

Abstract
Transstyloid, transscaphoid, transcapitate fractures are uncommon. We report the case of a 28-year-old man who sustained this fracture following direct trauma. The patient was successfully treated by open reduction internal fixation of the scaphoid and proximal capitate fragment, with a good clinical outcome at 1-year follow-up. This pattern is a new variant of scaphocapitate fracture as involves a fracture of the radial styloid as well.
Background
Transstyloid, transscaphoid, transcapitate fractures are extremely rare. A fracture of the capitate is uncommon due to its anatomical position and cuboidal shape.1 The incidence of capitate fractures is between 0.2% and 1.3% of all carpal bone fractures.2 3 Rotation of the proximal fragment of the capitate through 90 or 180 combined with a scaphoid fracture has been previously reported.4 5 We report a variant of scaphocapitate fracture with an associated radial styloid fracture.
Case presentation
A 28-year-old man presented with a painful, swollen right wrist following an assault. On examination, he had tenderness in the anatomical snuff box, the dorsal and palmar aspects of his wrist. Gross limitation of movement in all directions was noted. There was no neurovascular compromise. He had a history of a right scaphoid fracture 6 years previously, but did not attend follow-up clinics.
Investigations
Plain radiographs showed a transstyloid, transscaphoid, transcapitate fracture (figure 1). A CT scan was also performed and confirmed significant rotation of the proximal fragment of the capitate in addition to the fractures (figure 2).
Figure 1.
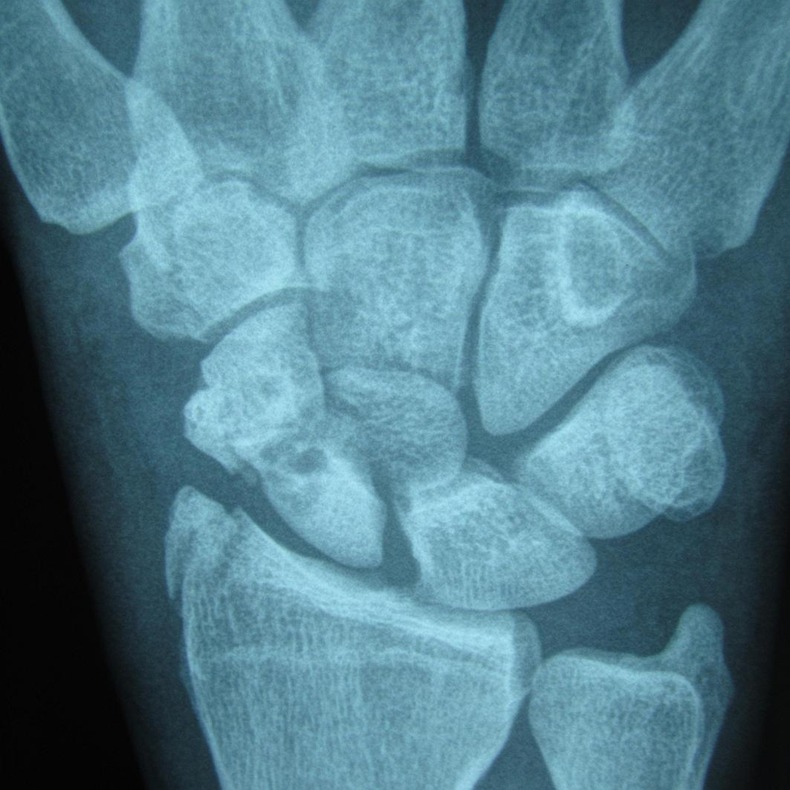
Radiograph demonstrating a transstyloid, transscaphoid, transcapitate fracture.
Figure 2.

CT scan (sagittal) showing rotation of the proximal fragment of the capitate.
Treatment
The patient underwent open reduction, bone grafting and internal fixation of the scaphoid fracture and open reduction and internal fixation of the capitate fragment (figure 3). The position of radial styloid fracture fragment was anatomical and so it was not fixed.
Figure 3.

Postoperative radiograph following anatomical reduction and open reduction and internal fixation.
Outcome and follow-up
At 1 year following surgery, the fracture sites had radiologically healed. The patient was pain free and had a full range of movement after a course of physiotherapy.
Discussion
A transstyloid, transscaphoid, transcapitate fracture is an osseous injury involving the carpal bones which has not been previously published in the literature. The mechanism of injury for this patient was direct trauma. Scaphocapitate fractures can occur following a fall with the wrist extended. The compressive forces cause the scaphoid to fracture. The impaction of the posterior aspect of the radius on the neck of the capitate during hyperextension of the wrist causes the capitate to fracture.6–8 This injury pattern is similar to a greater arc injury which involves a fracture of the perilunate bones, as the energy dissipated through the scaphoid and capitate.9 Appropriate imaging is necessary to adequately evaluate the extent of injury and position of the fracture fragments prior to treatment.
It is important to treat this fracture appropriately as long-term pain and functional deficit can develop secondary to post-traumatic arthritis, avascular necrosis of the capitate or non-union.6 Anatomical reduction of the scaphoid and midcarpal joint prevents carpal instability and arthrosis,10 as the restoration maintains carpal alignment and allows for the healing of the ligamentous structures.
Internal fixation allows for early mobilisation of the wrist joint, which is associated with a good functional outcome, as demonstrated by this patient. Delayed treatment may result in a salvage procedure such as a proximal row carpectomy or wrist arthrodesis being performed. This case is a variant of the scaphocapitate fracture that involves a fracture of the radial styloid. It also highlights the need for early surgical intervention for fractures of the capitate with significant rotation of proximal fragment to ensure a satisfactory clinical outcome.
Learning points.
A transstyloid, transscaphoid, transcapitate fracture is a traumatic injury which needs to be carefully assessed clinically and radiologically.
Early operative intervention and mobilisation is key to a good outcome.
Delayed intervention may result in post-traumatic arthritis, avascular necrosis of the capitate or non-union.
Footnotes
Contributors: NGB wrote the case report. CHC provided the images and proof read and edited the case report. BJON proof read and edited the case report. EPK is the consultant in overall charge of the case, and edited and approved the final draft of the case report.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Fenton RL. The naviculo-capitate fracture syndrome. J Bone Joint Surg Am 1956;38-A:681–4 http://www.ncbi.nlm.nih.gov/pubmed/13319423 [cited 27 Jan 2014] [PubMed] [Google Scholar]
- 2.Rand JA, Linscheid RL, Dobyns JH. Capitate fractures: a long-term follow-up. Clin Orthop Relat Res 1982;209–16 http://www.ncbi.nlm.nih.gov/pubmed/7075062 [cited 27 Jan 2014] [PubMed] [Google Scholar]
- 3.Kuderna H. [Fractures and dislocation fractures of the wrist joint]. Orthopade 1986;15:95–108 http://www.ncbi.nlm.nih.gov/pubmed/3714271 [cited 27 Jan 2014] [PubMed] [Google Scholar]
- 4.Robbins M, Nemade A, Chen T, et al. Scapho-capitae syndrome variant: 180-degree rotation of the proximal capitate fragment without identifiable scaphoid fracture. Radiol Case Rep 2008;:193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Steffens K, Luce S, Koob E. [Unusual course of scapho-capitate syndrome]. Handchi Mikrochi Plast Chir 1994;26:12–14 http://www.ncbi.nlm.nih.gov/pubmed/8150380 [cited 27 Jan 2014] [PubMed] [Google Scholar]
- 6.Boisgard S, Bremont JL, Guyonnet G, et al. [Scapho-capitate fracture. Apropos of a case, review of the literature]. Ann Chir Main Memb Super 1996;15:181–8 http://www.ncbi.nlm.nih.gov/pubmed/8924343 [cited 27 Jan 2014] [DOI] [PubMed] [Google Scholar]
- 7.Adler JB, Shaftan GW. Fractures of the capitate. J Bone Joint Surg Am 1962;44-A:1537–47 http://www.ncbi.nlm.nih.gov/pubmed/14040732 [cited 27 Jan 2014] [PubMed] [Google Scholar]
- 8.Monahan PR, Galasko CS. The scapho-capitate fracture syndrome. A mechanism of injury. J Bone Joint Surg Br 1972;54:122–4 http://www.ncbi.nlm.nih.gov/pubmed/5011738 [cited 27 Jan 2014] [PubMed] [Google Scholar]
- 9.Dawson J, Fitzpatrick R, Murray D, et al. Comparison of measures to assess outcomes in total hip replacement surgery. Qual Health Care 1996;5:81–8 http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1055370&tool=pmcentrez&rendertype=abstract [cited 16 Oct 2013] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Amaravati RS, Saji MJ, Rajagopal HP. Greater arc injury of the wrist with fractured lunate bone: a case report. J Orthop Surg (Hong Kong) 2005;13:310–13 http://www.ncbi.nlm.nih.gov/pubmed/16365499 [cited 27 Jan 2014] [DOI] [PubMed] [Google Scholar]