

Abstract
Background:
E-learning, in addition to promotion of patients’ level of awareness, causes a more efficient way to increase patient-personnel interaction and provision of patients’ educational content.
Materials and Methods:
In a quasi-experimental study, 100 primigravida women, referring to Navab Safavi health care center affiliated to Isfahan University of Medical Sciences, were selected through convenient sampling. The subjects received education via E-learning or booklet education methods for four weeks. Questionnaire of satisfaction with the awareness of prenatal care was completed by both groups before and 4-6 weeks after education. Data were analyzed by student t-test and paired t-test through SPSS with a significance level of P < 0.05.
Results:
No significant difference was noted between scores of satisfaction and awareness in both groups before education, while a significant difference was observed four weeks after intervention (P = 0.004). There was a significant difference between scores of satisfaction and awareness after intervention in both groups (P = 0.001, P = 0.034). Satisfaction and awareness scores increased by 169% and 123%, and 61% and 37% in the E-learning and control groups, respectively (P = 0.034).
Conclusions:
E-learning can cause an increase in the level of primigravida women's satisfaction and awareness. Therefore, conducting such education, as an efficient learning method, is recommended as it needs less time, has lower costs, and does not need any special equipment.
Keywords: Awareness, electronic, learning, prenatal, satisfaction
INTRODUCTION
Prenatal care is among the basic health issues in each society and acts as an efficient intervention in the improvement of pregnancy outcomes.[1,2] Reduction in maternal mortality resulting from pregnancy and delivery is on the top of maternal health priorities of the World Health Organization (WHO).[3] Prenatal health is efficient if accompanied with preventive services and administration of maternal necessary interventions.[4] Lack of access to comprehensive and appropriate health services is the most important obstacle in promotion of maternal care so that a majority of prenatal complications and mortality can be prevented through empowerment of available quality healthcare providing centers.[2,5] Determination of patients’ expectations and effective factors in patients’ satisfaction as well as detecting existing weaknesses in the healthcare providing system is one of the most important indexes of the quality of healthcare services and its monitoring, which can lead to promotion of the methods of providing standard healthcare services.[6,7] In fact, preventive medicine and promotion of individuals’ awareness and satisfaction is the fastest way toward social health. Meanwhile, the level of necessary prenatal education is not actually appropriate in Iran. Education is fundamental for culture, knowledge, and technology.[8,9,10] Until now, various educational methods have been applied to learning. Existence of numerous problems concerning attendance of a skillful teacher, new educational facilities in the region, and access to new educational technology as well as the problem of learners’ attendance in classes have led to development of learning-teaching with the use of modern educational technologies and software.[11] In E-learning, the teacher and the learner are physically far from each other, and the learner can learn the educational material without fact-to-face education.[12] This type of education is the most important application of information technology, which is presented in the form of online learning in different modes such as computer-based learning (web-based leaning) and offline learning.[10] Application of this sort of education in nursing profession and other healthcare professions is important for patient education due to higher level of content, healthcare services, and the use of information and communication technology.[13] Improvement in prenatal care quality, with regard to its effect on maternal health, is essential, and this improvement requires consideration of patients’ expectations and viewpoints. Midwives, as the main members of primary healthcare team, play a major role in the provision of preoperative and post-delivery services.[14] With regard to public advantages of E-learning and rapid development of virtual education, this method seems to be a necessity in all educational centers. As lecture and pamphlet methods are used more in the domain of healthcare and treatment, this study aimed to define the effect of E-learning on the satisfaction and awareness of primigravida women about prenatal care.
MATERIALS AND METHODS
This quasi-experimental study was conducted to define the effect of E-learning on satisfaction and awareness of 100 primigravida women referring to Navab Safavi healthcare center in 2012. Sample size was calculated as 42 subjects in each group (total of 84 subjects) after a pilot study on 20 participants (10 participants in each group) through the use of means comparison formula with CI = 95% and power = 90%. As a probable 20% of subjects drop during study, the number of subjects was calculated to 101. The study was finalized with 100 subjects (50 subjects in each group). Researcher referred to Navab-Safavi health care center after approval from the ethics committee of Isfahan University of Medical Sciences. In order to have an identical prenatal education, the education was conducted by a single person in both groups, so just one healthcare center was selected. The sampling method used was convenient sampling with random allocation of the subjects to both groups. Therefore, among the women referred to the healthcare center each day, the first woman was randomly selected to undergo electronic education and the second women selected to be educated by an education booklet. First, the researcher explained about the goals of research to the subjects after an introduction. Then, after getting a written consent, the researcher checked the inclusion criteria (being primigravida; Iranian nationality and residing in Isfahan; having gestational age 6-12 weeks; least literacy of reading and writing; ability to use a computer or VCR at home; and the ability to speak, hear, and see) and exclusion criteria (existence of a high-risk pregnancy based on maternal health combined manual of categorized care, working staff of medical sciences, and attending preparation classes of delivery during study). If the subjects met all inclusion criteria and lacked exclusion criteria, the personal, familial, and fertility characteristics and source of obtained information questionnaires were complete. Questionnaire of satisfaction with prenatal education was completed after conducting the education by the related healthcare provider in both groups. Data collection tool was a questionnaire containing 31 questions in four sections. The first section contained personal, familial, and fertility characteristics (12 questions); the second contained questions related to the major source of information in relation with prenatal education and prohibition of family, friends, and relatives concerning a source of information; the third section had satisfaction questionnaire (17 questions); and the fourth section included awareness of prenatal education questionnaire (50 questions). Questionnaire of satisfaction was designed based on standard Ersi standard questionnaire (2000)[15] and literature review of valid texts in the form of a researcher-made questionnaire containing 17 questions and a 5-point Likert scale ranging from absolutely satisfied (score 5) to absolutely dissatisfied (score 1). Questionnaire of awareness contained 50 “yes/no” and “no idea” statement questions scored as 0-50. For determination of validity, the questionnaires were given to five academic members of Isfahan University of Medical Sciences and after consideration of their suggestions and doing necessary modifications, the final tool was distributed among 10 pregnant women to answer all questions for determining the reliability. After collection of questionnaires and through test re-test (with a two-week interval), the reliability of satisfaction and awareness questionnaires were calculated as 0.95 and 0.94, respectively. After visiting the pregnant women and giving prenatal education in the E-learning group, the related E-learning software was given to them, and they were asked to work on the software for 4-6 weeks. This 30-minute software contained prenatal care education on the following issues:
Personal, mental, and physical health
Nutrition and medication complements
Advantages, preparation, and appropriate place of a natural delivery
Breast feeding and family planning counseling
Neonatal care and high-risk infant signs, which were prepared using texts, pictures, animation, sound, and slide shows.
As internet access was impossible for all women and, as in similar studies, E-learning had been applied, and low internet speed in Iran resulted in a low sound and image quality during online education, the education content was made in the form of web pages or FLV, WMV, and MP4 that can be used offline. After explaining about the usage of this software, the subjects were asked to answer questions related to satisfaction with prenatal education through phone or their next referral to healthcare center within 4-6 weeks. Educational content of the software was in separate sections; hence, if pregnant women were unable to understand the content, they could rewind the material and access it through an audio-visual facility. Two weeks after giving the software to them, their use was followed up by phone calls to be sure about the subjects’ ability to use the CD. In the second group, education was conducted among pregnant women through an educational booklet after their visit and giving them prenatal care education by a midwife, the educational illustrated booklet was given to them. The women were asked to study the content, and 4-6 weeks later, questionnaire of satisfaction with prenatal education was again completed through phone calls. Any questions by the subjects concerning films and educations as well as other questions were answered through their phone calls. Data were analyzed using independent t-test, paired t-test, and Chi-square test through SPSS version 14; moreover, P < 0.05 was considered significant.
RESULTS
Results showed that 54% of the subjects were at 19-26 years of age, had BMI 19.6-25.9 kg/m2; 61% had education level ≤high school diploma and 39% had university education; 90% were homemakers, 10% were employees, and 89% had adequate income; 87% intended to have a pregnancy and 13% had an unexpected pregnancy. In addition, 92% of the women's spouse were >25 years of age; 74% had high school education or less and 93% were employees.
Diagram 1 depicts the most frequent resource of information before intervention in both groups.
Diagram 1.
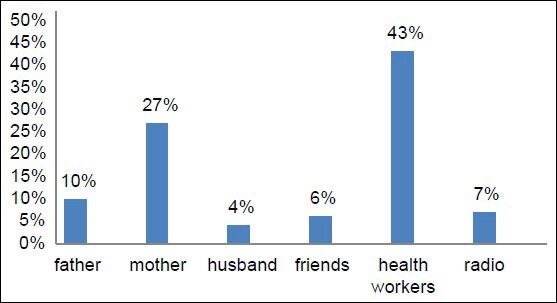
Frequency distribution of subjects based on the source of prenatal education
Both groups were homogenous concerning age, BMI, gestational age, women's and their spouses’ occupation and education, the desire of pregnancy, and score of satisfaction, with prenatal care and had no significant difference before intervention (P > 0.05).
About 94% of women in the E-learning group and 54% in the educational booklet group were satisfied with education after intervention.
Table 1 represents a significant increase in mean scores of satisfaction with prenatal education after intervention compared to before education.
Table 1.
Comparison of primigravida women's mean scores of satisfaction with prenatal care before and four weeks after intervention in multimedia and booklet groups

Four weeks after intervention, 44% were dissatisfied, while 56% were satisfied with education in the booklet group (P = 0.034). In the E-learning group, 6% were dissatisfied, while 94% were satisfied with education. In addition, the level of satisfaction showed a 61% increase in the E-learning education group and 37% increase in the booklet group after intervention compared to before intervention; moreover, there was a significant difference between the two groups. The highest and lowest obtained mean scores in various dimensions of satisfaction after intervention in both E-learning and booklet groups were for prenatal nutrition [Table 2].
Table 2.
Mean scores of satisfaction dimensions based on educational content in primigravida women about prenatal education before and four weeks after intervention in multimedia and booklet groups

In addition, the results showed a significant difference between scores of awareness of prenatal education before and after intervention in both groups [Table 3].
Table 3.
Comparison of mean scores of awareness of prenatal care in primigravida women before and four weeks after intervention in multimedia and booklet groups

Changes in the awareness score in both groups showed that the E-learning group had the highest increase in awareness score (61%) compared to booklet group (37%). Mean difference test showed a significant difference in percentage of awareness score changes (score increased in both groups (P = 0.002).
DISCUSSION
Physical environment is notable as one of the important dimensions of satisfaction; therefore, Handler argued that women pay specific attention to physical environment and cleanness of examination and waiting rooms and may be less interested in using unclean health services.[16] Sharami (2007) also studied the level of pregnant women's satisfaction with the physical environment of waiting rooms and reported the above value as 55.8%.[6] In the present study, mean scores of satisfaction with waiting room and physical environment were 10 (1.2) and 0.2 (001) before and after intervention in both groups, respectively, so that 100% of the subjects were dissatisfied before intervention (conventional education), but only 50% were dissatisfied after intervention in both groups. Farokhi (2008) showed that almost 48% of prenatal education was inappropriate.[5] Gashtasebi (2001) showed that 7 out of 15 centers in Kohkilouiee province had problems in education of pregnant mothers.[17] Meanwhile, prenatal care is as important as other cares and should be conducted to fulfill pregnant women's needs.[5] Among other effective factors on patients’ satisfaction with education is the amount of time spent on this issue by the health provider, which can increase clients’ satisfaction. It was so that this time was 30 minutes for the E-learning group with satisfaction levels of 1.2 and 3.2 before and after intervention, respectively, and 100% and 42% of subjects were dissatisfied with length of education before and after intervention, respectively. Often, active method and dialogues have a higher effect on listeners as in ancient Greece, dialogues and mass communication were reported to have a higher effect on the addressee group.[18] Based on the results of the present study, E-learning and booklet education led to increased satisfaction and awareness of prenatal care. Results showed that increase in mean satisfaction scores were 169% and 123% four weeks after intervention in E-learning and booklet groups, respectively, with a significant difference. Mean scores of awareness four weeks after intervention were 61% and 37% in E-learning and booklet groups, respectively, with a significant difference. Education of health providers by a booklet or other educational materials does not necessarily always meet pregnant women's expectations and result in their satisfaction and awareness.[19] In E-learning, clients learn how to learn. This method has no time or place limitation, and individuals can handle it by self-study at home or other environments and learn the materials based on their own learning schedule. Through this method, the mothers who do not have adequate time to refer to the clinic or receive education from health providers can learn educational materials with no anxiety or stress.[20] Mangeli (2008), in a quasi-experimental one-group study in Arak on the effect of education of natural changes in pregnancy on marital satisfaction of 112 pregnant women with gestational age 4-32 weeks, used education pamphlet of physical and mental changes in women and measured their satisfaction before and one month after distribution of these pamphlets. The results showed that the level of marital satisfaction increased from 168.7 to 187.3 after education by pamphlets in the intervention group.[21] Kuo's study (2009) showed a significant difference between awareness scores before and two weeks after education in both groups of multimedia and conventional education, with the score of awareness increasing 7.2 and 1.7 in E-learning and conventional education groups, respectively (P < 0/001).[22] Davis (2002) showed that pamphlets and an educational package were more efficient than conventional methods, and that the number of visits to physicians dropped from 20% to 2% after education by booklet.[23] Langkamp (2006) reported that verbal education, accompanied with a written material is more efficient than verbal education alone.[24]
In fact, in E-learning, the written information, accompanied with sound and animation, can be available to learners at home, on a trip, and whenever they need. The materials can be printed if needed, which is one of the most important advantages of this method.[25]
CONCLUSION
The results of this study showed higher effects of E-learning and revealed that the increase in levels of clients’ satisfaction and awareness was more in the E-learning than the booklet method. This method can be a solution for managers planning a prenatal education outline, modification and promotion of learners’ levels of awareness, and satisfaction that leads to lower costs and time saving for healthcare providers.
ACKNOWLEDGMENTS
This study was part of a research project approved in September 2012 at Isfahan University of Medical Sciences, and was financially sponsored by Vice Chancellery of research in the related university. We greatly appreciate the support and cooperation of this Vice Chancellery, as well as all pregnant mothers and the healthcare staff at the Navab Safavi Health Center in Isfahan.
Footnotes
Source of Support: Isfahan University of Medical Sciences, 291090
Conflict of Interest: None declared
REFERENCES
- 1.Bakhshi F, Mokhtari N, Jafroodi S, Abbasi M, Atrkar Roshan Z. Survey influencing factors on prenatal care in referring maternal to health care centers in Rasht City. Iran J Nurs Res. 2012;16:21–7. [Google Scholar]
- 2.Tayebi T, Turk Zahrani S, Jannesari S, Mohammadpour R. Assessment of Relationship between Adequacy of Prenatal care Utilization Index with Preterm Labor. J Mazandaran Univ Med Sci. 2011;21:87–95. [Google Scholar]
- 3.Hogan MC, Foreman KJ, Naghavi M, Ahn SY, Wang M, Makela SM, et al. Maternal mortality for 181 countries, 1980-2008: A systematic analysis of progress towards Millennium Development Goal 5. Lancet. 2010;375:1609–23. doi: 10.1016/S0140-6736(10)60518-1. [DOI] [PubMed] [Google Scholar]
- 4.Farrokhi F, Khadivzadeh T. The quality of referrals and follow up cares in prenatal care units of health centers in Mashad, 2001. J Mashhad Sch Nurs Midwifery. 2003;4:27–38. [Google Scholar]
- 5.Farokhi F, khadivzadeh T. Quality assessment of midwives performance in prenatal cares in urban health centers in Mashhad, Iran. Health Monitor. 2008;7:203–10. [Google Scholar]
- 6.Sharami S, Zahiri Z, Zendehdel M. Assessment the client satisfaction in prenatal unit of Rasht public hospitals. J Guilan Univ Med Sci. 2008;17:29–37. [Google Scholar]
- 7.Kojuri MD, Karimi S, Shekarabi R, Hossinei F. A study of satisfaction with prenatal care services in the women attending to the health centers of the Shirevan Chardavel (IRAN), in 2005. Iran J Nurs. 2005;18:61–9. [Google Scholar]
- 8.Arzaniv A, Kermanshahi S, Zahedpasha Y. The effect of educational intervention on continuous breast feeding in low birth weight infants. J Qazvin Univ Med Sci. 2008;12:64–74. [Google Scholar]
- 9.Mirmolaei ST, Moshrefi M, Kazemnejad A, Farivar F, Morteza H. The Effect of Nutrition Education on Nutritional Behaviors in Pregnant Women. J Faculty Nurs Midwifery. 2010;15:35–42. [Google Scholar]
- 10.Siavash V, Tadrisi S, Ghayyem S, Ebadi A, Daneshmandi M, Saghafi N. Comparing the Effect of Triage Education in Lecture and Multimedia Software on Nurses Learning. Iran J Crit Care Nurs. 2011;4:7–12. [Google Scholar]
- 11.Gharebaghi SH, Soltan Mohammadi Z. Discussion learning activity; a novel approach to virtual education. Iranian Journal of Educational Strategies. 2010;3:35–9. [Google Scholar]
- 12.Farshi M, Babatabar Darzi H, Mahmoudi H, Mokhtari Nouri J. Comparison of nursing care learning in air evacuation and transport by lecture and e-learning methods? [Cited Nov 2013];Journal of Military Medicine. 2012 14:27–31. Available from: http://www.militarymedj.ir/browse.php?a_code=A-10-787-1 and slc_lang=en and sid=1 and sw=Transport . [Google Scholar]
- 13.Jones R, Skirton H, Mcmullan M. Feasibility of combining e-health for patients with e-learning for students using synchronous technologies. J Adv Nurs. 2006;56:99–109. doi: 10.1111/j.1365-2648.2006.03984.x. [DOI] [PubMed] [Google Scholar]
- 14.Mirmolaei S, Khakbazan Z, Kazemnejad A, Azari M. Prenatal care utilization rate and patients satisfaction. Hayat. 2007;13:31–40. [Google Scholar]
- 15.Nikpour S, Shahpourian F, Haji Kazemy E, Hosseini F, Safdari M. The Relationship Between Women's Satisfaction With Prenatal Care Services and Characteristics of the Women and the Provision of Services. Iran J Nurs. 2007;20:15–27. [Google Scholar]
- 16.Handler A, Rosenberg D, Raube K, Lyons S. Prenatal care characteristics and African-American Women's Satisfaction with care In a managed care organization. Womens Health Issues. 2003;13:93–103. doi: 10.1016/s1049-3867(03)00031-8. [DOI] [PubMed] [Google Scholar]
- 17.Gashtasebi A, Majlesi F, Rahimi Foroushani A, Nadim A. Quality assessment of prenatal care in kohgiloyeh and boyerahmad province, Iran. Payesh 2002. 2002;1:12–7. [Google Scholar]
- 18.Bahadoran P, Oreizy H. The Effect of Different Educational Methods in Changing Girl Students’ Negative Attitude towards Menstruation, in Intermediate Schools of Isfahan. Iran J Med Educ. 2006;6:27–33. [Google Scholar]
- 19.Toghyani R, Ramezani MA, Izadi M, Shahidi SH, Aghdak P, Motie Z, et al. The effect of prenatal care group education on Pregnant Mothers’ Knowledge, Attitude and Practice. Iran J Med Educ. 2008;7:317–24. [Google Scholar]
- 20.Huang M, Kuo S, Avery M, Chen W, Lin KC, Gau ML. Evaluating effects of a prenatal web-based breastfeeding education programme in Taiwan. J Clin Nurs. 2007;16:1571–9. doi: 10.1111/j.1365-2702.2006.01843.x. [DOI] [PubMed] [Google Scholar]
- 21.Mangeli M, Ramezani T, Mangeli S. The effect of educating about common change in pregnancy period and way to cope with them on marital satisfaction of pregnant women. Iran J Med Educ. 2009;8:305–11. [Google Scholar]
- 22.Kuo SC, Chen YS, Lin KC, Lee TY, Hsu CH. Evaluating the effects of an Internet education programme on newborn care in Taiwan. J Clin Nurs. 2009;18:1592–601. doi: 10.1111/j.1365-2702.2008.02732.x. [DOI] [PubMed] [Google Scholar]
- 23.Davis TC, Fredrickson DD, Bocchini C, Arnold CL, Green KW, Humiston SG, et al. Improving Vaccine Risk/Benefit communication with an immunization education package: A Pilot Study. Ambul Pediatr. 2002;2:193–200. doi: 10.1367/1539-4409(2002)002<0193:ivrbcw>2.0.co;2. [DOI] [PubMed] [Google Scholar]
- 24.Langkamp DL, Hoshaw-woodard S, Boye ME, Lemeshow S. Delay in receipt of immunizations in low-birth-weight children: A nationally representative sample. Arch Pediatr Adolesc Med. 2006;155:167–75. doi: 10.1001/archpedi.155.2.167. [DOI] [PubMed] [Google Scholar]
- 25.Mohamadirirzi S, Bahadoran P, Fahami F. Comparsion between the impacts of e-learning and booklet education on Primigravida Women's Satisfaction about postpartum care. IJOGI. 2013;16:1–8. [Google Scholar]