

Abstract
[Purpose] The effectiveness of intrinsic foot flexor strength training performed in the plantar flexion position was examined using needle electromyography. [Subjects] The subjects of this study were 18 healthy men. [Methods] We used needle electromyography to measure the muscle activities of the flexor hallucis brevis (FHB), and the flexor digitorum brevis (FDB) in maximum plantar and an intermediate position. [Results] Significant increases in muscle activities were observed for both FHB and FDB, and the rates of increase from the intermediate position to the plantar flexion position were 43% for FHB and 46% for FDB. [Conclusion] This study demonstrated that it is possible to evaluate intrinsic foot flexors, in addition to the numerous reports on treatment methods focusing on extrinsic foot flexors. Furthermore, the results suggest that toe flexion exercises performed during plantar flexion of the ankle joint are an effective method for intrinsic foot flexor strength training.
Key words: Intrinsic foot flexor muscles, Needle electromyography, Muscle activity
INTRODUCTION
Human feet function to directly absorb shock from the ground thereby insulating the body from impact, supporting body weight, and propelling the body. They make not only walking, but also running and jumping possible1,2,3,4,5,6,7,8,9).
Extrinsic foot flexors that cause toe flexion are the flexor hallucis longus and flexor digitorum longus. They are responsible for flexing the interphalangeal (IP) and metacarpophalangeal (MP) joints of the first toe, as well as the distal interphalangeal (DIP), proximal interphalangeal (PIP), and MP joints of the second through fifth toes. Intrinsic foot flexors that cause toe flexion are the flexor hallucis brevis and the flexor digitorum brevis. They are responsible for flexing the MP joint of the first toe, as well as the PIP and MP joints of the second through fifth toes.
The majority of studies on the treatment and prevention of foot injuries have focused on the recovery of arch function, prevention of flat foot, range of motion training for the sole and lower leg, and muscle stretching and strengthening10,11,12,13,14). All these treatment and prevention methods focus on extrinsic foot flexors, primarily because it is difficult to evaluate intrinsic foot flexors individually and separately during training.
The contractile force of intrinsic foot flexors, which is exerted in ankle plantar flexion, is evidenced by the anatomical structure of the muscles, observation and palpation during dynamic contraction, and findings regarding loss of flexion capability in the IP joint of the first toe, as well as the DIP joints of the second through fifth toes. Hayashi and Ukai et al. established a method for measuring the strength of intrinsic foot flexor muscles by considering ankle joint plantar flexion as a position that inhibits extrinsic flexion (Fig. 1)15,16,17).
Fig. 1.
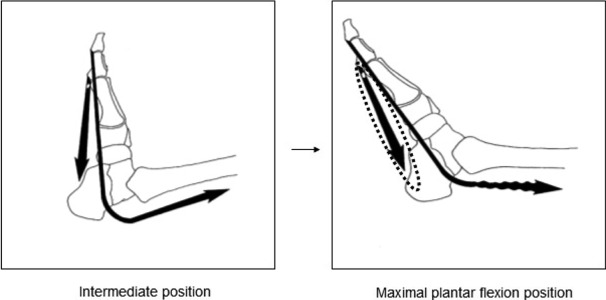
Differences in muscle activity as a result of the ankle joint position
A few studies have shown that intrinsic foot flexors are important for dynamic stabilization of the arches of the feet, enabling a more efficient exertion of extrinsic foot flexor muscle force and improving walking performance. However, the effects of training these muscles are still unclear18,19,20,21). In a previous study, we described a method of intrinsic foot flexor strength training to improve the full toe flexion gripping force of the MP joint of the first toe and the PIP and MP joints of the second through fifth toes. The ankle joint was secured in the maximum plantar flexion position, and 200 repetitions were performed thrice with a load of 3 kg over a period of 8 weeks. We found improvements in the strength of intrinsic flexor muscles, arch structure (the medial longitudinal arch and the transverse metatarsal arch in a static position), and dynamic performance (vertical jump, one-legged long jump, 50-m dash time)22). However, the extent of dependence of muscle activity on intrinsic foot flexors while performing toe flexion exercises with maximum plantar flexion position is still unclear. Therefore, the present study is significant, in that we examined the effectiveness of intrinsic foot flexor strength training performed in the plantar flexion position using highly reliable needle electromyography.
SUBJECTS AND METHODS
This study used needle electromyography to examine how different ankle positions, specifically the position between plantar flexion and dorsiflexion (hereafter, the intermediate position) and the maximum plantar flexion position (hereafter, the plantar flexion position), affect the activity levels of intrinsic foot flexor muscles. Secondary aim of this study was to demonstrate the effectiveness of intrinsic foot flexor strength training performed in the plantar flexion position.
After receiving approval from the Juntendo University Graduate School of Health and Sports Science Ethics Committee (Nos. 22-31), the purpose and content of this study were explained to participants, and their written consent was obtained.
The subjects were 18 healthy adult males with no history of physical injury. Their mean age, height, and weight (mean ± SD) were 31.6 ± 8.3 years, 170.9 ± 5.1 cm, and 65.2 ± 5.5 kg, respectively (Table 1).
Table 1. Characteristics of subjects.
| n=18 | |
| Age (years) | 31.6 ±8.3 |
| Height (cm) | 170.9 ± 5.1 |
| Weight (kg) | 65.2 ± 5.5 |
| BMI (kg/m2) | 22.3±1.7 |
Mean ± SD, BMI: Body Mass Index
Needle electromyography was performed with an evoked potential using an electromyograph (Neuropack MEB-2200, Nihon Kohden). The sampling frequency was 10 kHz, and EMG signals were converted to direct current by full wave rectification after filtering with a band-pass filter (10–5,000 Hz).
The activity levels the flexor hallucis brevis (FHB) and flexor digitorum brevis (FDB) were measured. Measurements were taken in the intermediate position and the plantar flexion position. A physician performed the measurements in accordance with an electromyography guide23).
A 10-kg tubular spring scale (Shinwa), which displays load values in the units of 0.1 kg, was used for measurements. The ankle joint was secured in the intermediate and maximal plantar flexion positions using a 50 × 14 × 60 cm 3wooden half-box stabilizer built for this study, and the tubular spring scale was secured to the box. Measurements were obtained in the intermediate and maximal plantar flexion ankle joint positions with the subjects in a long sitting position. To set up the initial position for the full toe flexion exercise, a finger sling (C7791, SAKAI) was perpendicularly attached to the proximal phalanx of each of the first through fifth toes in the intermediate position. Thereafter, the toes were elevated. It was confirmed that the load reached 3 kg when the MTP joint of the first toe and the PIP and MTP joints of the second through fifth toes were in the maximal flexion position before securing the foot in each position. After inserting needles into the muscles to be measured, 5-s isometric full toe flexion exercises were performed with a 3-kg load applied to the ankle joint in the intermediate and maximal plantar flexion positions. Measurements were performed on the left foot for a total of four times.
The activity levels of FHB and FDB in the two measurement positions were quantified as the one-second product (mVms). Wilcoxon’s signed rank test was used to determine the differences in mean muscle activity, rate of increase (%), and muscle activities of the FHB and FDB in the intermediate and maximal plantar flexion positions24, 25). p values <0.05 were considered significant. Statistical analyses were performed with SPSS version 18.0 (SPSS JAPAN Inc.).
RESULTS
Mean FHB muscle activity was 410.7 ± 255.1 mVms (median: 423.2) in the intermediate position and 997.1 ± 524.9 mVms (median: 870.4) in the maximal plantar flexion position. A significant increase in activity was observed (p < 0.001). The rate of increase from the intermediate position to the plantar flexion position was 43% (Table 2).
Table 2. FHB muscle activity in the intermediate and plantar flexion positions.
| FHB intermediate the one-second product (mVms) |
FHB maximal plantar flexion the one-second product (mVms) |
| 410.7±255.1 | 997.1±524.9*** |
FHB: flexor hallucis brevis, Mean ± SD, ***:p<0.001
Mean FDB muscle activity was 493.9 ± 297 mVms (median: 455.1) in the intermediate position and 1,215.3 ± 429.8 mVms (median: 1,096.5) in the plantar flexion position. A significant increase in activity was observed (p < 0.001). The rate of increase from the intermediate position to the plantar flexion position was 46% (Table 3).
Table 3. FDB muscle activity in the intermediate and plantar flexion positions.
| FDB intermediate the one-second product (mVms) |
FDB maximal plantar flexion the one-second product (mVms) |
| 493.9±297 | 1,215.3±429.8*** |
FDB: flexor digitorum brevis, Mean ± SD, ***:p<0.001
DISCUSSION
Studies have shown that intrinsic foot flexors support the transverse metatarsal and medial longitudinal arches, that they dynamically protect suspensory ligaments and joint tissue in the feet, and that excessive loads in the standing position, specifically loads over 400 lbs (1,780 N) while standing on one foot, increase their muscle activities26,27,28,29,30,31). While running, intrinsic foot flexors function to create a strong lever for ankle joint plantar flexion and are constantly active under the load of body weight while running at maximal speed. Furthermore, these muscles are an important factor in improving jumping ability32,33,34). However, detailed methods for assessing intrinsic foot flexors and the positions that yield effective activation have not yet been revealed.
In this study, needle electromyography was used to measure muscle activity, because intrinsic foot flexors are thin and deep muscles. Full toe flexion exercise was performed, but not all toes could be secured at the same angle. In addition, it was difficult to standardize the angle of toe flexion between the intermediate and the plantar flexion positions due to differences in the degree of extension of toe extensors. Therefore, to perform measurements in each position, the study conditions were the resistance position, resistance angle, identical load, and maximal toe flexion.
Our results show that the muscle activities of both FHB and FDB significantly increased between the intermediate and plantar flexion ankle joint positions. Toe flexion in the intermediate ankle joint position is within the same angular range of motor execution as standing or walking, and there is little intrinsic flexor muscle activity in this position due to support from ligaments and extrinsic foot flexors. However, toe flexion during plantar flexion of the ankle joint shortens the origin and insertion of extrinsic foot flexors, and plantar flexion torque is minimized in this position. This also decreases the active tension of extrinsic foot flexors, including that of the flexor hallucis longus, flexor digitorum longus, tibialis posterior, and peroneus longus that act during plantar flexion of the ankle joint and toe flexion exercises, and puts these muscles in a restrictive position34). Therefore, intrinsic foot flexors either contract easily or must contract to this position, and this is believed to increase muscle activity (Fig. 1).
It is essential the ankle joint should be in a plantar flexion position in movements that are faster than walking, such as running or jumping, as well as in movements used during sports. A sequence of movements associated with plantar flexion of the ankle joint secures and stabilizes the foot, compensates for decreased extrinsic flexor function, and creates propulsion.
In addition to the method outlined in our previous study, toe flexion exercises in a long sitting or supine position, a prone position that makes it easy to achieve maximal plantar flexion with body weight, a ital (a Japanese-style sitting) position, and a position in which toe flexion and ankle plantar flexion is maintained under controlled body weight with support from the arms are other methods for training intrinsic foot flexors with the ankle joint in a plantar flexion position. Increasing the load by an appropriate amount is also effective (Fig. 2).
Fig. 2.
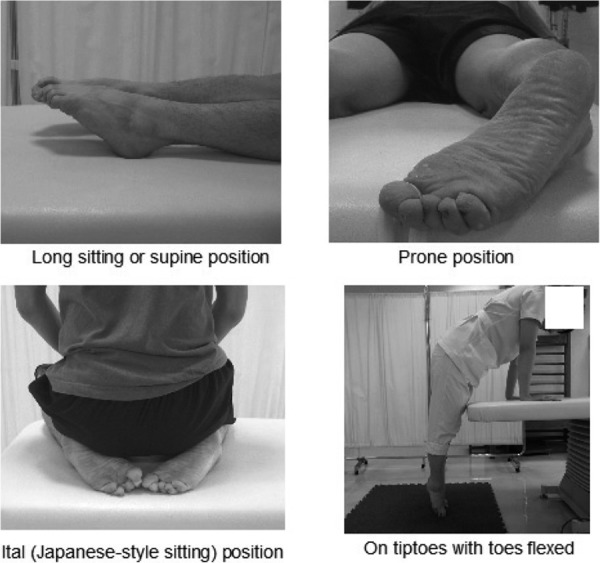
Positions for training the intrinsic foot flexor muscles
This study demonstrated that it is possible to evaluate intrinsic foot flexors, in addition to the numerous reports on treatment methods focusing on extrinsic foot flexors. Furthermore, the results suggest that toe flexion exercises performed during plantar flexion of the ankle joint are an effective method for intrinsic foot flexor strength training.
REFERENCES
- 1.Miyazaki K: Impact loading on the foot and ankle and its attenuation during level walking. Kurume Med J, 1998, 45: 75–80 [DOI] [PubMed] [Google Scholar]
- 2.Dixon PC, Böhm H, Döderlein L: Ankle and midfoot kinetics during normal gait: a multi-segment approach. J Biomech, 2012, 45: 1011–1016 [DOI] [PubMed] [Google Scholar]
- 3.Rouhani H: Ambulatory measurement of ankle kinetics for clinical applications. J Biomech, 2011, 44: 2712–2718 [DOI] [PubMed] [Google Scholar]
- 4.Lambrinudi C: Use and abuse of toes Postgrade. Med J, 1932, 8: 459–464 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hughes J, Clark P, Klenerman L: The importance of the toes in walking. J Bone Joint Surg Br, 1990, 72: 245–251 [DOI] [PubMed] [Google Scholar]
- 6.Stokes IA, Hutton WC, Stott JR, et al. : Foeces under the hallux valgus foot before and after surgery. Clin Orthop Relat Res, 1979, 142: 64–72 [PubMed] [Google Scholar]
- 7.Hutton WC, Dhanendran M: A Study of the distribution of load under the normal foot during walking. Int Orthop, 1979, 3: 153–157 [DOI] [PubMed] [Google Scholar]
- 8.Ctercteko GC, Dhanendran M, Hutton WC, et al. : Vertical Forces Acting on the Feet of Diabetic Patients with Neuropathic Ulceration. Br J Surg, 1981, 68: 608–614 [DOI] [PubMed] [Google Scholar]
- 9.Lieberman DE, Venkadesan M, Werbel WA, et al. : Foot strike patterns and collision forces in habitually barefoot versus shod runners. Nature, 2010, 463: 531–535 [DOI] [PubMed] [Google Scholar]
- 10.Morris JM: Biomechanics of the foot and ankle. Clin Orthop, 1977, 122: 10–17 [PubMed] [Google Scholar]
- 11.Hohmann G: Der Hallux Valgus und die vebrigen Zchenverkruemmungen. Ergeb Chir Orthop, 1925, 18: 308–376 [Google Scholar]
- 12.Groiso JA: Juvenile hallux valus. A conservative approach to treatment. J Bone Joint Surg, 1992, 74-A: 1367–1374 [PubMed] [Google Scholar]
- 13.Tanaka Y, Takakura Y, Kumai T, et al. : Radiographic analysis of hallux valgus. A two dimensional coordinate system. J Bone Joint Surg, 1995, 77: 205–213 [DOI] [PubMed] [Google Scholar]
- 14.Ihara H, Miwa M, Takayanagi K: Dynamic joint control training for knee ligament injuries. Am J Sports Med, 1986, 14: 309–315 [DOI] [PubMed] [Google Scholar]
- 15.Hayashi N, Ukai T, Ohtake N, et al. : The relationship between the metatarsal arch and toe flexor strength. Hakkai Seikei Geka Rihabiriteishon Kenkyuukaishi. 2000, 6: 9–12 [Google Scholar]
- 16.Hayashi N, Ukai T, Hashimoto T, et al. : Effects of insole on the intrinsic flexor’s strength. Bull Jpn Soc Prosthet Orthot Educ Res Dev, 2000, 16: 94–95 [Google Scholar]
- 17.Ukai T, Hayashi N, Hashimoto T, et al. : Effects of the flexor digitorum longus on peroneus ongus activity. J 8th Cong Soc Rehab Orthopaedics. 2000, 6: 40–43.
- 18.Blanpied P, Smidt GL: The difference in stiffness of the active plantarflexors between young and elderly human females. J Gerontol, 1993, 48: M58–M63 [DOI] [PubMed] [Google Scholar]
- 19.Fiolkowski P, Brunt D, Bishop M, et al. : Intrinsic pedal musculature support of the medial longitudinal arch: an electromyography study. J Foot Ankle Surg, 2003, 42: 327–333 [DOI] [PubMed] [Google Scholar]
- 20.Neptune RR, Sasaki K: Ankle plantar flexor force production is an important determinant of the preferred walk-to-run transition. J Exp Biol, 2005, 208: 799–808 [DOI] [PubMed] [Google Scholar]
- 21.Wu L: Nonlinear finite element analysis for musculoskeletal biomechanics of medial and lateral plantar longitudinal arch of Virtual Chinese Human after plantar ligamentous structure failures. Clin Biomech (Bristol, Avon), 2007, 22: 221–229 [DOI] [PubMed] [Google Scholar]
- 22.Hashimoto T, Sakuraba K: Intrinsic foot flexor strength training: verifying the effects on strength, foot arch, and dynamic test items. Jpn J Orthop Sports Med. 2011, 31: 149–154 [Google Scholar]
- 23.Perotto AO: Anatomical Guide for the Electromyographer: The Limbs and Trunk. Charles C, ed. Thomas Publisher, 2005, pp 120–124. [Google Scholar]
- 24.O’Sullivan PB, Dankaerts W, Burnett AF, et al. : Effect of different upright sitting postures on spinalpelvic curvature and trunk muscle actiation in a pain-free population. Spine, 2006, 31: E707–E712 [DOI] [PubMed] [Google Scholar]
- 25.Bjerkefors A, Ekblom MM, Josefsson K, et al. : Deep and superficial abdominal muscle activation during trunk stabilization exercises with and without instruction to hollow. Man Ther, 2010, 15: 502–507 [DOI] [PubMed] [Google Scholar]
- 26.Ukai T, Hayashi N, Hashimoto T, et al. : The effects of taping on stride length. Rigaku Ryohougaku, 2000, 27: 217 [Google Scholar]
- 27.Cavanagh PR, Rodgers MM, Liboshi A: Pressure distribution under symptom-free during barefoot standing. Foot Ankle, 1987, 7: 262–276 [DOI] [PubMed] [Google Scholar]
- 28.Umeki Y: Static results of medial foot arch. J Jpn Orthop Assoc, 1991, 65: 41–51 [PubMed] [Google Scholar]
- 29.Basmajian JV, Stecko G: The role of muscles in arch support of the foot. J Bone Joint Surg Am, 1963, 45: 1184–1190 [PubMed] [Google Scholar]
- 30.Thordarson DB, Schmotzer H, Chon J, et al. : Dynamic support of the human longitudinal arch: a biomechanical evaluation. Clin Orthop Relat Res, 1995, 316: 165–172 [PubMed] [Google Scholar]
- 31.Suzuki R: Functional of the leg and foot muscles from the viewpoint of the electromyogram. J Jpn Orthop Surg Soc, 1956, 30: 67–78 [Google Scholar]
- 32.Rabita G, Couturier A, Lambertz D: Influence of training background on the relationships between plantarflexor intrinsic stiffness and overall musculoskeletal stiffness during hopping. Eur J Appl Physiol, 2008, 103: 163–171 [DOI] [PubMed] [Google Scholar]
- 33.Mann RA, Hagy DL, Dyski M: The function of the toes in walking, jogging and running. Clin Orthop Relat Res, 1979, 142: 24–29 [PubMed] [Google Scholar]
- 34.Nistor L, Markhede G, Grimby G: A technique for measurements of plantar flexion torque with the Cybex dynamometer. Scand J Rehabil Med, 1982, 14: 163–166 [PubMed] [Google Scholar]