

Abstract
The purpose of this study was to determine pillow designs suitable for supine and side-lying positions. [Subjects] Twenty female and twenty male subjects with a mean age of 22.7 years (SD = 1.3) participated in the study. [Methods] First, a three-dimensional motion analysis system was used to analyze the movements of the head and the shoulder joints during changes from supine positions to side-lying positions. Second, the height from the face to the shoulder and the height from the floor to the middle of the neck in a side-lying position were measured. Third, the weight distribution ratios of the head and the trunk were compared using general pillows (polyester sponge), memory foam, and prototype pillows. [Results] During position changes from supine positions to side-lying positions, the head moved in a fan shape, and the shoulder joint moved an average of 4.4 cm upward. The height from the face to the shoulder was 9 cm on average. The height from the floor to the middle of the neck was 11 cm on average. The weight distribution ratios between the head and the trunk were compared among general pillows (polyester sponge), memory foam, and prototype pillows. The results showed significant differences in the side-lying position. [Conclusion] Pillows with uniform heights are not suitable for a supine or side-lying position. In the case of both positions, users should be allowed to select pillows in shapes that can support the neck.
Key words: Pillow, Sleep position, Motion analysis
INTRODUCTION
Sleeping is an activity that accounts for 1/3 of daily living and is the longest activity in which we engage. Ideally, each adult should get a minimum of 7–8 hours of sleep per night to maintain optimum body functions and health1). While sleeping, the human body maintains homeostasis, and the brain forms the pathways necessary for learning, creating memories, and realizing new insights2). A lack of sleep impairs daytime functioning3). Those who cannot sleep sufficiently tend to have more mood problems, reduced cognitive ability, and increased fatigue and physical discomfort compared with those who sleep normally4).
Stress and musculoskeletal discomfort are major causes of lack of sleep5, 6). Musculoskeletal discomfort that disturbs sleep frequently includes neck pain. Although incorrect sleep postures can aggravate pain, the use of an appropriate pillow can relieve neck pain7). The role of pillows is to support the cervical spine during sleep so that it can be maintained in a neutral positions. In supine positions, normal spine curves should be maintained, and in side-lying positions, the cervical and thoracic portions of the spine should be aligned with each other so that there is no muscle stiffness and no excessive load is imposed on the facet joint8, 9). If a person with cervical pain uses a pillow that can support his/her neck, his/her quality of sleep can be enhanced10,11,12,13).
Some previous studies on pillows have examined comfort in relation to the types and shapes of pillows. The comfort and distribution of the head’s weight of water-based pillows significantly improved the quality of sleep and relieved cervical pain14). In another study, the degree of comfort was examined when one or a combination of two or more of four types of pillows currently available on the market were used. The results showed individual differences in comfort. Such studies suggest that pillow selection is largely a matter of personal preference13). Some studies have recently also examined whether a relationship exists between cervical lordosis curves, neck girths, and lateral neck lengths and pillow sizes. Pillows were made in four sizes with differences in the heights of the central region and both edges. Their central regions were designed to be 5–8 cm high, and both edges were designed to be 10–11 cm high. When subjects with asymptomatic cervical spines and subjects with organic pathology within the cervical spine used the pillows they preferred among these four sizes, their pain and neck disability indexes significantly decreased and their quality of sleep was significantly improved15,16,17). Not only did the quality of sleep improve, but the subjects’ pain was also relieved with the use of appropriate pillows; however, the pillow designs were not explained. Studies conducted thus far have not considered that people change their positions while they sleep, allowing them to take not only supine positions but also side-lying positions. Pillows currently on the market are too high for supine positions and too low for side-lying positions. Therefore, the purpose of this study was to examine position changes during sleep, to design pillows that could support the neck both in supine and side-lying positions, and to provide the results as reference data for pillow designs.
SUBJECTS AND METHODS
The subjects of this study were 40 normal persons (20 women, 20 men; mean age, 22.7 ± 1.3 years) who agreed to participate in the experiment after an explanation of its contents, its risks, and its benefits. The mean values (mean and standard deviation) for subject’s mass and height were 62.6 ± 10.8 kg and 166.1 ±10.4 cm, respectively. This study was approved by the university research and development review board for human subjects. The entire procedures conformed to the Declaration of Helsinki.
First, six three-dimensional motion analysis cameras (Qualisys AB, Gothenburg, Sweden) were used to analyze head and shoulder joint movements during natural direction changes from supine positions to side-lying positions without any conscious cervical flexion or extension. The axis of movement was the pelvis or the lower extremities. The sampling frequency was set to 100 Hz, and 25 reflective makers were attached to certain points of the body that served as anatomical landmarks for each subject. The markers measured using the cameras were checked using the Qualisys Track Manager program, and data were analyzed using a biomechanics analysis program (Visual 3D). Second, the height from the face to the shoulder and the height from the floor to the middle of the neck were measured. Third, a 23 × 9.5-cm-sized air bag was built in the region that would contact the neck to design a pillow that would allow the subjects to determine the most suitable pressure for them. Thereafter, the pressure necessary to maintain the normal cervical lordosis angles of 30–35° and the pressure that felt the most comfortable were measured. To check whether the normal cervical lordosis angles were maintained, X-ray images were taken through lateral projection while increasing the pressure by 20 mmHg at a time from 0 mmHg to 100 mmHg. Fourth, to examine the degree to which the pillow supported the neck in side-lying positions, the indexes of body weight distribution between the head and the trunk were compared using general pillows (polyester sponge), memory foam, and prototype pillows (Fig. 1). General pillows (polyester sponge) 50 × 38.7 × 11.5 cm in size and memory foam pillows 49 × 32 × 10 cm in size were used. Two force plates (Kistler 9260AA6, Kistler Instrumente AG, Winterthur, Switzerland) were used; the head was placed on one (F1) of the force plates, and the trunk was placed on the other force plate (F2). In side-lying positions, the acromion was placed on the edge of the force plate (F2) on which the trunk was placed, and changes in body weight were measured and analyzed for each force plate when the subject was in a side-lying position using the pillow. The index of body weight distribution was calculated using the following formula: [vertical force of F1 / (vertical force of F2 + vertical force of F1)] × 100 (%). Larger calculated values mean better support for the head by the pillow, with greater weight distributed to the head side.
Fig. 1.
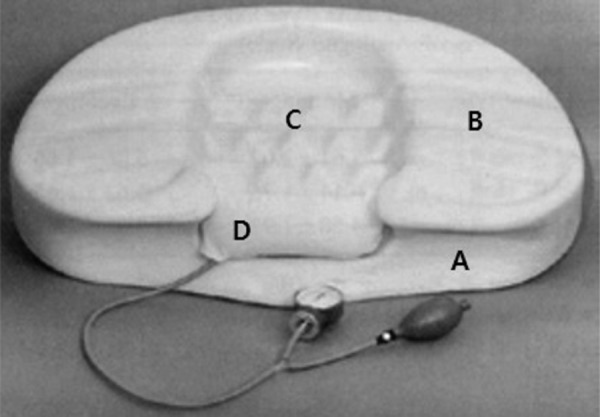
Prototype pillow A: An indent was made in the part of the surface of the pillow that contacted the shoulder in side-lying positions. B: The height from the face to the shoulder. C: The height from the floor to the middle neck. D: 23 × 9.5-cm air bag was built.
All data were statistically analyzed using PASW 18.0, and the analysis of the general characteristics of the subjects incorporated descriptive statistics. Repeated measures ANOVAs were used to compare weight distribution ratios between pillows, and post hoc tests were conducted using the Bonferroni method. The statistical significance level was 0.05.
RESULTS
Figure 2 shows head movements during a direction change from a supine position to a side-lying position. When the axis of movement was the pelvis and the lower leg, the head moved in a fan-shaped manner. The distance of movement of the shoulder joint along the Y-axis was 4.4 cm, on average (average of 20 females 3.1 cm, average of 20 males 5.7 cm).
Fig. 2.

Head movement trajectory during movement from the supine to side-lying position
The height from the face to the shoulder was 9 cm, on average. The height from the floor to the middle neck was 11 cm on average.
The pressure necessary to maintain the normal cervical lordotic curvature of 30–35° was 80–100 mmHg in the largest number of cases (n=18, 45%) (Table 1). The pressure that felt the most comfortable was diverse among the subjects and ranged from 0 to 90 mmHg, although 20–40 mmHg was selected by the largest number of subjects (n=20, 50%) (Table 2).
Table 1. Pressure to induce normal lordotic curve.
| Pressure | Number |
| 0–20 mmHg | 3 (7.5) |
| 20–40 mmHg | 5 (12.5) |
| 40–60 mmHg | 9 (22.5) |
| 60–80 mmHg | 5 (12.5) |
| 80–100 mmHg | 18 (45) |
Values are numbers (%)
Table 2. Most comfortable pressure in supine position.
| Pressure | Number |
| 0–20 mmHg | 2 (5) |
| 20–40 mmHg | 20 (50) |
| 40–60 mmHg | 7 (17.5) |
| 60–80 mmHg | 6 (15) |
| 80–100 mmHg | 4 (10) |
Values are numbers (%)
The weight distribution ratios between the head and the trunk were compared among general pillows (polyester sponge), memory foam, and prototype pillows. According to the results, the ratio was the smallest in the case of general pillows at 11.38 ± 1.51, followed by memory foam pillows at 13.93 ± 1.20, and prototype pillows at 18.1 ± 3.46; these differences were significant (Table 3).
Table 3. Effect of pillow type on weight distribution.
| Pillows | Ratio |
| Prototype pillow | 18.1±3.462,3 |
| Memory foam | 13.93±1.201,3 |
| Polyester sponge | 11.38±1.511,2 |
1Significant difference as compared with the prototype pillow. 2Significant difference as compared with memory foam. 3Significant difference as compared with polyester sponge.
DISCUSSION
The best sleep position is one in which the normal cervical curve is maintained. In supine positions, the normal cervical lordotic curvature should be maintained, and in side-lying positions, the cervical spine should be aligned with the thoracic spine8, 16). The intent in this study was to analyze head and shoulder joint movements, anthropometry, and weight distribution ratios between the head and the trunk in relation to position changes to determine pillow designs that can sufficiently support the neck in both positions.
During direction changes from supine positions to side-lying positions, the head movement trajectories were fan shaped. Based on this result, pillows were designed in pillow shapes because the head and the neck move downward in fan shapes instead on moving horizontally during direction changes from supine positions to side-lying positions. General pillows (polyester sponge) and memory foam pillows are designed so that the head and the neck move horizontally. If the neck and the head move from the pillow such that the pillow cannot sufficiently support the neck, muscle tone may occur in the neck. During direction changes from supine positions to side-lying positions, the shoulder joint was observed to move upward. Based on this result, an indent was made in the surface of the pillow that contracted the shoulder in side-lying positions.
The height from the face to the shoulder and the height from the floor to the middle of the neck were measured. The pillow was designed such that the height from the face to the shoulder was larger than the height from the floor to the middle of the neck. The intention of this was to maintain normal cervical lordosis in both supine positions and side-lying positions.
To maintain normal cervical lordosis and support the neck in supine positions, a 23 × 9.5-cm airbag was embedded in the region that contacts the neck. This air bag was placed perpendicular to the joint line of the cervical spine to induce traction to the facet joint when pressure increases. The pressure necessary to maintain the normal cervical lordosis and the pressure that felt the most comfortable to the subjects differed from each other and varied among individuals. The pillow was designed so that the air bag pressure could be adjusted by the user to the height that felt the most comfortable, as well as so that the height from the floor to the middle of the neck could be adjusted.
The ratios of weight distribution between the head and the trunk in a side-lying position were compared among pillow types, and according to the results, the prototype pillows showed the highest distribution ratios. The ratios of weight distribution increased when the weight on the side of the head increased. That is, the weight on the side of the head increased because the pillow sufficiently supported the neck. The indentation in the part of the surface of the pillow that contacts the shoulder in side-lying positions is considered to have helped the pillow in supporting the neck by preventing the neck from being pushed upward or downward. This study can be recommended the design of pillow based on this experiment.
REFERENCES
- 1.National Sleep Foundation: Summary of the sleep in America poll. 2009
- 2.Krueger JM, Obál F, Jr, Fang J: Why we sleep: a theoretical view of sleep function. Sleep Med Rev, 1999, 3: 119–129 [DOI] [PubMed] [Google Scholar]
- 3.Edinger JD, Bonnet MH, Bootzin RR, et al. : Derivation of research diagnostic criteria for insomnia: report of an American Academy of Sleep Medicine Work Group. Sleep, 2004, 27: 1567–1596 [DOI] [PubMed] [Google Scholar]
- 4.Kyle SD, Morgan K, Espie CA: Insomnia and health-related quality of life. Sleep Med Rev, 2010, 14: 69–82 [DOI] [PubMed] [Google Scholar]
- 5.Meerlo P, Sgoifo A, Suchecki D: Restricted and disrupted sleep: effects on autonomic function, neuroendocrine stress system and stress responsivity. Sleep Med Rev, 2008, 12: 197–210 [DOI] [PubMed] [Google Scholar]
- 6.Palermo TM, Wilson AC, Lewandowski AS, et al. : Behavioral and psychosocial factors associated with insomnia in adolescents with chronic pain. Pain, 2011, 152: 89–94 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gordon SJ, Grimmer-Somers K, Trott P: Pillow use: the behavior of cervical pain, sleep quality and pillow comfort in side sleepers. Man Ther, 2009, 14: 671–678 [DOI] [PubMed] [Google Scholar]
- 8.Cyriax PJ: Text book of Orthopedic Medicine, 8th ed. London: WB Saunders, 1988 [Google Scholar]
- 9.Liebenson C: Rehabilitation of the spine, 1st ed. Los Angeles: Williams & Wilkins, 1996 [Google Scholar]
- 10.Ambrogio N, Cuttiford J, Lineker S, et al. : A comparison of three types of neck support in fibromyalgia patients. Arthritis Care Res, 1998, 11: 405–410 [DOI] [PubMed] [Google Scholar]
- 11.Persson L, Moritz U: Neck support pillows: a comparative study. J Manipulative Physiol Ther, 1998, 21: 237–240 [PubMed] [Google Scholar]
- 12.Palazzi C, Miralles R, Miranda C, et al. : Effects of two types of pillows on bilateral sternocleidomastoid EMG activity in healthy subjects and in patients with myogenic cranio-cervical-mandibular dysfunction. Cranio, 1999, 17: 202–212 [DOI] [PubMed] [Google Scholar]
- 13.Liu SF, Lee YL, Liang JC: Shape design of an optimal comfortable pillow based on the analytic hierarchy process method. J Chiropr Med, 2011, 10: 229–239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lavin RA, Pappagallo M, Kuhlemeier KV: Cervical pain: a comparison of three pillows. Arch Phys Med Rehabil, 1997, 78: 193–198 [DOI] [PubMed] [Google Scholar]
- 15.Erfanian P, Hagino CC, Guerriero RC: Pilot study: an investigation of the relationship between external cervical measurements and the preference of cervical pillow thickness. J Can Chiropr Assoc, 1998, 42: 83–89 [Google Scholar]
- 16.Erfanian P, Hagino CC, Guerriero RC: A preliminary study assessing adverse effects of a semi-customized cervical pillow on asymptomatic adults. J Can Chiropr Assoc, 1998, 42: 156–162 [PMC free article] [PubMed] [Google Scholar]
- 17.Erfanian P, Tenzif S, Guerriero RC: Assessing effects of a semi-customized experimental cervical pillow on symptomatic adults with chronic neck pain with and without headache. J Can Chiropr Assoc, 2004, 48: 20–28 [PMC free article] [PubMed] [Google Scholar]