

Abstract
Despite recent increases in life course research on mental illness, important questions remain about the social patterning of, and explanations for, depression trajectories among women in later life. The authors investigate competing theoretical frameworks for the age patterning of depressive symptoms and the physical health, socioeconomic, and family mechanisms differentiating black and white women. Using data from the National Longitudinal Survey of Mature Women, the authors use linear mixed (growth curve) models to estimate trajectories of distress for women aged 52 to 81 years (N = 3,182). The results demonstrate that: (1) there are persistently higher levels of depressive symptoms among black women relative to white women throughout later life; (2) physical health and socioeconomic status account for much of the racial gap in depressive symptoms; and (3) marital status moderates race differences in distress. The findings highlight the importance of physical health, family, and socioeconomic status in racial disparities in mental health.
Elevated rates of psychological distress among socially disadvantaged groups are perhaps the most enduring and observable consequences of social inequality in the United States (Mirowsky and Ross 2003). Women exhibit greater levels of depression than men (Gove 1978; Mirowsky 1996; Yang and Lee 2009), with symptoms of depression about twice as high among older women than older men (Penninx 2006). However, important questions remain regarding the influence of race on the life course patterning of depression among women (Gazmararian, James, and Lepkowski 1995;Skarupski et al. 2005; Williams, Costa, and Leavell 2010), particularly at older ages, when physical and mental health are strongly connected (Keith and Brown 2010;Penninx 2006). Do black women have persistently worse psychological health into later life? Or do black-white disparities in well-being increase or decrease as women transition to old age? How do physical health, socioeconomic status (SES), and family anchor and/or reinforce racial inequalities in women's mental health? Answers to these questions are fundamental to understanding how multiple systems of stratification—gender, age, and race—affect psychological health.
The processes that underlie potential racial differences in women's later life depression are not clear. However, physical health is a well-gdocumented correlate of mental health (Penninx 2006), and volumes of research on health disparities suggest two principal social mechanisms. First, SES is widely recognized as an important indicator of structural inequality and poor health (Evans-Campbell, Lincoln, and Takeuchi 2007; Williams, Costa, and Leavell 2010). Indeed, the unequal distribution of and returns to SES for women of different racial groups may explain some of the differences in depressive symptoms between black and white women (Williams, Costa, et al. 2010). Although race, gender, and SES fundamentally influence mental health (Keith and Brown 2010), the extent to which SES shapes black and white women's depressive symptoms at later ages is only beginning to be understood (Bromberger et al. 2004).
Another hypothesized mechanism is family status. Marital and parental roles expose women to a complex array of material resources, emotional demands, and various achievements and hardships that characterize the adult life course. Research suggests that marriage has greater benefits for whites than blacks (Williams, Frech, and Carlson 2010) and that family roles may be sources of greater stress for black women (Keith and Brown 2010). Moreover, it is well established that family formation, spousal and kin relationships, and their maintenance differ between white and black women (Fossett and Kielcolt 1993; Keith and Brown 2010; Williams, Frech et al. 2010). However, evidence of how family influences race differences in women's depression is less clear than the role of SES (Williams, Frech et al. 2010).
The dearth of research applying an integrated framework to examine these topics underscores the need for a comprehensive analysis of black-white differences in women's psychological distress in later life. Using more than three decades of panel data from the National Longitudinal Survey of Mature Women (NLS-MW), we investigate the extent to which theories of cumulative disadvantage, “multiple jeopardies,” and age as leveler offer new insights into how socioeconomic and familial factors affect race differences in age-related symptoms of depression. Unlike many studies that rely on cross-sectional designs to study depression (e.g., Kessler et al. 1992; Schieman, Van Gundy, and Taylor 2002), our study explicitly tests hypothesized changes in depressive symptoms across age and considers the effects of physical health, SES, and family on the racial patterning of depression among women in middle to older adulthood. We discuss our findings in the context of life course processes that are anchored to social statuses and structured inequalities.
Background
The literature focusing on age patterns of depression suggests that symptoms are elevated during adolescent years, followed by a stage of relatively low symptoms in early to late midlife, and then increase steadily into late life (Adkins et al. 2009;Kessler et al. 1992; Mirowsky and Ross 1992; Schieman et al. 2001; Yang 2007). However, this general pattern is largely based on cross-sectional studies or “snapshots” of the life course in younger samples. Theoretical and empirical developments aid and underscore the need for more detailed investigations of social group variation in depression trajectories and how the general age pattern of depression applies across genders and races.
Scholars have compared the mental health of black and white Americans for decades (Aneshensel, Clark, and Frerichs 1983; Blazer et al. 1998; Roxburgh 2009), with different conclusions common across measures of mental health (Evans-Campbell et al. 2007). Nevertheless, the findings generally show that whites have more favorable levels of psychological well-being than blacks (Cochran, Brown, and McGregor 1999;Comstock and Helsing 1976; George and Lynch 2003; Jones-Webb and Snowden 1993). Although rates of psychiatric disorders (including major depressive disorder) among whites tend to be higher than, or equal to, those among racial minorities (D. Williams et al. 2010), much of the evidence suggests that blacks have significantly higher levels of depressive symptoms than whites (e.g., Cochran et al. 1999; Gazmararian, James, and Lepkowski 1995; Skarupski et al. 2005; D. Williams et al. 2010).
Assuming a black disadvantage in depressive symptomatology across the life course in aggregate, it remains unclear which pattern best describes racial differences in depressive symptoms: divergence, convergence, or persistence (cf. Ferraro and Farmer 1996a). Two theoretically compatible perspectives suggest that trajectories of depression diverge with age: cumulative disadvantage and double jeopardy (Schieman and Plickert 2007). Cumulative disadvantage theory suggests that greater social and economic disadvantages that accumulate over time lead to worse health for black women relative to white women, who are less likely to experience commensurate adversities over the life course (Dannefer 2003). The consequences of these differences in disadvantage ultimately manifest as health disparities that widen with age (Schieman and Plickert 2007). According to the double jeopardy hypothesis (or potential “triple jeopardy” for women; Ferraro and Farmer 1996b), the detrimental effects of multiple disadvantaged statuses—being a minority and being older—may lead to an accelerated health decline among older black women relative to older white women (Ferraro and Farmer 1996b; Schieman and Plickert 2007). Despite the arguably intuitive appeal of the double jeopardy hypothesis for predicting health, empirical tests yield inconsistent support (Ferraro and Farmer 1996b; Schieman and Plickert 2007).
Alternatively, the “age as leveler” hypothesis predicts that trajectories of health converge in later life (Ferraro and Farmer 1996a; Kim and Durden 2007). According to this perspective, the relative social advantages of being white may become less consequential as all women face deteriorating physical health with age (Ferraro and Farmer 1996a). Although this perspective is mostly oriented toward explaining patterns of physical health due to mortality selection (Beckett 2000; Dupre 2007), age may also act as a leveling agent of racial inequalities in mental health (Xu et al. 2010). That is, as aging women experience changes in physical health and social status, racial disadvantage may become less salient. Moreover, poorer health and earlier death among black women could exclude the most depressed from observational studies of later life, potentially masking persistent or widening gaps in depression.
A recent longitudinal study of adults from midlife through older ages supports the age-as-leveler perspective by demonstrating diminishing inequalities in depression between blacks and whites across this age range (Xu et al. 2010). Moreover, the findings are statistically significant despite adjusting for SES (education and income), physical health, married status, and gender. The convergence of depressive symptoms may be anchored in the greater social stratification of women at younger ages that gradually attenuates in later life as major stressors (e.g., income, health care) are reduced through social programs for older adults. Indeed, Walsemann, Gee, and Geronimus (2009) demonstrate that black-white differences in levels of depression narrow in early midlife among relatively high SES women.
A third age-related pattern of depression can be characterized by persistent inequality. Ferraro and Farmer (1996a) demonstrate some divergent and convergent trajectories, depending on the measure of health, but persistent disadvantages in health best characterize racial differences across age among adults in the United States. That is, the black-white gap in health trajectories appears parallel throughout the later stages of life, suggesting that racial disadvantages may be deeply rooted by late life and immutable to the influence of changes in social statuses. Although support for persistent health inequality is largely based on physical health outcomes (Kelley-Moore and Ferraro 2004; Xu et al. 2010), similar patterns may be observed in mental health given the well-documented association between physical and mental health.
Recognizing the inconsistencies in existing research, we draw from recent and relevant evidence on depressive symptoms (Walsemann et al. 2009; Xu et al. 2010) to hypothesize that black-white differences in women's trajectories of depressive symptoms will converge at later ages (hypothesis 1). However, we also consider the potential for persistent or convergent trajectories of depression. We anticipate that adjustments for racial differences in physical health, socioeconomic resources, and family formation will alter the patterning of women's depression across age, as described below.
Explanations for Black-White Disparities in Depression Trajectories
Physical health
Correlations between physical health and psychological well-being are routinely documented: Poor physical health increases levels of depression in older adults (e.g., Schnittker 2005). Among women, studies demonstrate important race differences that have been theoretically described according to the “weathering hypothesis” (Geronimus 1996, 2001). This hypothesis posits that black women experience worsening health earlier in life than white women because of greater social disadvantages and discrimination, with implications observed in adverse birth outcomes (Geronimus 1996), later life physical disability (Taylor 2008), and higher mortality risk (Spence and Eberstein 2009). Considering the depressive effects of poor health (Schnittker 2005) and recent evidence of the effect of physical health (i.e., functional status) on race differences in distress (Xu et al. 2010), we hypothesize that physical health will reduce black-white differences in depression trajectories (hypothesis 2).
Socioeconomic status (SES)
Social scientists have long debated the extent to which racial disparities in health are a reflection of socioeconomic inequalities (e.g., Evans-Campbell et al. 2007; Kessler and Neighbors 1986). Accordingly, recent evidence suggests that black-white differences in depressive symptoms may be substantially accounted for by SES inequalities (Williams, Costa, et al. 2010). In some studies, SES-adjusted estimates suggest converging or inverting levels of depression between blacks and whites (Bratter and Eschbach 2005). Moreover, socioeconomic factors appear to moderate racial differences in mental health (Gazmararian et al. 1995; George and Lynch 2003;Kessler and Neighbors 1986), with a demonstrated nonequivalence of SES across race groups that influences racial differences in health outcomes (Williams, Costa, et al. 2010).
Disadvantages associated with race lead to lower educational attainment, income, and wealth accumulation, with potential consequences including inadequate coping resources to ameliorate stress and reduce depressive symptoms (Keith and Brown 2010). Still, evidence suggests that SES may be less important for later life health disparities. For example, longitudinal evidence shows that the magnitude of the racial gap in older adults remains statistically significant (Skarupski et al. 2005; Xu et al. 2010), suggesting that race differences are not strictly a function of SES. Therefore, we hypothesize that SES will explain a substantial portion of the black-white difference in women's trajectories of depressive symptoms (hypothesis 3a).
Research also suggests that SES may operate as a moderator of the relationship between race and mental health (George and Lynch 2003; Kessler and Neighbors 1986). This may be related to unequal returns from commensurate levels of education (Keith and Brown 2010; Kessler and Neighbors 1986; Williams, Costa, et al. 2010) or differential exposure to stress (George and Lynch 2003). Low-income blacks appear to exhibit more distress than their white counterparts (Kessler and Neighbors 1986). However, Walsemann et al. (2009) suggest that racial differences in depression are reduced during early midlife among whites and blacks with more than a high school education and $24,000 or more in family income. Results for women are less clear, although nonpoor black women appear to report more depressive symptoms than nonpoor white women (Gazmararian et al. 1995). Drawing on these studies, we hypothesize that the black disadvantage in depression will be greater among low-SES women and less among women with higher SES (hypothesis 3b).
Family status
Scholars are moving beyond the prevailing emphasis on SES as an explanation for racial inequalities in mental health (Evans-Campbell et al. 2007) and focusing greater attention on the influence of women's family status (Keith and Brown 2010). Family connections can be instrumental and emotional sources of support that are protective of mental health (Gazmararian et al. 1995). Marital and parental statuses may also structure racial inequalities in life course exposures to opportunities and hardship, represent sources of stress, or provide psychological armament to cope with adversity throughout adulthood.
Evidence bears that married people report better mental health than their unmarried counterparts (Hughes and Waite 2009); however, there is a need for more comprehensive investigations of marital status differences (Williams, Frech, et al. 2010). Blacks are more likely to be never or previously married than whites (Bramlett and Mosher 2002), and the mental health benefits of marriage appear to be strongest among whites (Williams, Frech, et al. 2010). Thus, marital status variability may account for black-white differences in distress at older ages. Although never-married black women do not appear to differ in psychological health from married black women (Jackson 1997; Williams, Takeuchi, and Adair 1992), previously married black women exhibit higher rates of psychiatric disorders than married black women (Williams et al. 1992). White women who never married or are separated or divorced appear psychologically worse than their married peers (Williams et al. 1992). However, comparisons across race by marital status categories are less clear. Some suggest that black women adapt to marital dissolution better than their white counterparts (McKelvey and McKenry 2000), with widowed white women demonstrating higher rates of depression than widowed black women (Jones-Webb and Snowden 1993). Being unmarried may be less problematic among black women, given lower rates of marriage in this population (Bramlett and Mosher 2002) and increased likelihood of developing coping mechanisms by midlife (Marks and Lambert 1998). On the other hand, the benefits of marriage may be less pronounced for black women than for white women because they are more likely to be employed while bearing the burden of domestic labor (Keith and Brown 2010).
Parenthood may also differentially influence black and white women's well-being throughout the life course (Umberson, Pudrovska, and Reczek 2010). Although parenthood is a respected and valued social role (Koropeckyj-Cox, Pienta, and Brown 2007), the psychological benefits of having children often may not manifest until older ages, when child-rearing burdens are reduced (Evenson and Simon 2005). Childbearing histories (including childlessness, high parity, and early childbearing) can have important implications for psychological well-being throughout life (Evenson and Simon 2005; Spence 2008; Sudha et al. 2006; Umberson et al. 2010). However, little is known about how childbearing histories may affect black-white differences in women's later life well-being. Motherhood may have lasting consequences in the forms of financial deficiencies, poor social relationships and marital challenges, and physical weathering that are most apparent at the intersection of race and gender, particularly given the different patterns of family formation.
Racial differentiation in childbearing histories is well documented (Burton 1990; Keith and Brown 2010), and parental status may differentially affect black and white women's health. A community-based study of older women finds childlessness associated with lower levels of depressive symptoms for blacks but not whites (Sudha et al. 2006), implying a moderating effect of childlessness. Although race differences are not examined, Mirowsky and Ross (2002) showed that the relationship between childlessness and depression is contingent on age at first birth, with women having children early and late more depressed than childless women. Significantly higher rates of depression are found among adolescent mothers: Young black mothers report more depression than their white counterparts (Deal and Holt 1998). Others find limited evidence for the role of early childbearing on psychological well-being (Koropeckyj-Cox et al. 2007; Spence 2008). Late childbearing (i.e., after about age 35), on the other hand, may have an independent effect on late-life depression (Koropeckyj-Cox et al. 2007; Spence 2008), but additional research is needed to understand the extent to which this may shape black-white differences in well-being. Another potentially important family-related factor in race differences in mental health is the number of children, given higher parity among black women and its role in well-being (Grundy and Holt 2000). Overall, existing evidence implicates childbearing histories as an element of family status important for psychological health throughout the life course.
Over the life course, the relevance and influence of childbearing histories for psychological well-being likely varies as women age and experience role changes. Moreover, parental roles may matter less for the well-being of black women because of their greater social integration beyond the immediate family (e.g., in their community and church) in middle age and older adulthood (Coleman et al. 1987). Research addressing the weathering hypothesis also suggests that early childbearing may have fewer negative consequences for black women's health relative to white women (Spence and Eberstein 2009). Thus, the influence of family on later life well-being may be more relevant for older white women than for older black women.
Collectively, research on family status suggests that marriage and childbearing—particularly disadvantages associated with separation or divorce, widowhood, and aspects of childbearing histories—may mediate and/or moderate the impact of race on later life depression. On the basis of existing evidence, we hypothesize that family status will mediate black-white differences in depressive symptoms across age (hypothesis 4a). To the extent that particular marital statuses and childbearing histories affect black women more than white women, controlling for these factors should reduce the observed black disadvantage in depressive symptoms. Finally, family status is hypothesized to moderate racial differences in trajectories of depression (hypothesis 4b). Although existing evidence offers little guidance for the pattern of moderation, race differences in family formation and the impact of family status on well-being suggest that black and white women may be distinctly influenced by being unmarried, remaining childless, experiencing high parity, and/or having children early or late in life.
Data and Methods
Data and Sample
We use nationally representative data from the NLS-MW, a multistage probability sample of civilian, noninstitutionalized women aged 30 to 44 years in 1967, with an oversampling of black women (Center for Human Resource Research 2001). The NLS-MW surveyed 5,083 women at the baseline interview. The NLS-MW cohort was interviewed 20 times from 1967 to 2003. Sample attrition through 2003 was attributed primarily to respondent death (N = 1,485) and refusals (N = 1,036); respondents lost to follow-up (N = 325) made up the remainder.
The NLS-MW is among the longest running studies of American women and is well–suited for the study of health in later life. A key advantage of the survey is the collection of panel data over more than 35 years, spanning important stages of the life course. In 1989, the NLS-MW supplemented its rich measures of SES and family characteristics with measures of health, including depressive symptoms. The NLS-MW data on women born in the 1920s and 1930s reduces the confounding effects of cohort differences on age effects shown in recent research (Yang 2007; Yang and Lee 2009). The long-term panel design and the detailed collection of key measures provides a unique opportunity to study the hypothesized changes in depressive symptoms among aging women.
Measures
The dependent variable in the analyses is depressive symptoms. An abbreviated seven-item version of the Center for Epidemiologic Studies Depression Scale (Radloff 1977) is available in six waves of the NLS-MW (1989 through 2003), when women were aged 52 to 81 years. Respondents were asked the frequency in the past week with which they felt: (1) unable to shake the blues; (2) trouble keeping their minds on tasks; (3) that everything took extra effort; (4) restless sleep; (5) lonely; (6) sad; and (7) that they could not get going. Summed responses range from 0 to 21; where 0 =no symptoms of depression. Scale reliability (α) across years ranges from .82 to .84.
Race is ascertained from self-identification as black (coded 1) or white (coded 0). We include three dichotomous variables (1922 to 1927 [reference], 1928 to 1932, and 1933 to 1937) to model the influence of birth cohort differences in the age-based analyses. We measure physical health using a continuous, time-varying index (mean centered) of the degree of difficulty (1) walking one block; (2) using stairs or inclines; (3) reaching; (4) sitting for long periods; (5) stooping, kneeling, and crouching; (6) lifting and carrying heavy weights; and (7) fingering or grasping.
SES is measured as educational attainment, income, and home ownership. Educational attainment is measured with dichotomous variables representing: (1) less than high school; (2) some high school but no diploma; and (3) high school graduate or higher (reference group). Family income is time varying, measured in thousands of dollars (logged and mean centered). A dichotomous variable for no home ownership (coded 1) is included as a time-varying proxy for assets.
Family status is measured using indicators of marital status, the number of children, and the timing of birth. Marital status is measured using time-varying dichotomous variables: (1) never married; (2) married (reference group); (3) divorced or separated; or (4) widowed at each assessment. A dichotomous measure of childlessness is derived from fertility histories collected when the women were age 45 to 59 years. High parity is a dichotomous measure indicating whether the respondent gave birth to four or more children (yes = 1). Another dichotomous measure indicates whether the respondent had her first child as a teenager (coded 1) compared with initiating childbearing after age 19. Women whose last birth was later than age 35 (coded 1) were categorized as having late births.
Analytic Strategy
Linear mixed models are used to analyze depressive symptoms across age (Bryk and Raudenbush 1992; Goldstein 1995). The advantages of mixed models for the analysis of longitudinal data processes of change are well described elsewhere (see Bryk and Raudenbush 1992; Goldstein 1995; Willett, Singer, and Martin 1998). Here, mixed models allow the investigation of how women's depressive symptoms vary with age, account for the dependency of repeated observations, and accommodate unbalanced panel data, such as the NLS-MW.
Our analyses begin by modeling the unconditional growth curve for depressive symptoms in the full sample of women. Comparisons of linear, quadratic, and cubic functional forms indicated that the average trajectory is characterized by a U-shaped pattern of decreasing symptoms followed by increasing symptoms in old age. The unconditional trajectory is modeled as a quadratic function of age defined by a random intercept and linear and quadratic slope components written as follows:
| (1) |
| (2) |
| (3) |
In the level 1 model, for woman i at time t, y ti is the Center for Epidemiologic Studies Depression Scale score, Ageti is the age with the trajectory intercept specified at 52 years (the youngest age); Age2 ti is the squared age, and e ti is the within-individual residual. For woman i, π0i is the intercept of the growth trajectory, π1i is the linear component of the slope of the trajectory, and π2i is the quadratic component of the slope of the trajectory. In the level 2 model, β00 is the mean (or fixed) intercept of the age trajectory, β10 is the mean linear component of the slope of the age trajectory, and β20 is the mean quadratic component of the slope of the age trajectory. For woman i, r 0i is the random effect of the intercept term, r 1i is the random effect of the linear component of the slope, and r 2i is the random effect of the linear component of the slope. The combined model expresses the observed repeated measures of depressive symptoms as an additive combination of a fixed and random growth component.
Analyses were conducted in Stata version 11, using multiple imputation with mixed models using the EM algorithm for maximum likelihood estimation as described by Pinheiro and Bates (2000). Consistent with existing evidence that mixed models generally have desirable properties for analyzing longitudinal data with attrition (Twisk 2004; Twisk and de Vente 2002), sensitivity analyses demonstrated no substantive differences from the results presented when using data for (1) nonattriting subjects only and (2) individuals who attrite from the sample before the last observation.
Results
Descriptive Results
Figure 1 illustrates mean depressive symptoms by age and race. The figure shows that black women consistently report higher levels of depressive symptoms than white women from middle to late life. The racial disparity in symptoms generally appears smallest at the oldest ages, with decreasing depression among black women during midlife and increasing levels of depression among white women after about age 70. However, these trends should be interpreted cautiously given small sample sizes at the two ends of the age range.
Figure 1. Average Depressive Symptoms by Age and Race.
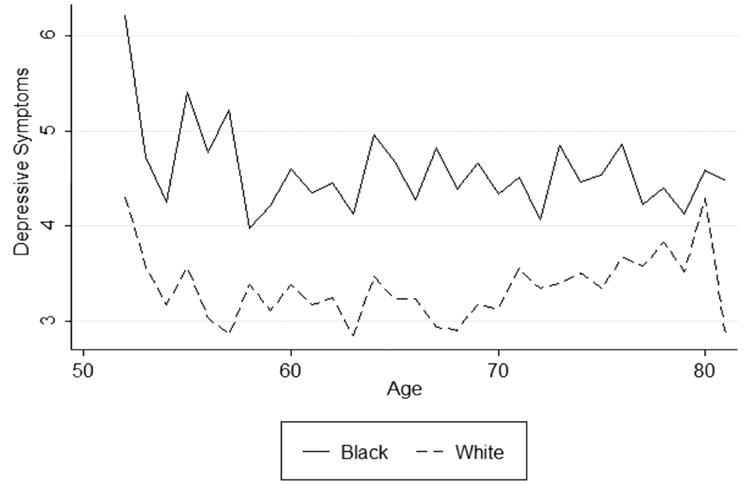
Table 1 presents descriptive statistics for the repeated observations of all predictors separately for black and white women prior to multiple imputation. Descriptive statistics estimated from multiple imputation (not shown) do not substantively differ from those in Table 1. Distributionally, black and white women differ significantly on all variables at the .05 level, with the exception of birth cohort (1933 to 1937). Blacks report more than one additional physically limited activity than whites. Notable differences are also apparent in SES indicators, with black women disadvantaged relative to white women. Marriage is approximately twice as high among white women, whereas divorce is twice as high among black women. Black women are more often never married or widowed, have lower rates of childlessness, have more early first and late last births, and have higher parity than white women.
Table 1. Descriptive Statistics for the Independent Variables in the NLS-MW.
| Predictors | White | Black | ||||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||
| M | SD | Range | Observations | M | SD | Range | Observations | |
| Age | 67.50 | 6.33 | 52 to 81 | 10,782 | 67.23 | 6.22 | 52 to 81 | 3,629 |
| Birth cohort | ||||||||
| 1922 to 1927 | .38 | .49 | 0 to 1 | 10,782 | .34 | .47 | 0 to 1 | 3,629 |
| 1923 to 1932 | .33 | .47 | 0 to 1 | 10,782 | .37 | .48 | 0 to 1 | 3,629 |
| 1933 to 1937 | .30 | .46 | 0 to 1 | 10,782 | .29 | .46 | 0 to 1 | 3,629 |
| Physical limitations | 3.05 | 3.50 | 0 to 21 | 10,763 | 4.43 | 4.06 | 0 to 21 | 3,625 |
| SES | ||||||||
| Less than high school | 1.1 | .31 | 0 to 1 | 10,754 | .36 | .48 | 0 to 1 | 3,624 |
| Some high school | .17 | .38 | 0 to 1 | 10,754 | .33 | .47 | 0 to 1 | 3,624 |
| High school graduate or higher | .72 | .50 | 0 to 1 | 10,754 | .31 | .42 | 0 to 1 | 3,624 |
| Income ($) | 21,341 | 17,371 | 0 to 194,897 | 10,681 | 12,031 | 12,258 | 0 to 151,007 | 3,563 |
| Not homeowner | .16 | .36 | 0 to 1 | 10,767 | .34 | .48 | 0 to 1 | 3,623 |
| Family status | ||||||||
| Never married | .03 | .18 | 0 to 1 | 10,708 | .07 | .25 | 0 to 1 | 3,606 |
| Married | .60 | .49 | 0 to 1 | 10,708 | .30 | .46 | 0 to 1 | 3,606 |
| Divorced | .11 | .31 | 0 to 1 | 10,708 | .22 | .41 | 0 to 1 | 3,606 |
| Widowed | .26 | .44 | 0 to 1 | 10,708 | .41 | .49 | 0 to 1 | 3,606 |
| Childless | .09 | .29 | 0 to 1 | 10,711 | .08 | .27 | 0 to 1 | 3,596 |
| High parity (four or more children) | .37 | .48 | 0 to 1 | 10,782 | .60 | .49 | 0 to 1 | 3,629 |
| Teenage first birth | .21 | .40 | 0 to 1 | 10,698 | .51 | .50 | 0 to 1 | 3,595 |
| Last birth age 35 or older | .21 | .40 | 0 to 1 | 10,698 | .30 | .46 | 0 to 1 | 3.595 |
Note; NLS-MW = National Longitudinal Survey of Mature Women; SES = socioeconomic status. SD = standard deviation. Distributions are based on nonimputed repeated observations of NLS-MW respondents. All black-white differences are significant at p < .05, except birth cohort 1933 to 1937.
Model 3 includes the time-varying measure of physical health to test hypothesis 2. The results show that physical health reduces black-white differences in depression. Panel 2 of Figure 2 further shows declining levels of depressive symptoms throughout later life net of physical health. Although race differences narrow, they remains statistically significant. Given the important correlation between physical and mental health, physical health is included in models examining the roles of SES and family on black-white differences.
Figure 2. Effects of Physical Limitations and Socioeconomic Status on Black-White Trajectories of Depressive Symptoms.
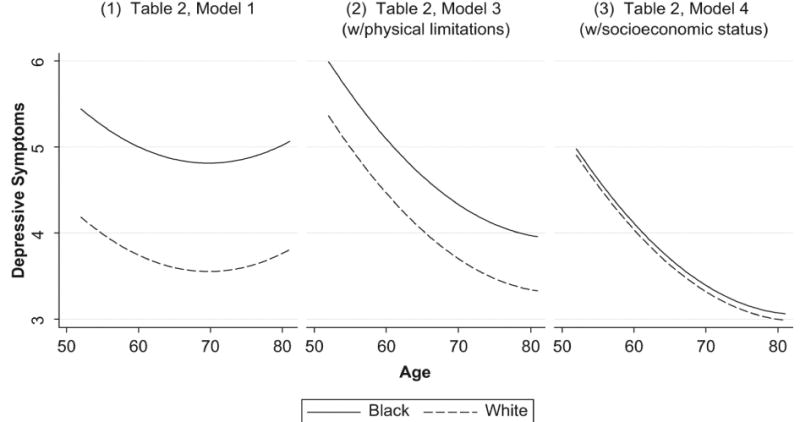
Models 4 to 6 in Table 2 test mediating effects of SES and family (hypotheses 3a and 4a, respectively), and model 7 shows a full model. Model 4 adds educational attainment, income, and home ownership. All SES indicators independently predict depressive symptom trajectories, with socioeconomic disadvantage associated with increased levels of symptoms. Furthermore, the black-white difference in trajectories of depression is statistically eliminated by SES (see panel 3 of Figure 2). A formal test of attenuation indicates a significant reduction (p < .01) in the race coefficient, lending support to hypothesis 3a. Models 5 and 6 examine the influence of marital status and childbearing histories, respectively. Being formerly married is independently and negatively associated with depression relative to being married, and having children early and late during the reproductive years increases depression. However, black-white differences remain significant. Model 7 demonstrates a full attenuation of the black disadvantage in depressive symptoms when controlling for SES and family.
Table 2. Health, SES, and Family Influences on Trajectories of Depressive Symptoms in Women Aged 52 to 80 Years (N = 14,411).
| Variable | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 |
|---|---|---|---|---|---|---|---|
| Agea | −.071** | −.081*** | −.128*** | −.124*** | −.137*** | −.126*** | −.132*** |
| Age2 | .002** | .003*** | .002** | .002** | .002* | .002** | .002** |
| Birth cohort (reference: 1923 to 1927) | |||||||
| 1928 to 1932 | −.426** | −.427** | −.457*** | −.345** | −.434*** | −.486*** | −.338** |
| 1933 to 1937 | −.602*** | −.601*** | −.760*** | −.620*** | −.719*** | −.753*** | −.566*** |
| Black (reference: white) | 1.258*** | 1.057** | .630*** | .073 | .425*** | .484*** | −.051 |
| Black × Age | .041 | ||||||
| Black × Age2 | −.002 | ||||||
| Physical limitations | .438*** | .420*** | .434*** | .435*** | .418*** | ||
| SES | |||||||
| Less than high school (reference: high school or more) | 1.421*** | 1.362*** | |||||
| Some high school (reference: high school or more) | .821*** | .795*** | |||||
| Income | −.070** | −.044 | |||||
| No home ownership | .305** | .199* | |||||
| Family status | |||||||
| Never married (reference: married) | .206 | .336 | |||||
| Divorced (reference: married) | .553*** | .470** | |||||
| Widowed (reference: married) | .902*** | .777*** | |||||
| Childless | −.200 | −.375 | |||||
| High parity (four or more children) | −.064 | −.151 | |||||
| Teenage first birth | .434*** | −.004 | |||||
| Last birth age 35 or older | .271* | .220 | |||||
| Intercept | 4.182*** | 4.230*** | 5.358*** | 4.902*** | 5.206*** | 5.245*** | 4.825*** |
| Random age SD | .056** | .056** | .000 | .000 | .000 | .000 | .000 |
| Random age2 | .002** | .002** | .001** | .002** | .001** | .001** | .002** |
| Random intercept SD | 2.757*** | 2.758*** | 2.210*** | 2.137*** | 2.186*** | 2.201*** | 2.124*** |
| Residual SD | 3.039*** | 3.039*** | 3.004*** | 2.999*** | 2.995*** | 3.003*** | 2.991*** |
Note: SES = socioeconomic status.
Age = actual age − 52 years.
p < .05.
p < .01.
p < .001 (two−tailed tests).
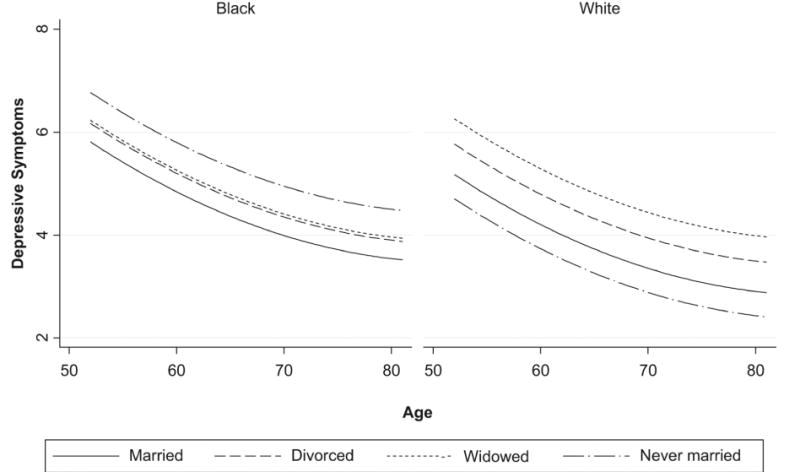
Table 3 tests race by SES and family status interactions (hypotheses 3b and 4b). Model 1 shows no evidence to support the moderating role of SES on racial differences in depressive symptoms (hypothesis 3b). Model 2 tests the moderating effects of marital status on race and shows significant interactions between race and marital status, lending partial support to hypothesis 4b. The interactions between race and marital status are illustrated in Figure 3. Among widows, blacks have lower levels of depressive symptoms than whites, whereas never-married whites have lower levels of depressive symptoms than never-married blacks. The effects of parental status characteristics do not differ significantly by race (model 3).
Table 3. Moderating Influences of SES and Family Status on Trajectories of Depressive Symptoms in Women Aged 52 to 81 Years (N = 14,411).
| Variable | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Age | −.125*** | −.137*** | −.126*** |
| Age2 | .002** | .002** | .002** |
| Birth cohort (reference: 1923 to 1927) | |||
| 1928 to 1932 | −.360** | −.410** | −.437*** |
| 1933 to 1937 | −.630*** | −.724*** | −.747*** |
| Black | .089 | .636*** | .460* |
| Physical limitations | .420*** | .434*** | .434*** |
| SES | |||
| Less than high school (reference: high school or more) | 1.534*** | ||
| Some high school (reference: high school or more) | .711*** | ||
| Income | −.072* | ||
| No home ownership | .341** | ||
| Family status | |||
| Never married (reference: married) | −.469 | ||
| Divorced (reference: married) | .591*** | ||
| Widowed (reference: married) | 1.086*** | ||
| Childless | −.262 | ||
| High parity (four or more children) | −.101 | ||
| Teenage first birth | .527*** | ||
| Last birth age 35 or older | .258 | ||
| Moderating effects | |||
| Black × Less Than High School | −.206 | ||
| Black × Some High School | .285 | ||
| Black × Income | −.009 | ||
| Black × No Home Ownership | −.122 | ||
| Black × Never Married | 1.429** | ||
| Black × Divorced | −.231 | ||
| Black × Widowed | −.665** | ||
| Black × Childless | .257 | ||
| Black × High Parity | .201 | ||
| Black × Teenage Birth | −.296 | ||
| Black × Late Birth | .044 | ||
| Intercept | 4.924*** | 5.171*** | 5.246*** |
| Random age SD | .000 | .000 | .000 |
| Random age2 | .002** | .001** | .001** |
| Random intercept SD | 2.136*** | 2.176*** | 2.203*** |
| Residual SD | 3.005*** | 2.994*** | 3.008*** |
Note: SES = socioeconomic status.
p < .05.
p < .01.
p < .001 (two−tailed tests).
Figure 3. Moderating Effects of Marital Status on Black-White Trajectories of Depressive Symptoms.
Discussion
Race and age shape health and happiness directly and indirectly through systems of stratification that influence later life statuses. Using more than three decades of panel data, we investigate the impacts of physical health, SES, and family on black-white differences in psychological well-being among women from midlife to older adulthood. The results demonstrated a clear age patterning of depression and mixed evidence for the effects of physical health, SES, and family on racial differences in the trajectories of depression.
Our findings do not support hypothesis 1, that black-white differences in depression converge at later ages of the life course. Rather, we find that black women exhibit persistently higher levels of depressive symptoms than white women. Despite recent attention to the cumulative disadvantage and age-as-leveler hypotheses to describe respective divergence and convergence in health inequalities, our results are more compatible with prior research on the persistence of physical health inequalities among older adults (e.g. Ferraro and Farmer 1996a). That is, the process of aging does not appear to aggravate or ameliorate racial disadvantages in well-being among women in the United States.
Three theoretically important mechanisms were evaluated. First, we investigated the role of physical health in accounting for psychological well-being. Next, we examined SES to (1) account for the well-established relationship between SES and health and (2) assess the impact of differences in SES among racial groups. Our findings support hypothesis 3a, that black-white differences in depressive symptoms can be largely attributed to SES, as previously shown (Xu et al. 2010). Moreover, although blacks and whites may differentially benefit from socioeconomic achievements, we found no evidence of moderating relationships between race and SES when predicting women's depressive symptoms from middle to later life (hypothesis 3b). This finding differs from previous studies showing differential effects of race within SES groups (Gazmararian et al. 1995; Jones-Webb and Snowden 1993; Kessler and Neighbors 1986; Walsemann et al. 2009). Indeed, the nonequivalence of SES among black and white women may matter more during earlier stages of the life course and less in later life.
The third set of hypotheses considered family status as a potential mechanism producing black-white differences in trajectories of distress. Culturally and historically based patterns of family formation distinguish black and white women's experiences. Variations in the life course patterning of these factors were hypothesized to elucidate an important pathway into race disparities in health. We tested the mediating and moderating effects of family status on the race-distress relationship and found mixed results. Although we found limited support for the hypothesis that family acts as a mediator (hypothesis 4a), marital status moderated the effect of race on women's trajectories of depressive symptoms from midlife to older ages (hypothesis 4b). Specifically, we demonstrated elevated levels of depression among widowed white women and never-married black women. Our findings are concordant with earlier research showing increased depression among widowed white women (Jones-Webb and Snowden 1993). However, the results presented here differ from those suggesting that black women who never marry are not disadvantaged in health (Jackson 1997;Williams et al. 1992). Williams et al. (1992) showed higher risk for psychiatric disorders associated with being widowed for black women and of being never married for white women. More apparent differences across marital status categories for white women suggest that marital status may differentiate levels of depression more among white women than black women. More research is needed to clarify the unexpected findings for never-married women and to understand why widowhood differentiates the psychological well-being of white women in light of evidence that the effects of widowhood on mental health do not vary by race (Carr 2004).
Our findings should be interpreted within the context of the study's strengths and limitations. We provide longitudinal evidence of race disparities in psychological distress in the later decades of life using nationally representative data. Previous research on black-white differences in depressive symptoms among older adults often draws on regional samples (e.g., Skarupski et al. 2005) or samples of adults younger than 70 years old (e.g., Gazmararian et al. 1995; Jones-Webb and Snowden 1993;Walsemann et al. 2009; for an exception, see Xu et al. 2010). The aging U.S. population, particularly the feminization of old age, underscores the need for understanding women's experiences from middle ages into older adulthood. It is important to note, however, that our measurement of depression begins at midlife; therefore, we acknowledge that selective mortality could influence the observed patterns of racial disparities.
In this study, we consider physical health, SES, and family as potential mechanisms of black-white differences in distress. The results highlight the importance of all three for racial disparities in mental health and a need for additional research to understand the reasons for the moderating effects of marital status. Information on relationship quality, perceptions of social support from family and other sources (e.g., religious groups), and the burdens associated with caregiving may help further explain the effects of family status on distress. Moreover, the weathering hypothesis suggests that differences in stress exposure and physiological stress response may distinguish older black and white women in well-being (Geronimus 2001). Elucidating the fundamental causes of racial disparities in health and well-being presents major challenges for researchers but is imperative for progress toward social equality.
Acknowledgments
We would like to thank Andrew M. Cislo and Mathew Gayman for helpful suggestions on earlier versions of this article. An earlier draft of this article was presented at the 2010 annual meeting of the American Sociological Association.
This study was supported in part by National Institute of Mental Health grant K01MH093731 awarded to Daniel E. Adkins.
Biographies
Naomi J. Spence is an assistant professor of sociology at Lehman College, City University of New York. Her research focuses on intersections of race-ethnicity, family, and health. Her work has examined these relationships across the life course. Her recent studies are investigating social group differentials in family formation among contemporary cohorts to clarify the antecedents of the family-health relationship.
Daniel E. Adkins is an assistant professor at the Center for Biomarker Research and Personalized Medicine of Virginia Commonwealth University. His research interests include statistical modeling, developmental psychopathology and gene-environment interaction in psychiatric disorders. His research has recently been published in Molecular Psychiatry, Development and Psychopathology, Social Forces and Sociological Theory and is supported by the National Institute of Mental Health.
Matthew E. Dupre is a research associate at the Duke Clinical Research Institute at Duke University Medical Center and senior fellow at Duke's Center for the Study of Aging and Human Development. His research broadly centers on the social determinants of adult health and well being. His recent studies use a life course perspective and interdisciplinary methods to study how cumulative processes of disadvantage shape inequalities in aging.
References
- Adkins Daniel E, Wang Victor, Dupre Matthew E, van den Oord Edwin JGC, Elder Glen H., Jr Structure and Stress: Trajectories of Depressive Symptoms across Adolescence and Young Adulthood. Social Forces. 2009;88(1):39–60. doi: 10.1353/sof.0.0238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aneshensel Carol S, Clark Virginia A, Frerichs Ralph R. Race, Ethnicity, and Depression: A Confirmatory Analysis. Journal of Personality and Social Psychology. 1983;44(2):385–398. doi: 10.1037//0022-3514.44.2.385. [DOI] [PubMed] [Google Scholar]
- Beckett Megan. Converging Health Inequalities in Later Life—an Artifact of Mortality Selection? Journal of Health and Social Behavior. 2000;41:106–119. [PubMed] [Google Scholar]
- Blazer Dan G, Landerman LR, Hays JC, Simonsick EM, Saunders WB. Symptoms of Depression among Community-Dwelling Elderly African-American and White Older Adults. Psychological Medicine. 1998;28(6):1311–1320. doi: 10.1017/s0033291798007648. [DOI] [PubMed] [Google Scholar]
- Bramlett Matthew D, Mosher William D, MD National Center for Health Statistics. Cohabitation, Marriage, Divorce, and Remarriage in the United States. (23).Vital and Health Statistics. (no. 22) [PubMed] [Google Scholar]
- Bratter Jenifer L, Karl Eschbach. Race/Ethnic Differences in Nonspecific Psychological Distress: Evidence from the National Health Interview Survey. Social Science Quarterly. 2005;86(3):620–644. [Google Scholar]
- Bromberger Joyce T, Harlow Sioban, Avis Nancy, Kravitz Howard M, Cordal Adriana. Race/Ethnic Differences in the Prevalence of Depressive Symptoms Among Middle-Aged Women: The Study of Women's Health Across the Nation (SWAN) American Journal of Public Health. 2004;94(8):1378–1385. doi: 10.2105/ajph.94.8.1378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bryk Anthony S, Raudenbush Stephen W. Hierarchical linear models: Applications and data analysis methods Advanced qualitative techniques in the social sciences. xvi. Thousand Oaks, CA, US: Sage Publications, Inc.; 1992. p. 265. [Google Scholar]
- Burton Linda M. Teenage Childbearing as an Alternative Life-Course Strategy in Multigeneration Black Families. Human Nature. 1990;1(2):123–143. doi: 10.1007/BF02692149. [DOI] [PubMed] [Google Scholar]
- Center for Human Resource Research. National longitudinal surveys mature women user's guide. Columbus, OH: The Ohio State University; 2001. [Accessed 23.05.08]. Available from: http://www.bls.gov/nls/mwguide/2001/nlsmwg0.pdf. [Google Scholar]
- Cochran Donna L, Brown Diane R, Mcgregor Karl C. Racial Differences in the Multiple Social Roles of Older Women: Implications for Depressive Symptoms. The Gerontologist. 1999;39(4):465–472. doi: 10.1093/geront/39.4.465. [DOI] [PubMed] [Google Scholar]
- Coleman Lerita M, Antonucci Toni C, Adelmann Pamela K, Crohan Susan E. Social Roles in the Lives of Middle-Aged and Older Black Women. Journal of Marriage and the Family. 1987;49(4):761. [Google Scholar]
- Comstock George W, Helsing Knud J. Symptoms of Depression in Two Communities. Psychological Medicine. 1976;6(4):551–563. doi: 10.1017/s0033291700018171. [DOI] [PubMed] [Google Scholar]
- Dannefer Dale. Cumulative Advantage/Disadvantage and the Life Course: Cross-Fertilizing Age and Social Science Theory. The Journals of Gerontology: Series B. 2003;58(6):S327–S337. doi: 10.1093/geronb/58.6.s327. [DOI] [PubMed] [Google Scholar]
- Deal Lisa W, Holt Victoria L. Young Maternal Age and Depressive Symptoms: Results from the 1988 National Maternal and Infant Health Survey. American Journal of Public Health. 1998;88(2):266–270. doi: 10.2105/ajph.88.2.266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dupre Matthew E. Educational Differences in Age-Related Patterns of Disease: Reconsidering the Cumulative Disadvantage and Age-As-Leveler Hypotheses. Journal of Health and Social Behavior. 2007;48(1):1–15. doi: 10.1177/002214650704800101. [DOI] [PubMed] [Google Scholar]
- Evans-Campbell Teresa, Lincoln Karen D, Takeuchi David T. Race and Mental Health: Past Debates, New Opportunities. In: Avison William R, McLeod Jane D, Pescosolido Bernice A., editors. Mental Health, Social Mirror. New York: Springer; 2007. pp. 169–189. [Google Scholar]
- Evenson Renae J, Simon Robin W. Clarifying the Relationship between Parenthood and Depression. Journal of Health and Social Behavior. 2005;46(4):341–358. doi: 10.1177/002214650504600403. [DOI] [PubMed] [Google Scholar]
- Ferraro Kenneth F, Farmer Melissa M. Double Jeopardy to Health Hypothesis for African Americans: Analysis and Critique. Journal of Health and Social Behavior. 1996a;37(1):27. [PubMed] [Google Scholar]
- Ferraro Kenneth F, Farmer Melissa M. Double Jeopardy, Aging as Leveler, Or Persistent Health Inequality? A Longitudinal Analysis of White and Black Americans. The Journals of Gerontology: Series B, Psychological Sciences and Social Sciences. 1996b;51(6):S319–28. doi: 10.1093/geronb/51b.6.s319. [DOI] [PubMed] [Google Scholar]
- Fossett Mark A, Kielcolt K Jill. Mate Availability and Family Structure among African Americans in U.S. Metropolitan Areas. Journal of Marriage and the Family. 55:302–31. [Google Scholar]
- Gazmararian Julie A, James Sherman A, Lepkowski James M. Depression in Black and White Women. The Role of Marriage and Socioeconomic Status. Annals of Epidemiology. 1995;5(6):455–463. doi: 10.1016/1047-2797(95)00061-5. [DOI] [PubMed] [Google Scholar]
- George Linda K, Lynch Scott M. Race Differences in Depressive Symptoms: A Dynamic Perspective on Stress Exposure and Vulnerability. Journal of Health and Social Behavior. 2003;44(3):353. [PubMed] [Google Scholar]
- Geronimus Arline T. Black/White Differences in the Relationship Of Maternal Age To Birthweight: A Population-Based Test Of The Weathering Hypothesis. Social Science & Medicine. 1996;42(4):589–597. doi: 10.1016/0277-9536(95)00159-x. [DOI] [PubMed] [Google Scholar]
- Geronimus Arline T. Understanding and Eliminating Racial Inequalities in Women's Health in the United States: The Role of the Weathering Conceptual Framework. Journal of the American Medical Women's Association. 2001;56(4):133–6. 149–50. [PubMed] [Google Scholar]
- Goldstein H. Multilevel statistical models. London, Edward Arnold New York: Halstead Press; 1995. [Google Scholar]
- Gove Walter R. Sex Differences in Mental Illness among Adult Men and Women: An Evaluation of Four Questions Raised regarding the Evidence on the Higher Rates of women. Social Science & Medicine, Part B: Medical Anthropology. 1978;12:187–198. doi: 10.1016/0160-7987(78)90032-7. [DOI] [PubMed] [Google Scholar]
- Grundy Emily, Gemma Holt. Adult Life Experiences and Health in Early Old Age in Great Britain. Social Science & Medicine. 2000;51(7):1061–1074. doi: 10.1016/s0277-9536(00)00023-x. [DOI] [PubMed] [Google Scholar]
- Hughes Mary E, Waite Linda J. Marital Biography and Health at Mid-Life. Journal of Health and Social Behavior. 2009;50(3):344–358. doi: 10.1177/002214650905000307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson Pamela B. Role Occupancy and Minority Mental Health. Journal of Health and Social Behavior. 1997;38(3):237. [PubMed] [Google Scholar]
- Jones-Webb Rhonda J, Snowden Lonnie R. Symptoms of Depression among Blacks and Whites. American Journal of Public Health. 1993;83(2):240–244. doi: 10.2105/ajph.83.2.240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kelley-Moore Jessica A, Ferraro Kenneth F. The Black/White Disability Gap: Persistent Inequality in Later Life? Journal of Gerontology: Social Sciences. 2004;59B(1):S34–S43. doi: 10.1093/geronb/59.1.s34. [DOI] [PubMed] [Google Scholar]
- Keith Verna M, Brown Diane R. African American Women and Mental Well-Being: The Triangulation of Race, Gender, and Socioeconomic Status. In: Scheid Teresa L, Brown Tony N., editors. A Handbook for the Study of Mental Health: Social Contexts, Theories, and Systems. 2nd. New York: Cambridge University Press; 2010. pp. 291–305. [Google Scholar]
- Kessler Ronald C, Foster Cindy, Webster Pamela S, House James S. The Relationship between Age and Depressive Symptoms in Two National Surveys. Psychology and Aging. 1992;7(1):119–126. doi: 10.1037//0882-7974.7.1.119. [DOI] [PubMed] [Google Scholar]
- Kessler Ronald C, Neighbors Harold W. A New Perspective on the Relationships among Race, Social Class, and Psychological Distress. Journal of Health and Social Behavior. 1986;27(2):107. [PubMed] [Google Scholar]
- Jinyoung Kim, Durden Emily. Socioeconomic Status and Age Trajectories of Health. Social Science & Medicine. 2007;65(12):2489–2502. doi: 10.1016/j.socscimed.2007.07.022. [DOI] [PubMed] [Google Scholar]
- Koropeckyj-Cox Tanya, Pienta Amy M, Brown Tyson H. Women of the 1950s and the “Normative” Life Course: The Implications of Childlessness, Fertility Timing, and Marital Status for Psychological Well-being in Late Midlife. International Journal of Aging & Human Development. 2007;64(4):299–330. doi: 10.2190/8PTL-P745-58U1-3330. [DOI] [PubMed] [Google Scholar]
- Marks Nadine F, Lambert James D. Marital Status Continuity and Change among Young and Midlife Adults: Longitudinal Effects on Psychological Well-Being. Journal of Family Issues. 1998;19(6):652–686. [Google Scholar]
- McKelvey Mary W, McKenry Patrick C. The Psychosocial Well-Being of Black and White Mothers Following Marital Dissolution. Psychology of Women Quarterly. 2000;24(1):4–14. [Google Scholar]
- Mirowsky John. Age and the Gender Gap in Depression. Journal of Health and Social Behavior. 1996;37(4):362. [PubMed] [Google Scholar]
- Mirowsky John, Ross Catherine E. Social Causes of Psychological Distress. Hawthorne, N.Y: Aldine de Gruyter; 2003. [Google Scholar]
- Mirowsky John, Ross Catherine E. Depression, Parenthood, and Age at First Birth. Social Science & Medicine. 2002;54:1281–1298. doi: 10.1016/s0277-9536(01)00096-x. [DOI] [PubMed] [Google Scholar]
- Mirowsky John, Ross Catherine E. Age and Depression. Journal of Health and Social Behavior. 1992;33(3):187. [PubMed] [Google Scholar]
- Penninx Brenda WJH. Women's Aging and Depression. In: Keyes Corey LM, Goodman Sherryl H., editors. Women and Depression. A Handbook for the Social, Behavioral, and Biomedical Sciences. Cambridge: Cambridge University Press; 2006. pp. 129–144. [Google Scholar]
- Pinheiro JC, Bates DM. Mixed-effects models in S and S-plus. New York, NY: Springer; 2000. [Google Scholar]
- Radloff Lenore S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Applied Psychological Measurement. 1977;1(3):385–401. [Google Scholar]
- Roxburgh Susan. Untangling Inequalities: Gender, Race, and Socioeconomic Differences in Depression. Sociological Forum. 2009;24(2):357–381. [Google Scholar]
- Schieman Scott, Plickert Gabriele. Functional Limitations and Changes in Levels of Depression Among Older Adults: A Multiple-Hierarchy Stratification Perspective. Journals of Gerontology: Series B. 2007;62(1):S36–S42. doi: 10.1093/geronb/62.1.s36. [DOI] [PubMed] [Google Scholar]
- Schieman Scott, Van Gundy Karen, Taylor John. The Relationship between Age and Depressive Symptoms: A Test of Competing Explanatory and Suppression Influences. Journal of Aging and Health. 2002;14(2):260–285. doi: 10.1177/089826430201400205. [DOI] [PubMed] [Google Scholar]
- Schnittker Jason. Chronic Illness and Depressive Symptoms in Late Life. Social Science & Medicine. 2005;60(1):13–23. doi: 10.1016/j.socscimed.2004.04.020. [DOI] [PubMed] [Google Scholar]
- Skarupski Kimberly A, Mendes de Leon Carlos F, Bienias Julia L, Barnes Lisa L, Everson-Rose Susan A, Wilson Robert S, Evans Denis A. Black-White Differences in Depressive Symptoms among Older Adults Over Time. The Journals of Gerontology: Series B, Psychological Sciences and Social Sciences. 2005;60(3):P136–42. doi: 10.1093/geronb/60.3.p136. [DOI] [PubMed] [Google Scholar]
- Spence Naomi J. The Long-Term Consequences of Childbearing: Physical and Psychological Well-being of Mothers in Later Life. Research on Aging. 2008;30(6):722–751. doi: 10.1177/0164027508322575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spence Naomi J, Eberstein Isaac W. Age at First Birth, Parity, and Post-Reproductive Mortality among White and Black Women in the U.S., 1982-2002. Social Science & Medicine. 2009;68(9):1625–1632. doi: 10.1016/j.socscimed.2009.02.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sudha S, Mutran Elizabeth J, Williams Ishan C, Suchindran Chirayath. Childbearing History and Self-Reported Well-Being in Later Life: Contrasting Older African American and White Women. Research on Aging. 2006;28:599–621. [Google Scholar]
- Taylor Miles G. Timing, Accumulation, and the Black/White Disability Gap in Later Life: A Test of Weathering. Research on Aging. 2008;30(2):226–250. [Google Scholar]
- Twisk Jos, De Vente W. Attrition in Longitudinal Studies. How to Deal with Missing Data. Journal of Clinical Epidemiology. 2002;55(4):329–337. doi: 10.1016/s0895-4356(01)00476-0. [DOI] [PubMed] [Google Scholar]
- Twisk Jos W R. Longitudinal Data Analysis. A Comparison between Generalized Estimating Equations and Random Coefficient Analysis. European Journal ofEpidemiology. 2003;19(8):769–776. doi: 10.1023/b:ejep.0000036572.00663.f2. [DOI] [PubMed] [Google Scholar]
- Umberson Debra, Pudrovska Tetyana, Reczek Corinne. Parenthood, Childlessness, and Well-Being: A Life Course Perspective. Journal of Marriage and Family. 2010;72(3):612–629. doi: 10.1111/j.1741-3737.2010.00721.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walsemann Katrina M, Gee Gilbert C, Geronimus Arline T. Ethnic Differences in Trajectories of Depressive Symptoms: Disadvantage in Family Background, High School Experiences, and Adult Characteristics. Journal of Health and Social Behavior. 2009;50:82–98. doi: 10.1177/002214650905000106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willett John B, Singer Judith D, Martin Nina C. The Design and Analysis of Longitudinal Studies of Development and Psychopathology in Context: Statistical Models and Methodological Recommendations. Development and Psychopathology. 1998;10:395–426. doi: 10.1017/s0954579498001667. [DOI] [PubMed] [Google Scholar]
- Williams David R, Costa Manuela, Leavell Jacinta P. Race and mental Health: Patterns and Challenges. In: Scheid Teresa L, Brown Tony N., editors. A Handbook for the Study of Mental Health: Social Contexts, Theories, and Systems. 2nd. New York: Cambridge University Press; 2010. pp. 268–290. [Google Scholar]
- Williams David R, Takeuchi David T, Adair Russell K. Socioeconomic Status and Psychiatric Disorder among Blacks and Whites. Social Forces. 1992;71(1):179. [PubMed] [Google Scholar]
- Williams Kristi, Frech Adrianne, Carlson Daniel L. Marital Status and Mental Health. In: Scheid Teresa L, Brown Tony N., editors. A Handbook for the Study of Mental Health: Social Contexts, Theories, and Systems. 2nd. New York: Cambridge University Press; 2010. pp. 306–320. [Google Scholar]
- Xiao Xu, Liang Jersey, Bennett Joan M, Quinones Ana R, Ye Wen. Ethnic Differences in the Dynamics of Depressive Symptoms in Middle Aged and Older Americans. Journal of Aging and Health. 2010;22(5):631–652. doi: 10.1177/0898264310370851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yang Yang. Is Old Age Depressing? Growth Trajectories and Cohort Variations in Late-Life Depression. Journal of Health and Social Behavior. 2007;48(1):16–32. doi: 10.1177/002214650704800102. [DOI] [PubMed] [Google Scholar]
- Yang Yang, Lee Linda C. Sex and Race Disparities in Health: Cohort Variations in Life Course Patterns. Social Forces. 2009;87(4):2093–2124. [Google Scholar]