

Abstract
Introduction:
Influenza A/H1N1 pandemic has recently threatened the health of world's population more than ever. Non-pharmaceutical measures are important to prevent the spread of influenza A/H1N1 and to prevent a pandemic. Effective influenza pandemic management requires understanding of the factors influencing preventive behavioral. This study reports on predictors of students’ preventive behaviors for pandemic influenza A/H1N1 using variables based on the protection motivation theory (PMT).
Materials and Methods:
In a cross-sectional study, multiple-stage randomized sampling was used to select 300 female students in Isfahan who completed a questionnaire in December 2009. Data were collected using a self-report questionnaire based on PMT. The statistical analysis of the data included bivariate correlations, Mann-Whitney, Kruskal-Wallis, and linear regression.
Results:
The mean age of participants was 15.62 (SE = 1.1) years old. Majority of participants were aware regarding pandemic influenza A/H1N1 (87.3%, 262 out of 300). Results showed that, protection motivation was highly significant relationship with preventive behavior and predicted 34% of its variance. We found all of the variables with the exception of perceived susceptibility, perceived severity, and response cost were related with protection motivation and explained 22% of its variance.
Conclusion:
Promotion of students’ self-efficacy, and intention to protect themselves from a health threat should be priorities of any programs aimed at promoting preventive behaviors among students. It is also concluded that the protection motivation theory may be used in developing countries, like Iran, as a framework for prevention interventions in an attempt to improve the preventive behaviors of students.
Keywords: Influenza A/H1N1, preventive behaviors, protection motivation theory
INTRODUCTION
Nowadays, the spread of infectious diseases across the globe is an important health issue in the society.[1] Respiratory infections are of great importance because of their rapid and extensive spread and their role in mortality of children, adolescents and adults.[2] Influenza A/H1N1 is a highly contagious respiratory disease that it is currently the greatest pandemic disease threat to humankind. This disease affected a large percent of the population with significant morbidity and mortality.[3,4]
According to Center of Disease Control (CDC), signs and symptoms of influenza A/H1N1 are the same as those of seasonal influenza including fever, cough, sore throat, body pain, headache, lethargy, and fatigue. Some people have digestive symptoms like diarrhea, and nausea.[5,6] One of the concerns of public health is the highly contagious nature of influenza, and its consequent epidemic of disease and death.[7] According to the WHO (2009), current evidence suggests that the main route of human-to-human transmission of the new Influenza A/H1N1 virus is via respiratory droplets, which are expelled by speaking, sneezing or coughing.[8] The probability of transmission through tear or saliva is not certain yet, but all respiratory secretions and fluids of the patients are potentially contaminating. The duration of transmission of this virus is like seasonal influenza. In fact the disease is contagious one day before until 7 days after onset of symptoms.[9,10,11]
During the pandemic Influenza A/H1N1, preventive behaviors such as face mask use, washing hands, using a tissue when coughing or sneezing, and avoid closely mixing with patients with Influenza-like symptoms have been suggested to be effective in the prevention of the pandemic.[12]
At risk people are those over 65-years old, children aged less than 5-years old, pregnant women, persons with chronic diseases and students.[13,14] On May 2009, more than 700 schools in the US were closed for health reasons. Schools must be prepared a range of threat and hazards and develop plans that address a variety of situation (US Dept. of Education, 2009) cited from CDC 2009.[13]
A greater understanding of the factors associated with preventive behavior pandemic influenza among students is required to inform communication strategies that promote improved preparedness for a pandemic.[13,15] We examined the determinant factors of preventive behaviors with used protection motivation theory (PMT), that it has been widely used in health behavior research and interventions. It was originally (Rogers, 1975) in order to better understand fear appeals and how people to protect themselves from a health threat.[16] It has two assessment stages of threat appraisal (perceived sensitivity, perceived severity, and perceived rewards), and coping appraisal (perceived self-efficacy, perceived response, and perceived costs) and fear, that the outcome of these two stages is protection motivation (intention to protect) and behavior.[17] Several previous studies have investigated protective health behaviors of influenza with used protection motivation theory.[18,19] Jiang et al. conducted a study about preventive behaviors to fight against SARS disease using protection motivation theory, and showed that perceived threat and perceived response efficacy regarding the SARS preventive behavior was the most important predictor.[20] Valigosky showed that components of PMT are weak predictors of preventive behavior in infectious diseases.[21] Any studies about perception or preventive behaviors for pandemic influenza with used this theory have not been reported in Iran. Therefore, we explored perception and performance of preventive behaviors for pandemic influenza in female high school students based on protection motivation theory (PMT) in Isfahan, Iran.
MATERIALS AND METHODS
This cross-sectional study was conducted on 300 female high school students of Isfahan in December 2009. Sampling was multi-stage random. There were a total of two high schools for female students in region 4 of Isfahan, which were chosen in the present study. Overall of 6 classes were randomly selected, and then the students were randomly chosen for participating in the present study. The principals of these schools were explained about the objectives of the study and informed consent was obtained from them. The research was approved by the Ethics Committee of the Isfahan University of Medical Sciences. After obtaining permission from education office, questionnaires were given to students. A panel of experts, consisting of 5 scholars in the areas of health behavior, health education, and infectious diseases reviewed and assessed the questions. The feedback from the panel of experts, which was mostly regarding the wording and phrasing of questions, was used to revise and modify the instrument. The final questionnaire was pilot-tested among a sub group of students before the starting of the main study. The data were used to estimate the internal consistency of the scales, using Cronbach's coefficient alpha.
The first section, socio-demographic information was collected for age, students’ grade, parents’ education, parents’ occupational, and annual household income. The second section, 40 statements were created to reflect and capture the PMT constructs. Four items were used to measure perceived sensitivity that for this variable an alpha coefficient of. 58 was reported. Three items were used to measure perceived severity that an alpha coefficient for this scale was 0.63. Response efficacy was assessed by six items that an alpha coefficient of 70 was reported. Self-efficacy was measured by five items that internal reliability was good (α = 0.82). Response cost was assessed by four items that for this variable an alpha coefficient of 0.56 was reported. Rewards were measured by three questions items that an alpha coefficient of 0.70 was reported. Fear was measured by three items that an alpha coefficient for this scale was 0.78. Protection motivation was measured by six items that internal reliability was good (α= 0.86). All questions, except for preventive behaviors were scored on 5-point likert scale ranging from 1(strongly disagree) to 5 (strongly agree). Preventive behavior was assessed by six items (α = 0.80) and using a 4-point scale (1, never; 2, sometimes (2-3 times a day); 3, often times (5 times a day); 4, always).
Statistical analysis was done using SPSS[14] software. Descriptive statistics were used to examine demographic characteristics and study variables. Mann-Whitney and Kruskal-Wallis were done to determine difference in preventive behaviors according to demographic variable categories. Correlation analysis was used to examine the simple association between study variables. Linear regression tests to evaluate how well perceived sensitivity, perceived severity, rewards, self-efficacy, perceived response, and perceived costs predicted the variance in both protection motivation and preventive behaviors. Before doing statistical testes, normal distribution of quantitative variables was evaluated and confirmed.
RESULTS
Students had a mean age of 15.62 ± 1.1 years with the highest frequency for 15-year-olds (32.7%; n = 98), and 16-year-olds (30.3%; n = 91). Most parents were high school dropouts (fathers, 53.7%; n = 161, and mothers, 62.7%; n = 188). Most fathers were self-employed (44.3%; n = 133), and most mothers were housewives (89.3%; n = 268). The main sources of information about influenza A/H1N1 were radio and TV (76.3%), family (37.3%), poster (35%), friends (25.3%); only 20% had received health information from health workers.
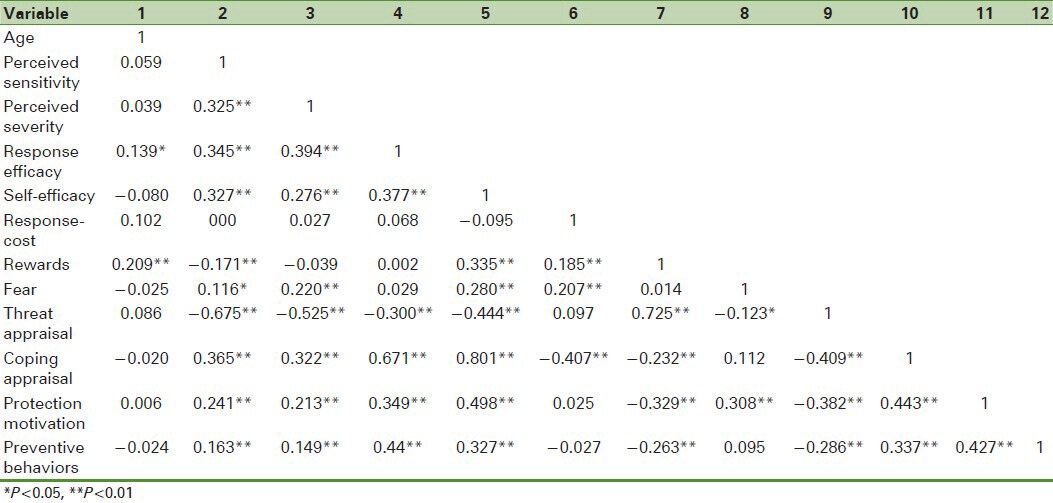
A summary of the means and standard deviation and Spearman's correlation matrix for all variables are present in Tables 1 and 2.
Table 1.
Descriptive statistics
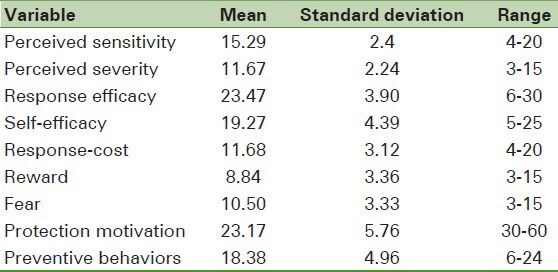
Table 2.
Spearman's correlation matrix of all variables
Almost all the participants, (74%; n = 222) reported that they always washed their hands with soap and water, and (69.7%; n = 209) always used a tissue when sneezing and coughing, (53.7%; n = 161) kept a distance of at least 1 meter away from suspected people, and (50%; n = 150) avoided contact with sick people.
The significant relationship was between fathers’ job and perceived sensitivity (P = 0.016). Perceived sensitivity in students whose fathers were jobless was higher. Furthermore, mothers’ job was significantly related with preventive behaviors (P = 0.027). Preventive behaviors were more in students whose mothers were housewives. We found moderate association between mothers’ higher education and obtain information about influenza A/H1N1 (P = 0.033). Furthermore, a significant relationship was found between obtain information and self-efficacy (P < 0.001), protection motivation (P = 0.006) and behavior (P = 0.47).
Using the PMT as a guide, a hierarchical regression was conduct. As seen in Figure 1, perceived sensitivity, perceived severity, response efficacy, self-efficacy, response-cost, reward, and fear together explained 22.8% of the variance protection motivation. Response efficacy, self-efficacy, reward, and fear were related to protection motivation, whereas perceived sensitivity, perceived severity, and response-cost were not related. The strongest predictor was response efficacy (β = 0.208) and self-efficacy (β = 0.200). Only reward toward not taken preventive behavior was a significant negative predictor of protection motivation and the other components had high and moderate statistically significant positive association with protection motivation directly. In predicting behavior, Figure 1 shows that protection motivation and PMT predicted 35.8% of the variance in behavior. Protection motivation, response efficacy, self-efficacy, and reward were significant predictors of behavior. The strongest predictor was protection motivation. In predicting protection motivation, Figure 2 shows that threat appraisal and coping appraisal predicted 14.4% of the variance in protection motivation. Between them, the role of coping appraisal (β = 0.262) was more that of threat appraisal (β = -0.179). Threat appraisal, coping appraisal, and protection motivation together predicted 34.5% of preventive behaviors, where the role of protection motivation (β = 0.244) was more than that of coping appraisal (β = 0.224) and threat appraisal (β = -0.112).
Figure 1.
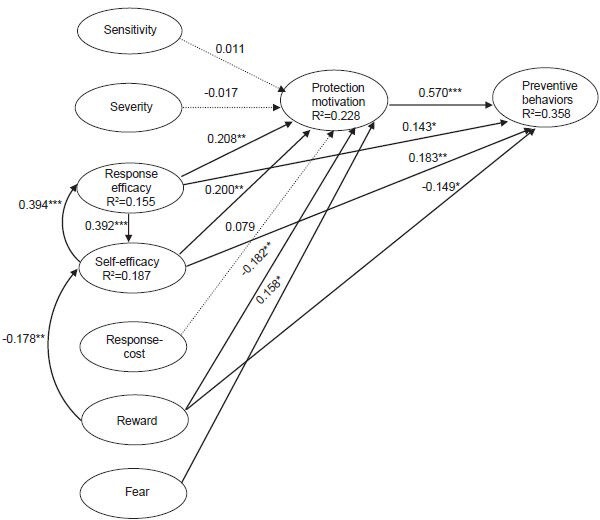
Presents the results from the path analysis which was conducted to examine the direct and indirect effects of the PMT components on the protection motivation and preventive behavior
Figure 2.
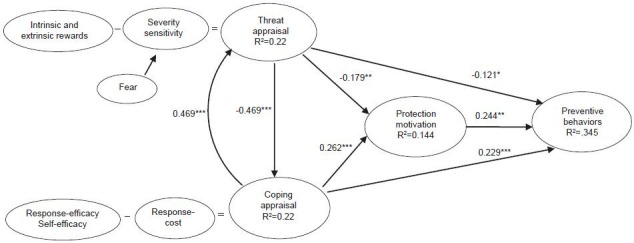
Presents the results from the path analysis, which was conducted to examining the effects two variables, threat appraisal and coping appraisal on the protection motivation and preventive behavior
DISCUSSION
The most commonly discussions at the time of H1N1 pandemics were of increasing preventive behaviors like frequent hand washing and using a tissue when sneezing and coughing.[22,23] In the present study, preventive behaviors were presented in the framework of PMT. In the present study, the total score of behavior was 77%, which is suitable. The most prevalent predictive behavior was frequent hand washing with soap and water. Rubin et al. reported that 40% of participants did preventive behaviors at the time of influenza A/H1N1 pandemics.[24] Akan et al. reported some preventive behaviors (washing hands and general hygiene) to be 53.5% among university students.[25] Van et al. found that 61.8% of the participants did not do any of the preventive behaviors, which is high as compared with our results.[26]
In line with PMT-relations, univariate results from the present study showed that perceived sensitivity and perceived severity were positively and significantly related. This finding contradicts the result of Kok et al.,[27] but corresponds with that of Park et al.,[22] and Valigosky.[23] The present study showed a strong and significant relationship between perceived severity and response efficacy in that people who had a higher perceived severity about the risks of influenza A/H1N1 reported higher response efficacy. McCool et al. found the same result in their study.[28]
The results of the present study showed a highly significant relationship of protection motivation with preventive behavior of influenza A/H1N1. This subject shows that if the person has more intension to do a behavior, the chances that he does the behavior are higher.
One of the stronger findings is that all variable in the protection motivation theory explained 22.8% of the variance in protection motivation and 35.8% of the variance in preventive behavior [Figure 1]. Both perceived severity and sensitivity are components of threat appraisal that in this study two components were small predicted of protection motivation. Furthermore, response efficacy and self-efficacy were the strongest predictions of protection motivation, which is in line with that of Barnett et al.[29] The effect sizes of such two components in previous meta-analyses were medium and barely predicted of protection motivation and behavior compared to the components of coping appraisal (response efficacy and self-efficacy).[30,31] Other studies showed that perceived efficacy of preventive behaviors of SARS, bird flu and swine flu were related with doing preventive behaviors.[32,33] We also find that self-efficacy was the second most important predictive of behaviour after protection motivation.
The present study coping appraisal predicted protection motivation and preventive behavior more than threat appraisal. Negative association was found for threat appraisal with protection motivation and preventive behavior. Grunfeld et al. expressed that threat appraisal and after that coping appraisal were stronger predictors of intention to perform safe sun exposure behaviors.[34]
One of the restrictions was difficulty in measuring the functioning because of using self-reporting questionnaire in this study. Moreover, studying only female students in one region of Isfahan is another restraint in this study. In attention people's attitude affected their behavior with regard to protecting themselves against influenza A/H1N1; it is recommended that attempt to improve people's performance in epidemics. The results of this study show the application of PMT in predicting behavior, so it can be used to devise training programs and interventional techniques to change attitude and behavior of students. The study points to issues that warrant attention in future prevention and preparedness efforts against influenza A/H1N 1.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Glass LM, Glass RJ. Social contact networks for the spread of pandemic influenza in children and teenagers. BMC Public Health. 2008;8:61. doi: 10.1186/1471-2458-8-61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chan PW, Chew FT, Tan TN, Chua KB, Hooi PS. Seasonal variation in respiratory syncytical virus chest infection in the tropics. Pediatr Pulmonol. 2002;34:47–51. doi: 10.1002/ppul.10095. [DOI] [PubMed] [Google Scholar]
- 3.World Health Organization Regional Office for Europe. [Last accessed on Oct 2009]. Available from: http://www.euro.who.int/influenza/AH1N1/20090611_11 .
- 4.Vaillant L, La Ruche G, Tarantola A, Barboza P. Epidemiology of fatal cases associated with pandemic H1N1 influenza 2009. Euro Surveill. 2009:14. doi: 10.2807/ese.14.33.19309-en. [DOI] [PubMed] [Google Scholar]
- 5.Picone O, Ami O, Vauloup-Fellous C, Martinez V, Guillet M, Dupont-Bernabe C, et al. Pandemic influenza A H1N1 2009 flu during pregnancy: Epidemiology, diagnosis and management. J Gynecol Obstet Biol Reprod (Paris) 2009;38:615–28. doi: 10.1016/j.jgyn.2009.09.016. [DOI] [PubMed] [Google Scholar]
- 6.2009 H1N1 Flu. Centers for Disease Control and Prevention. Novel H1N1 flu (swine flu) 2009. [Last accessed on 2012 Sep 14, Last cited 2009 Jun 26]. Available from: http://www.cdc.gov/swineflu/swineflu_you.html .
- 7.WHO, – Global Alert and Response—Pandemic (H1N1) 2009—Update 74, II Nov. 13. 2009. [Last accessed on 2009 Nov 13]. Available from: http://www.who.int/csr/don/2009_11_13/en/index.html .
- 8.The World Health Organizati on [WHO]. Pandemic influenza preparedness and response. Phase 5-6 Pandemic. 2009. [Last accessed on 2009 Aug 5]. Available from: http://www.who.int/csr/disease/influenza/piguidance 20091 en/index.html .
- 9.Mathematical modelling of the pandemic H1N1 2009. Wkly Epidemiol Rec. 2009;84:341–8. [PubMed] [Google Scholar]
- 10.WHO. Clinical Management of Pandemic (H1N1) 2009 Virus Infection, Interim Guidance from Expert Consultation [Online] 2009. [Last accessed on 14 Sep 2012, Last cited on 2009 Sep 17]. Available from: http://www.emro.who.int/csr/h1n1/pdf/clinical_management_guidelines.pdf .
- 11.WHO. WHO Guidelines for Pharmacological Management of Pandemic Influenza A (H1N1) 2009 and other Influenza Viruses [Online] 2010. Feb, [Last accessed on 2009 Oct]. Available from: http://www.who.int/csr/resources/publications/swineflu/h1n1_guidelines_pharmaceutical_mngt.pdf/Korea Center of Disease Control and Prevention . Available from: http://cdc.go.kr . [PubMed]
- 12.Cowling B1, Zhou Y, IP DKM. Epidemiology and Infection. Vol. 138. Cambridge: Cambridge University Press; 2010. Face mask to prevent transmission of influenza virus systematic review; pp. 499–456. [DOI] [PubMed] [Google Scholar]
- 13.United States Centers for Disease Control and Prevention. Interim guidance on case definitions to be used for investigations of novel influenza A (HINI) cases. [Last aaccessed on 2009 Jun 02]. Available from: www.cdc.gov/h1n1flu/casedef.htm .
- 14.Thorner AR. Treatment of pandemic HINI influenza (“swine influenza”) [Last accessed on 2009 Aug]. Available from: http://www.uptodate.com .
- 15.Centers for Disease Control and Prevention. HfNl Flu [online] [Last accessed on 2009 Jun 8]. Available from: http://www.cdc.gov/h1n1flu/update.htm .
- 16.Rogers RW. A protection motivation theory of fear appeals and attitude change. J Psychol. 1975;91:93–114. doi: 10.1080/00223980.1975.9915803. [DOI] [PubMed] [Google Scholar]
- 17.Milne S, Sheeran P, Orball SH. Prediction and intervention in Health-Related Behavior: A Meta-Analytic Review of Protection Motivation Theory. J Appl Soc Psychol. 2000;30:106–43. [Google Scholar]
- 18.Sadique MZ, Edmunds WJ, Smith RD, Meerding WJ, de Zwart O, Brug J, et al. Precautionary behavior in response to perceived threat of pandemic influenza. Emerg Infect Dis. 2007;13:1307–13. doi: 10.3201/eid1309.070372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Watkins RE, Cooke FC, Donovan RJ, MacIntyre CR, Itzwerth R, Plant AJ. Influenza pandemic preparedness: Motivation for protection among small and medium businesses in Australia. BMC Public Health. 2007;7:157. doi: 10.1186/1471-2458-7-157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jiang X, Elam G, Yuen C, Voeten H, de Zwart O, Veldhuijzen I, et al. The perceived threat of SARS and its impact on precautionary actions and adverse consequences: A qualitative study among Chinese communities in the United Kingdom and the Netherlands. Int J Behav Med. 2009;16:58–67. doi: 10.1007/s12529-008-9005-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Valigosky MA. Ohio: University of Toledo; 2009. Infection control perceptions and practices of spiritual care providers: An application of the protection motivation theory. [Google Scholar]
- 22.Park JH, Cheong HK, Son DY, Kim SU, Ha CM. Perceptions and behaviors related to hand hygiene for the prevention of H1N1 influenza transmission among Korean university students during the peak pandemic period. BMC Infect Dis. 2010;10:222. doi: 10.1186/1471-2334-10-222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lau JT, Griffiths S, Choi KC, Lin C. Prevalence of preventive behaviors and associated factors during early phase of the H1N1 influenza epidemic. Am J Infect Control. 2010;38:374–80. doi: 10.1016/j.ajic.2010.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Rubin GJ, Amlot R, Page L, Wessely S. Public perceptions, anxiety, and behaviour change in relation to the swine flu outbreak: Cross sectional telephone survey. BMJ. 2009;339:b2651. doi: 10.1136/bmj.b2651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Akan H, Gurol Y, Izbirak G, Ozdatli S, Yilmaz G, Vitrinel A, et al. Knowledge and attitudes of university students toward pandemic influenza: A cross-sectional study from Turkey. BMC Public Health. 2010;10:413. doi: 10.1186/1471-2458-10-413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Van D, McLaws ML, Crimmins J, MacIntyre CR, Seale H. University life and pandemic influenza: Attitudes and intended behaviour of staff and students towards pandemic (H1N1) 2009. BMC Public Health. 2010;10:130. doi: 10.1186/1471-2458-10-130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kok G, Jonkers R, Gelissen R, Meertens R, Schaalma H, de Zwart O. Behavioural intentions in response to an influenza pandemic. BMC Public Health. 2010;10:174. doi: 10.1186/1471-2458-10-174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.McCool J, Ameratunga S, Moran K, Robinson E. Taking a risk perception approach to improving beach swimming safety. Int J Behav Med. 2009;16:360–6. doi: 10.1007/s12529-009-9042-8. [DOI] [PubMed] [Google Scholar]
- 29.Barnett DJ, Balicer RD, Lucey DR, Jr, Everly GS, Omer SB, Steinhoff MC, et al. A systematic analytic approach to pandemic influenza preparedness planning. PLoS Med. 2005;2:e359. doi: 10.1371/journal.pmed.0020359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Floyd DL, Prentice-Dunn S, Rogers RW. A meta-analysis of research on protection motivation theory. J Appl Soc Psychol. 2000;30:407–29. [Google Scholar]
- 31.Milne S, Sheeran P, Orbell S. Prediction and intervention in health-related behavior: A meta-analytic review of protection motivation theory. J Appl Soc Psychol. 2000;30:106–43. [Google Scholar]
- 32.Lau JT, Yang X, Tsui HY, Pang E. SARS related preventive and risk behaviours practised by Hong Kong-mainland China cross border travellers during the outbreak of the SARS epidemic in Hong Kong. J Epidemiol Community Health. 2004;58:988–96. doi: 10.1136/jech.2003.017483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Lau JT, Kim JH, Tsui HY, Griffiths S. Anticipated and current preventive behaviors in response to an anticipated human-to-human H5N1 epidemic in the Hong Kong Chinese general population. BMC Infect Dis. 2007;7:18. doi: 10.1186/1471-2334-7-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Van D, McLaws ML, Crimmins J, MacIntyre CR, Seale H. University life and pandemic influenza: Attitudes and intended behaviour of staff and students towards pandemic (H1N1) 2009. BMC Public Health. 2010;10:130. doi: 10.1186/1471-2458-10-130. [DOI] [PMC free article] [PubMed] [Google Scholar]