

Abstract
This study examined the relationship between routine work environment stress and posttraumatic stress disorder (PTSD) symptoms in a sample of police officers (N = 180) who were first assessed during academy training and reassessed 1-year later. In a model that included gender, ethnicity, traumatic exposure prior to entering the academy, current negative life events, and critical incident exposure over the last year, routine work environment stress was most strongly associated with PTSD symptoms. We also found that routine work environment stress mediated the relationship between critical incident exposure and PTSD symptoms and between current negative life events and PTSD symptoms. Ensuring that the work environment is functioning optimally protects against the effects of duty-related critical incidents and negative life events outside police service.
Keywords: Work environment, traumatic stress, police officers
Police service is an inherently stressful occupation, which often results in both physical (e.g., cardiovascular, gastrointestinal, musculoskeletal problems) and psychological symptoms (increased depression, anxiety, posttraumatic stress disorder; e.g., Berg et al., 2006). The very nature of police work includes regular and ongoing exposure to confrontation, violence, and potential harm. Exposure to potentially traumatic experiences on a regular basis sets the stage for a series of mental health complications, including posttraumatic stress disorder (PTSD). Factors such as prior trauma history, negative life events, and routine work environment stress also can increase the risk for PTSD symptoms. In this study, we examined all of the aforementioned variables within a larger model, determining the unique contributions of each to PTSD symptoms reported by police officers. This study presents the first wave of data (i.e., baseline traumatic events and year 1 stressors and symptoms) within a prospective longitudinal design, contributing to the understanding of the interrelationships among these stressors (i.e., discrete and chronic) and between these stressors and PTSD symptoms.
Following the terrorist attacks of September 11, 2001, there has been greater attention paid to first responders, including police officers and firefighters, and the risks that each face due to the nature of their work. Although epidemiological studies using probability sampling strategies have not been conducted, several estimates of PTSD in police officers have been reported utilizing samples of convenience. The incidence of current duty-related PTSD in police officers has been found to vary between 7% and 19% (Carlier et al., 1997; Gersons, 1989; Robinson et al., 1997; Maia et al., 2007), with greater rates for those with subsyndromal PTSD. Among 262 Dutch police officers interviewed at 2 weeks, 3 months, and 12 months after experiencing a critical incident, 7% met full diagnostic criteria for current PTSD on at least one of the time points. Moreover, 34% suffered from posttraumatic stress symptoms or subsyndromal PTSD at some point during the study (Carlier et al., 1997). Among 157 Brazilian police officers, 9% met full criteria for PTSD and an additional 16% met criteria for subsyndromal PTSD (Maia et al., 2007).
There has been ongoing debate about which variables are most closely associated with PTSD symptoms in police officers and other first responders, especially given that most are resilient in the face of ongoing potentially traumatic events. Critical incidents have been examined as an important source of mental health symptoms among police officers. A critical incident is a potentially traumatic event which may cause a given individual’s emotional resources to become overtaxed, resulting in a spectrum of reactions from exhaustion to increased and unrelenting mental health symptomatology. Critical incidents often include a component of life threat and may range from being threatened (e.g., with a knife or gun) to direct exposure and/or injury (e.g., accidental or intentional). Critical incidents may impact individual police officers in different ways, with some returning to normal functioning in the immediate aftermath, whereas others require more intensive mental health intervention. There is clear evidence that critical incidents play an important role in the development of PTSD in police officers and other first responders (e.g., Carlier et al., 1997; Ward et al., 2006), with incidents that are perceived as highly threatening having the largest impact on levels of distress (McCaslin et al., 2006).
In addition to critical incident exposures, police officers face a number of other stressors, including negotiation of an inherently complex work environment that contributes to daily and ongoing stress. Theoretical models of work environment stressors often contain components such as organizational constraints (e.g., problems with equipment), coworker factors (e.g., inequitable workload, unsuitable partners), supervision (e.g., lack of feedback, unequal treatment), work content (e.g., unclear roles), and temporal factors (e.g., shift work; Hurrell et al., 1998). Others have divided work environment into organizational (e.g., poor equipment, excessive paperwork, lack of recognition) and operational stressors (e.g., hoax calls, missing meals, dealing with the public; Brough, 2004).
Although previous research has suggested that critical incidents are the driving force behind development of PTSD, more recent research has highlighted that routine work environment stressors may play an important role in the development and maintenance of psychological distress in police officers. For example, Collins and Gibbs (2003) found that the most highly ranked stressors among police were not related to critical incidents, but rather to concerns with the work environment, including a lack of consultation and communication, lack of control over workload, inadequate support, and general excessive workload. Carlier et al. (1997) found that work environment factors such as dissatisfaction with organizational support predicted PTSD symptoms in police officers. Similarly, Liberman et al. (2002) found that routine work stressors were associated with PTSD symptoms, and that these effects were independent from, and larger than, the effects of cumulative critical incident exposure.
Within the work environment, it is also important to consider how perceived discrimination contributes to subsequent mental health symptomatology. Among police officers, there is evidence that women and ethnic minorities report more negative social interactions and discrimination (i.e., criticism, bias, sexual harassment) within the context of the work environment (Morris, 1996). Consequently, discrimination should be included as part of any routine work environment stress construct. Morash and Haarr (1995) found that female officers experienced greater harassment and bias in their work environment despite multiple similarities between reported sources of stress in male and female police officers. Similarly, Thompson et al. (2006) examined a 3-factor model of sources of perceived stress in female officers, and found that interpersonal work environment stressors (i.e., lack of support from colleagues, gender discrimination, sexual harassment, interpersonal conflict, and lack of confidentiality; Thompson et al., 2006) contributed to the largest percentage of variance in reported stress; organizational and operational stress also contributed to overall levels of stress among female officers. Despite a great deal of evidence supporting the relationship between various aspects of the work environment and PTSD symptoms, there has also been evidence to the contrary. For example, Brough (2004) found that in a sample of police officers, while operational stressors predicted PTSD symptoms, organizational stressors did not.
There is also precedent for examining the contribution of environmental factors among other groups, such as veterans of war. For example, in their comprehensive model, King et al., (1995) studied the contribution of a number of war zone stressors in predicting PTSD symptoms in Vietnam veterans and found that malevolent environment (i.e., daily occupational and environmental hassles) was the strongest predictor of PTSD symptoms, even when accounting for predictors such as traditional combat, perceived threat, and atrocities committed by surveyed veterans (King et al., 1995). The construct of a malevolent environment can be quite helpful when conceptualizing contributors of PTSD in police officers, who face life threat and exposure to traumatic events in the line of duty. Both the findings, King et al. (1995) with Vietnam veterans and Liberman et al. (2002) with police officers, highlight the fact that the impact of a malevolent environment cannot be underestimated in the context of the development of PTSD, and in fact, may be more strongly associated with PTSD than other variables, including personal life threat.
Events occurring outside of the work environment can also impact the development and maintenance of PTSD symptoms, including negative life events and past trauma. Mikkelsen and Burke (2004) found that in a large sample of police officers, negative life events such as work-family conflict were predictive of poorer psychological health. The association between negative life events and PTSD symptoms also has been found in larger models with veterans of war, with a direct relationship between negative life events and PTSD (e.g., King et al., 1998). Similarly, prior to Operation Desert Storm, negative life events in the year prior to deployment were associated with anxiety, depression, and PTSD symptoms. More recently, in a study of Operation Iraqi Freedom military personnel, negative life events prior to deployment were associated with PTSD symptoms (Maguen et al., 2008).
Past traumatic events also are important to consider within any larger framework, given that there is evidence that prior trauma contributes to current symptoms. Individuals with a past trauma history have greater difficulty recovering from subsequent life stressors and threats than individuals with no trauma history, and prior exposure to trauma is a risk factor for chronic PTSD stemming from a subsequent trauma (Brunet et al., 2001; Dougall et al., 2000; King et al., 1999; Stretch et al., 1998). For example, Dougall et al. (2000) found that prior trauma that differs from an individual’s exposure to current trauma is a risk factor for the development of adverse mental health reactions, such as posttraumatic stress symptoms. In police academy recruits, childhood trauma appears to be a risk factor for the development of subsequent anxiety disorder symptoms, as demonstrated by an increased catecholamine response to psychological stress (Otte et al., 2005) and increased acoustic startle reactivity (Pole et al., 2007). In veterans of war, prior trauma is consistently found to be a risk factor for the subsequent development of PTSD (e.g., King et al., 1999).
In the current study, our goal was to better understand the relationship between work environment and PTSD symptoms after 1 year of police service. We hypothesized that among all included model variables, routine work environment stress would have the strongest relationship with PTSD symptoms and also serve as a mediator between several risk factors (i.e., life threatening critical incident exposure, negative life events outside police service, and prior trauma) and PTSD symptoms. We also were interested in whether women and ethnic minorities were more likely to report an aversive work environment due to reported discrimination, with work environment hypothesized to serve as a mediator between these demographic variables and the subsequent development of PTSD symptoms.
METHOD
Participants
Participating police officers (N = 180) were recruited from 4 urban police departments, the New York Police Department (NYPD) and 3 departments in the San Francisco Bay Area (Oakland, OPD; San Francisco, SFPD; and San Jose, SJPD) during police academy training.
The average age of police officers in this sample was 27 years (SD = 4.70), and 87% (n = 157) were men. Participants were White (47%), Latino (20%), Asian American/Pacific Islander (15%), and African American (10%), with 8% reporting other or multiple ethnicities. Over 3 quarters of participants were unmarried (77%) and the majority completed at least some college (89% completed 2– 4 years of college, 5.1% had completed a graduate degree).
Procedures
Academy trainees were introduced to the study through an in-person presentation made by study personnel during academy training classes. This presentation included the distribution of 2 letters, one from the commissioner or police chief of the affiliated department and one from the study team. A description of the study procedures, a contact number, and a participation form including the option to be contacted by the study team were all included with the approach letters. In addition to in-person presentations, informational flyers were posted at each academy which also provided contact information for the study team. Data were collected as part of a larger prospective and longitudinal study of police officer stress and health, and this report presents findings in the first 180 academy recruits enrolled. Study participants were recruited from a total of 5855 academy cadets in the Bay Area and New York and represent a sample of convenience. Compared with their respective academy classes, New York and Bay Area samples enrolled in our study were representative in terms of age, gender, and ethnicity.
Participants were evaluated at baseline, while still in training at the police academy, and 12 months after commencement of police training. For the first year of police duty, newly trained officers are all assigned to street patrol. Of those eligible for their 1-year assessment, 82% of participants interviewed at baseline were also interviewed at 12 months. Prior to each assessment, study procedures were described in detail and written informed consent was obtained. The baseline and 12-month assessments included a self-report questionnaire package and a structured interview of prior trauma exposure. The self-report questionnaire assessed psychological functioning, and measures that were used for the purposes of this investigation included demographic information (baseline), negative life events (12 months), routine work environment stress (12 months), and PTSD symptoms (12 months). The structured interview included a detailed assessment of prior trauma exposure (baseline).
All procedures were approved by the University of California Human Subjects Committee and Institutional Review Board. Participants were also informed that a Federal Certificate of Confidentiality was obtained for the study which assured that any information obtained under the auspices of this study is protected in that it cannot be disclosed to department personnel, nor may it be subpoenaed in either criminal or civil court.
Measures
Demographics
Participants were asked to report the following demographic variables: age, gender, ethnic minority status, marital status, and education.
Prior Trauma Exposure
Prior trauma was measured with the Life Stressor Checklist-Revised (LSC-R; Wolfe et al., 1996), a 30-item measure of lifetime exposure to stressful life events. For each potentially traumatic event, individuals were verbally asked whether: (1) each event happened to them and (2) whether they believed that they could have been killed or seriously harmed as a result of the particular event. In order for the individual to score positively on any given item, both conditions must have been met. For the purposes of this study, prior trauma history was defined as experiencing any 1 of 9 life threatening events listed on the LSC-R. Items included experiencing serious disaster, serious accident (or accident-related injury), very serious physical and mental illness, physical neglect, abortion or miscarriage (for women), physical assault, physical abuse, sexual assault, and/or sexual abuse. Military and preacademy critical incident items were not included in this measure. Participants either endorsed no prior trauma (41%), 1 (31%), 2 (19%), or 3 (9%) prior traumatic events.
Negative Life Events
Negative life events in the past year were measured with the Life Experiences Survey (LES; Sarason et al., 1978). The LES contains 50-items describing life changes (e.g., death of a family member, marriage, accidents, financial change) each of which are rated on a 7-point Likert scale ranging from “extremely negative” to “extremely positive” influence. If an event did not occur, the item is coded as zero. Every event that occurred is coded as one “life change unit.” These units are then summed to create a total score. Positive and negative events are summed separately. In the current investigation, we used negative life events reported in the last 12 months. The LES has been shown to have good validity and reliability, although the authors caution that reliability may be underestimated due to the frequency of change concerning many of these life events. In this study, individuals reported a range of 0 to 24 negative life events in the last 12 months, with a mean of 4.42 negative life events (SD = 4.74).
Critical Incident History Questionnaire
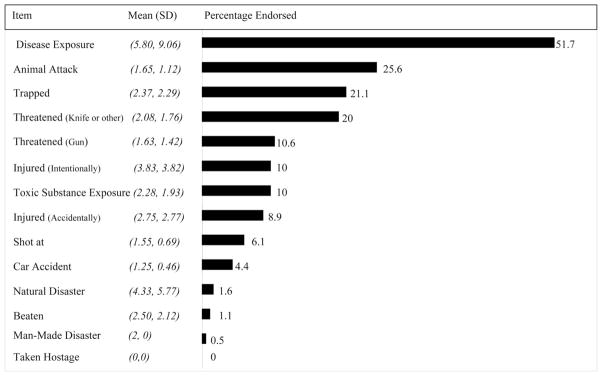
The Critical Incident History Questionnaire (CIHQ) is a 39-item self-report measure designed to produce a measure of cumulative exposure to critical incidents (Brunet et al., 1998; Weiss et al., 2004). Participants tabulate the number of times (frequency of exposure) that they have personally experienced each of the 39 critical incidents in the line of duty. The total cumulative exposure score is derived by summing the frequency of incident exposure across all items. The CIHQ demonstrated good agreement on incident severity ratings (0.94), and adequate convergent and divergent validity (Weiss et al., 2004). For the purposes of this study, we used 14 items that were personally life threatening to police officers in the last year (see Table 1 for percentages of police officers endorsing each item, as well as frequency of exposure among those endorsing item). In this sample, CIHQ sum score was found to be skewed and as a result, statistical analyses were carried out on the log-transformed values of this sum variable to normalize its distribution.
TABLE 1.
Frequency and Percentage of Critical Incident Personal Life Threat Items Endorsed by Police Officers
|
Work Environment Inventory
The Work Environment Inventory (WEI) is a 68-item measure in which police officers are asked to respond on a 5-point Likert scale to several statements about police service with responses ranging from “strongly disagree” to “strongly agree” (coded as −2 to 2) (Liberman et al., 2002). Positive and negatively phrased items are counterbalanced, positively phrased items were reverse coded, and higher scores indicate greater work environment stress. Topics evaluated include issues concerning management and administration, supervisors, equipment, training, boredom, role conflict, peers, shift work, work-related discrimination (i.e., concerning gender, ethnicity, and sexual orientation), and public attitudes towards police work (see Table 2 for sample items). For the purposes of this study, we used the mean item score on the WEI. Although a prior factor analysis has found more than one factor (e.g., Liberman et al., 2002), that earlier sample included older and more established police officers. We were unable to replicate these findings with our sample of new recruits; therefore we employed the WEI as a single factor, as was justified by our factor analysis. Mean item scores ranged from −2 to 0.84 (M = −0.44, SD = 0.46). Lieberman et al. (2002) found this measure to have good validity and reliability, with a Cronbach alpha of 0.92. The Cronbach alpha for the current sample is 0.91.
TABLE 2.
Means and Standard Deviations of the Ten Most Frequently Endorsed Routine Work Environment Stressors
| List | Item | Mean | SD |
|---|---|---|---|
| 1 | The criminal sentences given in court are about the right length and severity.* | 1.08 | 0.89 |
| 2 | The demands and nature of police work and the personal problems it could cause (like alcoholism, emotional depression, and anxiety) are about the same as in most jobs.* | 0.90 | 0.88 |
| 3 | The public criticizes the members of my profession unfairly. | 0.85 | 0.96 |
| 4 | I am not paid enough for what I do. | 0.79 | 1.34 |
| 5 | As a whole, variable work shifts and days off are a desirable part of my job.* | 0.77 | 1.02 |
| 6 | The administration/management seems to understand and care about my problems.* | 0.69 | 0.95 |
| 7 | The patrol cars that I regularly use are in safe condition.* | 0.68 | 0.92 |
| 8 | I do not let my neighbors know what I do for a living. | 0.34 | 1.21 |
| 9 | Working a night shift does not cause problems for my family or social life.* | 0.34 | 1.17 |
| 10 | Working a night shift disrupts my eating and sleeping. | 0.33 | 1.24 |
Reverse coded items.
Mississippi Combat Scale-Civilian Version
The Mississippi Combat Scale-Civilian Version (MCS-CV) is a 35-item measure that assesses PTSD-related symptoms of intrusion, avoidance, emotional numbing, hyperarousal, and related functional impairment (Keane et al., 1988). Items are rated on a 5-point Likert scale, with responses ranging from “not at all true” to “extremely true,” with higher sum scores indicating greater PTSD symptomatology. The civilian version has been used to assess PTSD symptoms in nonveteran controls in the National Vietnam Veterans Readjustment Study (NVVRS; Kulka et al., 1990) and in emergency services personnel following a disaster (Marmar et al., 1996; Weiss et al., 1995). For this study, police officers were asked to report the extent to which they have experienced each item, “since beginning police service.” The Cronbach alpha for the current sample is 0.80. The mean score for the MCS-CV for this sample is 61 (SD = 11, range, 36 –100). As expected, these norms are below those for PTSD patients (M = 130, SD = 18) and psychiatric patients (M = 86, SD = 26; Keane et al., 1988).
Data Analytic Procedure
We were interested in both the direct and indirect effects of gender, ethnicity, prior trauma, negative life events, critical incident exposure, and work environment on PTSD, as well as examining work environment as a mediator between each of the other variables and PTSD. Subsequently, a just-identified path analysis model was conducted with M-plus version 5.1 (Muthén and Muthén, 2007; Fig. 1); as a result, fit indices are not reported. The direct and indirect effects of each of these pathways are reported below.
FIGURE 1.

Path Model Predicting PTSD Symptoms in Police Officers.
RESULTS
Path Analysis
Prior to examining the paths of the specified model (Fig. 1) we first investigated correlations between each of the included variables to ensure there would be no concerns with multicollinearity (see Table 3). Next, we ran the proposed model in M-plus and found that it accounted for 33% of the variance in PTSD symptoms; we also determined that there were several direct paths to PTSD symptoms (see Table 4). The following variables were found to have a direct effect on PTSD symptoms: ethnicity (B = −0.20, t = −3.25, p < 0.01), negative life events in the past 12 months (B = 0.19, t = 2.94, p < 0.01), critical incident exposure (B = 0.15, t = 2.33, p < 0.05), and work environment (B = 0.36, t = 5.79, p < 0.01). There were also 2 variables with significant indirect paths to PTSD symptoms: negative life events (past 12-months; B = 0.08, t = 2.81, p < 0.05) and critical incident exposure (B = 0.07, t = 2.28, p < 0.05). There were also direct effects from the following variables to work environment: negative life events (past 12 months; B = 0.23 t = 3.19, p < 0.01), and critical incident exposure (B = 0.18, t = 2.50, p < 0.05). Given all of these direct and indirect paths, work environment was found to partially mediate the relationship between negative life events and PTSD symptoms and between critical incident exposure and PTSD symptoms.
TABLE 3.
Correlations Among Variables in Path Model
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| 1. Gender (87% male) | — | ||||||
| 2. Ethnicity (47% white) | −0.09 | — | |||||
| 3. Prior trauma (M = 1.00, SD = 0.97) | 0.17* | −0.13 | — | ||||
| 4. Negative life events (M = 4.42, SD = 4.74) | 0.05 | −0.06 | 0.07 | — | |||
| 5. CI exposure (M = 1.25, SD = 1.10) | −0.22** | 0.09 | 0.09 | 0.21** | — | ||
| 6. Work environment (M = −0.44, SD = 0.46) | −0.04 | 0.05 | 0.09 | 0.26** | 0.24** | — | |
| 7. PTSD symptoms (M = 61, SD = 11) | −0.01 | −0.19* | 0.20** | 0.33** | 0.28** | 0.45** | — |
p < 0.05, 2-tailed;
p < 0.01, 2-tailed.
Gender: 1 = male, 2 = female; ethnicity: 0 = ethnic minority, 1 = white; NLE indicates negative life events checklist; CI, log transformed number of critical incidents experienced in first year of police service.
TABLE 4.
Direct and Indirect Effects for the Path Model of PTSD Symptoms
| Model Variable | St. Beta | SE |
|---|---|---|
| Prior trauma | ||
| Direct effect | 0.12 | 0.06 |
| Total indirect effects | 0.07 | 0.04 |
| Specific indirect effects | 0.02 | 0.03 |
| Total effect | 0.19** | 0.07 |
| Gender | ||
| Direct effect | −0.01 | 0.06 |
| Total indirect effects | −0.04 | 0.04 |
| Specific indirect effects | −0.01 | 0.03 |
| Total effect | −0.05 | 0.07 |
| Ethnicity | ||
| Direct effect | −0.20** | 0.06 |
| Total indirect effects | 0.03 | 0.04 |
| Specific indirect effects | 0.02 | 0.03 |
| Total effect | −0.17* | 0.07 |
| Negative life events | ||
| Direct effect | 0.19** | 0.07 |
| Total indirect effects | 0.08* | 0.03 |
| Specific indirect effects | 0.08* | 0.03 |
| Total effect | 0.28** | 0.07 |
| Critical incidents | ||
| Direct effect | 0.15* | 0.07 |
| Total indirect effects | 0.07* | 0.03 |
| Specific indirect effects | 0.07* | 0.03 |
| Total effect | 0.22** | 0.07 |
| Work environment | ||
| Direct effect | 0.36** | 0.06 |
| Total indirect effects | —– | —– |
| Specific indirect effects | —– | —– |
| Total effect | 0.36** | 0.06 |
p < 0.05,
p < 0.01.
St. Beta indicates standardized beta; SE, standard error for standardized effects; specific indirect effects = indirect effects with WEI as mediator; gender: 1 = male, 2 = female; ethnicity: 0 = ethnic minority, 1 = white.
DISCUSSION
In the specified model, work environment had the strongest association with PTSD symptoms, above and beyond the effects of exposure to duty-related critical incidents and negative life events outside police service. A supportive work environment includes both organizational and operational aspects, as well as a nondiscriminatory milieu. Extending the findings of Liberman et al. (2002) this study highlights that work environment stressors such as equipment not working, daily operational hassles, being unclear about work roles, stressful relationships with coworkers, feelings of discrimination, etc. have a direct impact on PTSD symptoms. This finding echoes King et al’s. (1995) finding in veterans of war, which demonstrated that malevolent environment was the most robust predictor of PTSD symptoms.
This finding has significant implications for the prevention and management of PTSD symptoms among police officers, and highlights the importance of fostering a supportive and accommodating work environment. In this context, a compassionate work environment becomes a protective factor that arguably shields police officers against the development of PTSD. Indeed, Paton (2006) argues that the organization defines the context in which critical incidents are interpreted and processed, thereby impacting an individual officer’s meaning making and subsequent coping sequelae. Subsequently, the development of resilient organizations that can shape individual socialization, training and response is important. Given that often resilience factors have been conceptualized as preexisting (e.g., individual temperament, absence of prior abuse history, biological and psychological inoculation, etc.), work environment is noteworthy as a highly influential resilience and protective factor that is potentially mutable in the prevention of problematic mental health symptoms.
Work environment can also be seen as a proxy for cohesion and morale, and future studies should investigate the relationships between these variables and PTSD symptoms in a cohort of police officers. There is a rich body of literature that demonstrates the protective nature of these variables in PTSD among soldiers and veterans (e.g., Bartone et al., 1998; Maguen and Litz, 2006; Maguen et al., 2004). Work environment may also be a proxy for leadership effectiveness, with several studies demonstrating that strong leadership buffers against the adverse effects of stress, and enables role clarity, morale, and job engagement (e.g., Britt et al., 2004).
We also found that work environment mediated the relationship between critical incident exposure and PTSD symptoms as well as between negative life events and PTSD symptoms, demonstrating an even more complex relationship with variables that are seen to be central to the development of PTSD. A supportive work environment arguably can buffer against the development of PTSD even in those who have been exposed to horrific critical incidents and are experiencing unpredictable negative life events in their personal lives. Although the police department has little control over exposure to critical incidents and negative events that occur across the lifespan, a protective work environment can be a valuable and attainable asset for young police officers.
Notably, prior trauma history was not significantly related to either PTSD or work environment. This finding is encouraging, suggesting that other stressors operate separately from the impact of prior trauma and that when other variables are considered, exposure to traumatic events prior to entering police service is not as important in predicting PTSD as other, more controllable variables such as the work environment. As a result, a prior trauma history should not merely be seen as a liability as it relates to police service, and its effects should always be considered as part of a larger model, taking other important variables into account.
Finally, we did not find a significant relationship between demographic variables (i.e., gender, ethnicity) and work environment stress, despite prior evidence to the contrary (e.g., Morash and Haarr, 1995; Morris, 1996; Thompson et al., 2006). One possibility is that progressive policies that have been implemented by leadership in law enforcement to safeguard the work environment from unequal treatment based on gender and ethnicity may be paying dividends. Another possibility is that our measure of work environment was more comprehensive, and as a result may contain added dimensions of the work environment, as compared with prior studies that examine these relationships with a narrower focus on discrimination. Although it is an encouraging finding that there were no gender or ethnic minority differences in overall reports of the work environment, future research should continue to explore the relationship between these variables among police officers in greater detail. It is also noteworthy that there was a significant association between gender and critical incidents, with men reporting greater exposure. Consequently, it will be important to track this exposure over time in women; perhaps as exposure to critical incidents increases, this will also impact the relationship with work environment for women.
There are several important limitations that should be noted. Although we have a comprehensive measure of work environment, related constructs such as cohesion, morale, and strength of leadership were not directly measured, and each of these may be important in explaining some of the variance in both the work environment and in PTSD symptoms. Furthermore, it would be useful to use a more comprehensive measure of work-related discrimination to capture some of the subtleties that emerge as part of this construct. While our measure asks about these behaviors in general ways, utilizing a more specific measure would allow for a closer analysis and understanding of the ways in which discrimination in the work environment may impact the mental health and job satisfaction of ethnic minorities and women. Although the primary goal of this analysis was to look at the work environment as a whole, future studies should consider the issue of discrimination and its impact on cohesion and morale in more intricate ways. Another limitation is the inherent complexity that arises when collecting measures at a specific time point, and the resulting inability to make conclusions about temporal relationships. More specifically, in this study, negative life events, critical incident exposure, work environment stress, and PTSD symptom measures were each collected at 12 months. Therefore, we are unable to ascertain chronology and unable to make any conclusions about directionality. Over time, as we collect data at multiple time points, we will be in a better position to understand these temporal relationships (e.g., how work environment impacts PTSD symptoms over time). A sample of convenience was employed in this study, so results should be interpreted with caution. Findings related to women and ethnic minorities should also be interpreted with caution, given small sample sizes. Additionally, to make this study truly prospective we excluded personnel with prior experience in combat, law enforcement, and emergency services who reported prior critical incidents, which may limit generalizability. Biases that may arise due to self-selection and time 2 attrition also may limit generalizability.
CONCLUSIONS
Overall, the finding that work environment is most strongly associated with PTSD symptoms, above and beyond critical incidents and negative life events, has important implications for strengthening resilience and protective factors in police officers. Closely monitoring work environment is important and may become a marker of overall well being in this group. Ensuring that each part of the work environment is functioning at its highest capacity not only ensures that the entire system works more smoothly, but also protects against the effects of duty-related critical incidents and negative life events that are experienced as a part of everyday life. As we come to better understand the impact of this variable on mental health over time in this cohort, possible interventions that can help mitigate work environment stressors will become more apparent and closely tailored. These interventions arguably will not only impact each aspect of the work environment, but also have a broader effect on morale and cohesion within police units.
References
- Bartone PT, Adler AB, Vaitkus MA. Dimensions of psychological stress in peacekeeping operations. Mil Med. 1998;163:587–593. [PubMed] [Google Scholar]
- Berg AM, Hem E, Lau B, Ekeberg Ø. An exploration of job stress and health in the Norwegian police service: A cross sectional study. J Occup Med Toxicol. 2006;1:26. doi: 10.1186/1745-6673-1-26. Available at: http://www.occup-med.com/content/1/1/26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Britt TW, Davison J, Bliese PD, Castro CA. How leaders can influence the impact that stressors have on soldiers. Mil Med. 2004;169:541–545. doi: 10.7205/milmed.169.7.541. [DOI] [PubMed] [Google Scholar]
- Brunet A, Boyer R, Weiss DS, Marmar CR. The effects of initial trauma exposure on the symptomatic response to a subsequent trauma. Can J Behav Sci. 2001;33:97–102. [Google Scholar]
- Brunet A, Weiss D, Best SR, Liberman A, Fagan J, Marmar CR. Assessing recurring traumatic exposure: the Critical Incident History Questionnaire. Washington DC: International Society for Traumatic Stress Studies; 1998. p. 49. [Google Scholar]
- Brough P. Comparing the influence of traumatic and organizational stressors on the psychological health of police, fire and ambulance officers. Int J Stress Manag. 2004;11:227–224. [Google Scholar]
- Carlier IE, Lamberts RD, Gersons BR. Risk factors for posttraumatic stress symptomatology in police officers: A prospective analysis. J Nerv Ment Dis. 1997;185:498–506. doi: 10.1097/00005053-199708000-00004. [DOI] [PubMed] [Google Scholar]
- Collins PA, Gibbs A. Stress in police officers: a study of the origins, prevalence and severity of stress-related symptoms within a county police force. Occup Med. 2003;53:256–264. doi: 10.1093/occmed/kqg061. [DOI] [PubMed] [Google Scholar]
- Dougall AL, Herberman HB, Delahanty DL, Inslicht SS, Baum A. Similarity of prior trauma exposure as a determinant of chronic stress responding to an airline disaster. J Consult Clin Psychol. 2000;68:290–295. doi: 10.1037//0022-006x.68.2.290. [DOI] [PubMed] [Google Scholar]
- Gersons BP. Patterns of PTSD among police officers following shooting incidents: A two dimensional model and treatment implications. J Trauma Stress. 1989;2:247–257. [Google Scholar]
- Hurrell JJ, Nelson DL, Simmons BL. Measuring job stressors and strains: Where we have been, where we are and where we need to go. J Occup Health Psychol. 1998;3:368–389. doi: 10.1037//1076-8998.3.4.368. [DOI] [PubMed] [Google Scholar]
- Keane TM, Caddell JM, Taylor KL. Mississippi Scale for Combat-Related Posttraumatic Stress Disorder: Three studies in reliability and validity. J Consult Clin Psychol. 1988;56:85–90. doi: 10.1037//0022-006x.56.1.85. [DOI] [PubMed] [Google Scholar]
- King LA, King DW, Fairbank JA, Keane TM, Adams GA. Resilience-recovery factors in post-traumatic stress disorder among female and male Vietnam veterans: Hardiness, postwar social support and additional stressful life events. J Pers Soc Psychol. 1998;74:420–434. doi: 10.1037//0022-3514.74.2.420. [DOI] [PubMed] [Google Scholar]
- King DW, King LA, Foy DW, Keane TM, Fairbank JA. Posttraumatic stress disorder in a national sample of female and male Vietnam veterans: Risk factors, war-zone stressors and resilience-recovery variables. J Abnorm Psychol. 1999;108:164–170. doi: 10.1037//0021-843x.108.1.164. [DOI] [PubMed] [Google Scholar]
- King D, King L, Gudanowski D, Vreven DL. Alternative representations of war zone stressors: Relationships to posttraumatic stress disorder in male and female Vietnam veterans. J Abnorm Psychol. 1995;104:184–196. doi: 10.1037//0021-843x.104.1.184. [DOI] [PubMed] [Google Scholar]
- Kulka RA, Schlenger WE, Fairbank JA, Hough RL, Jordan BK, Marmar CR, Weiss DS. Trauma and the Vietnam War generation: Report on the findings from the National Vietnam Veterans Readjustment Study. New York: Brunner/Mazel; 1990. [Google Scholar]
- Liberman AM, Best SR, Metzler TJ, Fagan JA, Weiss DS, Marmar CR. Routine occupational stress and psychological distress in police. Policing. 2002;25:421–439. [Google Scholar]
- Maguen S, Litz BT. Predictors of morale in US peacekeepers. J Appl Soc Psychol. 2006;36:820–836. [Google Scholar]
- Maguen S, Litz BT, Wang JL, Cook M. The stressors and demands of peacekeeping in Kosovo: Predictors of mental health response. Mil Med. 2004;169:198–206. doi: 10.7205/milmed.169.3.198. [DOI] [PubMed] [Google Scholar]
- Maguen S, Turcotte DM, Peterson AL, Dremsa TL, Garb HN, McNally RJ, Litz BT. Description of risk and resilience factors among military medical personnel before deployment to Iraq. Mil Med. 2008;173:1–9. doi: 10.7205/milmed.173.1.1. [DOI] [PubMed] [Google Scholar]
- Maia DB, Marmar CR, Metzler T, Nobrega A, Berger W, Mendlowicz MV, Coutinho ES, Figueira I. Post-traumatic stress symptoms in an elite unit of Brazilian police officers: Prevalence and impact on psychosocial functioning and on physical mental health. J Affect Disord. 2007;97:241–245. doi: 10.1016/j.jad.2006.06.004. [DOI] [PubMed] [Google Scholar]
- McCaslin SE, Rogers CE, Metzler TJ, Best SR, Weiss DS, Fagan JA, Liberman A, Marmar CR. The impact of personal threat on police officers’ responses to critical incident stressors. J Nerv Ment Dis. 2006;194:591–597. doi: 10.1097/01.nmd.0000230641.43013.68. [DOI] [PubMed] [Google Scholar]
- Marmar CR, Weiss DS, Metzler TJ, Ronfeldt HM, Foreman C. Stress responses of emergency services personnel to the Loma Prieta earthquake Interstate 880 freeway collapse and control traumatic incidents. J Trauma Stress. 1996;9:63–85. doi: 10.1007/BF02116834. [DOI] [PubMed] [Google Scholar]
- Mikkelsen A, Burke R. Work-family concerns of Norwegian police officers: Antecedents and consequences. Int J Stress Manag. 2004;11:429–444. [Google Scholar]
- Morash M, Haarr RN. Gender, workplace problems and stress in policing. Justice Q. 1995;12:113–140. [Google Scholar]
- Morris A. Gender and ethnic differences in social constraints among a sample of New York police officers. J Occup Health Psychol. 1996;1:224–235. doi: 10.1037//1076-8998.1.2.224. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus User’s Guide. 5. Los Angeles (CA): Muthén & Muthén; 2007. [Google Scholar]
- Otte C, Neylan TC, Pole N, Metzler T, Best S, Henn-Haase C, Yehuda R, Marmar CR. Association between childhood trauma and catecholamine response to psychological stress in police academy recruits. Biol Psychiatry. 2005;57:27–32. doi: 10.1016/j.biopsych.2004.10.009. [DOI] [PubMed] [Google Scholar]
- Paton D. Critical incident stress risk in police officers: Managing resilience and vulnerability. Traumatology. 2006;12:198–206. [Google Scholar]
- Pole N, Neylan TC, Otte C, Metzler TJ, Best SR, Marmar CR. Association between childhood trauma and emotion-modulated psychophysiological responses to startling sounds: A study of police cadets. J Abnorm Psychol. 2007;116:352–361. doi: 10.1037/0021-843X.116.2.352. [DOI] [PubMed] [Google Scholar]
- Robinson HM, Sigman MR, Wilson JP. Duty-related stressors and PTSD symptoms in suburban police officers. Psychol Rep. 1997;81:835–845. doi: 10.2466/pr0.1997.81.3.835. [DOI] [PubMed] [Google Scholar]
- Sarason I, Johnson J, Siegel J. Assessing the impact of life changes: Development of the Life Experiences Survey. J Consult Clin Psychol. 1978;46:932–946. doi: 10.1037//0022-006x.46.5.932. [DOI] [PubMed] [Google Scholar]
- Stretch RH, Knudson KH, Durand D. Effects of premilitary and military trauma on the development of post-traumatic stress disorder symptoms in female and male active duty soldiers. Mil Med. 1998;163:466–470. [PubMed] [Google Scholar]
- Thompson BM, Kirk A, Brown D. Sources of stress in policewomen: A three-factor model. Int J Stress Manag. 2006;13:309–328. [Google Scholar]
- Ward CL, Lombard CJ, Gwebushe N. Critical incident exposure in South African emergency services personnel: Prevalence and associated mental health issues. Emerg Med J. 2006;23:226–231. doi: 10.1136/emj.2005.025908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiss DS, Brunet A, Best SR, Metzler T, Liberman A, Pole N, Fagan JA, Marmar CR. In International Society of Traumatic Stress Studies. Vol. 52. Miami (FL): 2004. The Critical Incident History Questionnaire: A method for measuring total cumulative exposure to critical incidents in police officers. [Google Scholar]
- Weiss DS, Marmar CR, Metzler TJ, Ronfeldt HM. Predicting symptomatic distress in emergency services personnel. J Consult Clin Psychol. 1995;63:361–368. doi: 10.1037//0022-006x.63.3.361. [DOI] [PubMed] [Google Scholar]
- Wolfe JW, Kimerling R, Brown PJ, Chresman KR, Levin K. Psychometric review of the life stressor checklist-revised. In: Stamm BH, editor. Measurement of Stress, Trauma and Adaptation. Lutherville (MD): Sidran Press; 1996. pp. 676–679. [Google Scholar]