-resolving.de/urn:nbn:de:0114-fqs0402351. [Google Scholar]
- 86.Mayring P. Qualitative Inhaltsanalyse: Grundlagen und Techniken. Weinheim: Beltz Verlag; 2003. [Google Scholar]
- 87.Wendler MC. Triangulation using a meta-matrix. J Adv Nurs. 2001 Aug;35(4):521–525. doi: 10.1046/j.1365-2648.2001.01869.x. Available from: http://dx.doi.org/10.1046/j.1365-2648.2001.01869.x. [DOI] [PubMed] [Google Scholar]
- 88.O’Cathain A, Murphy E, Nicholl J. Three techniques for integrating data in mixed methods studies. BMJ. 2010;341:c4587. doi: 10.1136/bmj.c4587. Available from: http://dx.doi.org/10.1136/bmj.c4587. [DOI] [PubMed] [Google Scholar]
- 89.Kouzes JM, Posner BZ. The Leadership Practices Inventory: Theory and Evidence behind the five Practices of Exemplary Leaders. John Wiley & Sons; 2002. [cited 2010 Feb 21]. Available from: http://media.wiley.com/assets/463/74/lc_jb_appendix.pdf. [Google Scholar]
- 90.Brügger U, Bamert U, Maeder C, Odermatt R. Beschreibung der Methode LEP Nursing 2. Leistungserfassung für die Gesundheits- und Krankenpflege. St. Gallen: LEP AG; 2002. [Google Scholar]
- 91.Tilquin C. Équipe de Recherche Opérationnelle en Santé (EROS) — PRN 1987. Montréal: Bibliothèque Nationale du Québec et du Canada; 1988. [Google Scholar]
- 92.Corley MC, Minick P, Elswick RK, Jacobs M. Nurse moral distress and ethical work environment. Nurs Ethics. 2005 Jul;12(4):381–390. doi: 10.1191/0969733005ne809oa. Available from: http://dx.doi.org/10.1191/0969733005ne809oa. [DOI] [PubMed] [Google Scholar]
- 93.Aiken LH, Clarke SP, Sloane DM International Hospital Outcomes Research Consortium. Hospital staffing, organization, and quality of care: cross-national findings. Int J Qual Health Care. 2002 Feb;14(1):5–13. doi: 10.1093/intqhc/14.1.5. [DOI] [PubMed] [Google Scholar]
- 94.Schubert M, Glass TR, Clarke SP, Schaffert-Witvliet B, De Geest S. Validation of the Basel Extent of Rationing of Nursing Care instrument. Nurs Res. 2007 Nov-Dec;56(6):416–424. doi: 10.1097/01.NNR.0000299853.52429.62. [DOI] [PubMed] [Google Scholar]