

Abstract
Appropriate use of local hemostatic agent is one of the important factors on the prognosis of endodontic microsurgery. However, most investigations to date focus on the hemostatic efficacy of the agents, whereas their biologic characteristics have not received enough attention. The purpose of this paper was to review the biologic response of local hemostatic agents, and to provide clinical guidelines on their use during endodontic microsurgery. Electronic database (PUBMED) was screened to search related studies from 1980 to 2013, and 8 clinical studies and 18 animal studies were identified. Among the materials used in these studies, most widely-investigated and used materials, epinephrine, ferric sulfate (FS) and calcium sulfate (CS), were thoroughly discussed. Influence of these materials on local tissue and systemic condition, such as inflammatory and foreign body reaction, local ischemia, dyspigmentation, delayed or enhanced bone and soft tissue healing, and potential cardiovascular complications were assessed. Additionally, biological property of their carrier materials, cotton pellet and absorbable collagen, were also discussed. Clinicians should be aware of the biologic properties of local hemostatic agents and their carrier materials, and should pay attention to the potential complications when using them in endodontic microsurgery.
Keywords: Calcium sulfate, Endodontic microsurgery, Epinephrine, Ferric sulfate, Hemostatic agent, Hemostatics
Introduction
Proper intra-operative hemostasis is one of the important factors that affect the prognosis of endodontic microsurgery, because it not only reduces operation time, but also enhances proper inspection on root structures and application of root-end filling materials.1,2,3 Therefore, the role of local hemostatic agents is more significant in endodontic microsurgery compared to conventional dental surgery. For this reason, numerous materials have been proposed and investigated as local hemostatic agents in surgical endodontic field.
However, most of the investigations focused on the hemostatic efficacy of the agents, whereas their biologic characteristics have not received enough attention. Biologic stability is an important requirement of local hemostatic agents, because they are placed in direct contact with periapical tissues, including cortical and cancellous bone, soft tissue flap, and mental nerve. Inappropriate application of local hemostatic agent in such area could result in undesirable local tissue response and systemic complications. Therefore, biologic properties of local hemostatic agents need to be considered as well as their hemostatic efficacy.
The purpose of this paper is to comprehensively review the literature on the biologic response of local hemostatic agents, and to provide clinical guidelines on using them during endodontic microsurgery.
Review
Electronic database (PUBMED) was screened to identify studies which investigated biologic responses of materials used as local hemostatic agents, from 1980 to 2013. Only in vivo studies which adopted animal or human subjects were included. The tissues investigated in these studies are osseous tissues (cranium, rib, tibia, ilium, femur, maxilla and mandible), soft tissues (schneiderian membrane and gingiva), and sciatic nerve. Studies that investigated open wounds such as extraction socket, intrabony periodontal defect were excluded because most endodontic microsurgeries are conducted on periradicular lesion, which is basically a closed wound.
Finally, 8 clinical studies (Table 1) and 18 animal studies (Table 2) were selected. Among the materials used in these studies (Bone wax, oxidized cellulose, gelatin-based sponge, microfibrillar collagen, ferric sulfate, calcium sulfate, aluminum chloride, chitosan sponge, and epinephrine), some are rarely used at present due to their biologically unfavorable tissue reactions (Bone wax, oxidized cellulose, and gelatin-based sponge).4,5,6,7,8,9,10,11,12
Table 1.
Clinical studies evaluated biologic response of materials used as local hemostatic agents
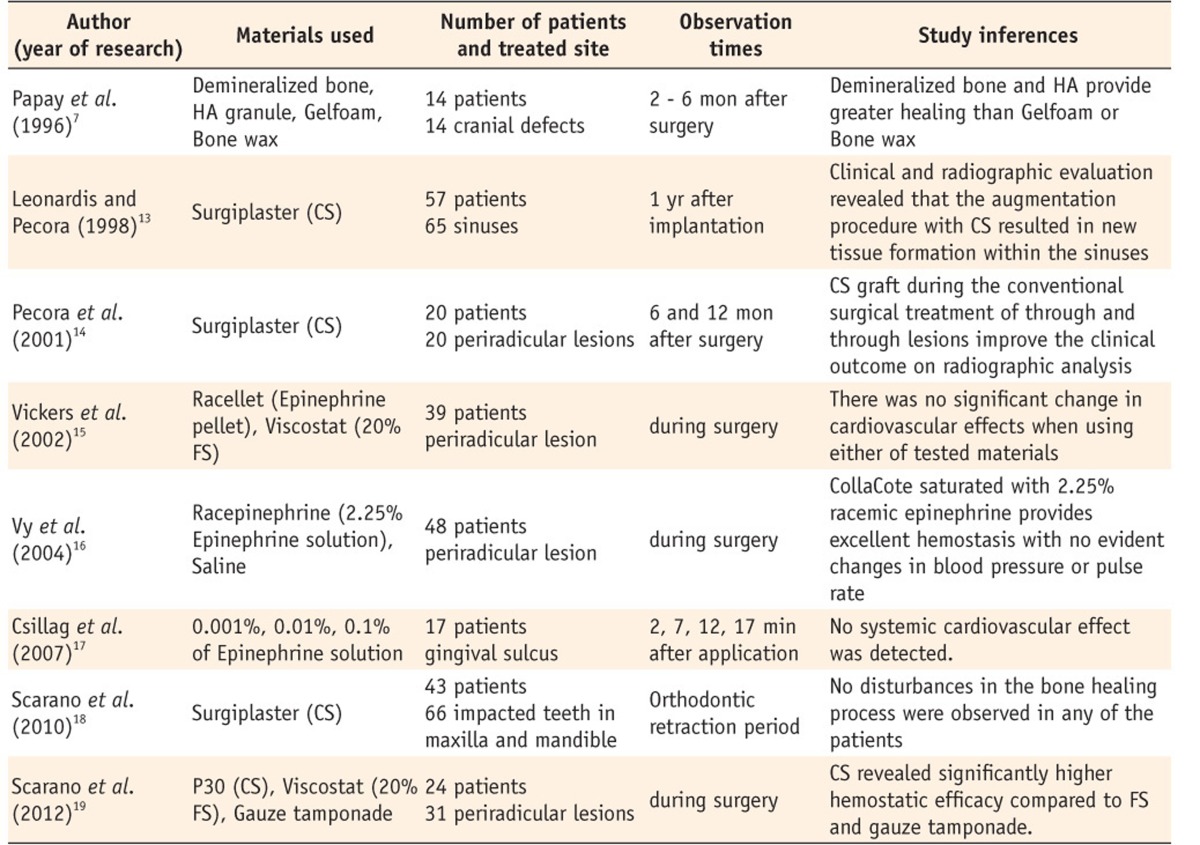
HA, hydroxyapatite; CS, calcium sulfate; FS, ferric sulfate.
Table 2.
Animal studies evaluated biologic response of materials used as local hemostatic agents
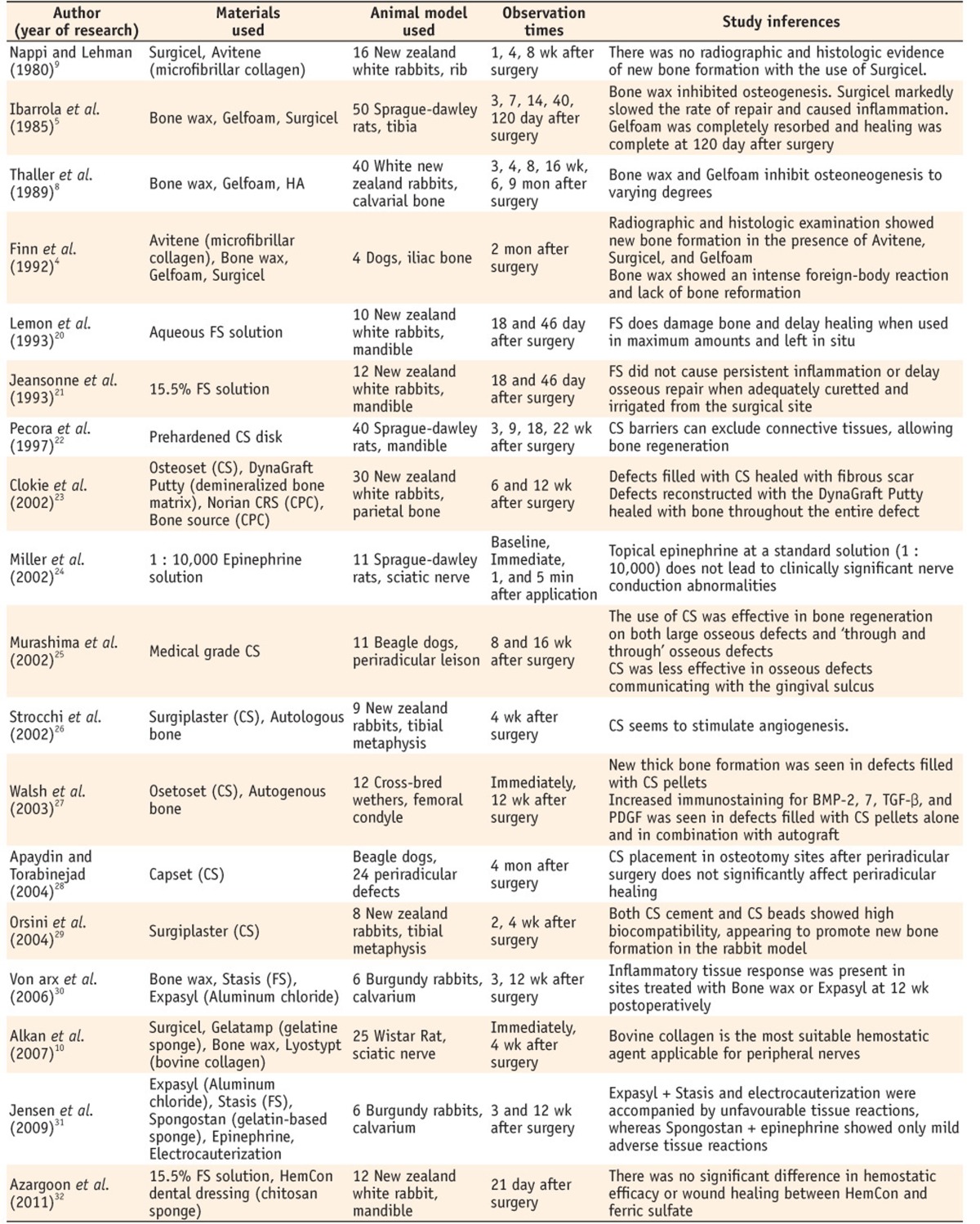
HA, hydroxyapatite; FS, ferric sulfate; CS, calcium sulfate; CPC, calcium phosphate cement.
Most widely-investigated and currently used materials such as epinephrine, ferric sulfate (FS) and calcium sulfate (CS) were selected and discussed further. Influence of these materials on local tissue, such as inflammatory and foreign body reaction, local ischemia, dyspigmentation, delayed or enhanced bone and soft tissue healing were reviewed as well. As for the systemic influence, cardiovascular complications were discussed related with the use of epinephrine. Additionally, biological properties of their carrier materials such as cotton pellet and absorbable collagen were discussed.
Epinephrine
Epinephrine is a sympathomimetic agent, which act as agonist of α and β adrenergic receptors.33 It induces vasoconstriction by binding to α1 receptor, and vasodilation by binding to β2 receptor. As α receptors predominate in oral mucosa, submucosa, and periodontium compared to β2 receptor, epinephrine mainly behaves as potent vasoconstrictor in the oral cavity.34,35,36
1. Hemostatic property
Epinephrine has been recommended as effective local hemostatic agent in endodontic surgery.1,2,34,37,38 Vickers et al. reported superior hemostatic efficacy of epinephrine above 20% FS during endodontic surgery.15 Vy et al. also reported that complete hemostasis was successfully established during 39 of 42 cases of periradicular surgery by epinephrine application alone.16
2. Biological response
1) Local tissue ischemia
Adverse local tissue reaction has rarely been reported with clinical application of epinephrine. However, because of its strong vasoconstrictive effect, epinephrine has been associated with local tissue ischemia and subsequent tissue necrosis on gingiva, bone tissues, and sensory nerve. In fact, such concerns have already been recognized in the medical field. Safety of epinephrine injection related with subsequent local tissue ischemia and tissue necrosis at end-perfusion areas (i.e. finger, foot, nose) has been in debate for decades in plastic surgery. However, recent large-scale clinical studies are now arguing that low concentration (1 : 100,000 - 1 : 80,000) of epinephrine injection is safe in ear, nose, hand and finger region.39,40,41,42 Denkler evaluated 21 cases of digital gangrene associated with epinephrine injection by reviewing the literatures from 1880 to 2000, and suggested that uncontrolled concentration of epinephrine caused by manual dilution as one of the reasons.43 There are few studies that investigated the effect of epinephrine on sensory nerve damage. Miller et al. reported that topical epinephrine (1 : 10,000) application did not cause significant alteration on conduction latency and amplitude in rat model, with no clinically significant nerve conduction abnormalities.24 This finding could be an implication on predicting the influence of topically-applied epinephrine on exposed mental nerve during endodontic microsurgery.
However, these results cannot be directly applied to endodontic microsurgery, because epinephrine concentration used in endodontic microsurgery is much higher (about 1 : 1,000) and the amount is much larger (3.9 - 104 folds) than those of other dental surgeries.44 Moreover, Csillag et al. reported that effect of epinephrine on human gingival blood flow is dose-related, and observed that local gingival ischemia was maintained until the study termination (17 minutes) when high concentration (0.1 and 0.01%) of epinephrine was applied into the gingival sulcus.17 Therefore, probability of epinephrine causing irreversible local tissue ischemia on bone or gingival tissues during endodontic microsurgery still remains.
2) Cardiovascular complications
Epinephrine strongly stimulates cardiac function by increasing both cardiac output and pulse rate when it is bound to β1 receptor.33 Thus, epinephrine is closely related to alteration of cardiovascular function when it enters systemic circulation.45 Jang and Kim stated that systemic influence of epinephrine could be increased in endodontic microsurgery, because endodontic microsurgery reveals two different aspects compared to other dental surgeries in epinephrine application, such as, dose and administration route.44 It is reported that 3.9 - 104 times more epinephrine is used in endodontic microsurgery compared to conventional dental surgery.44 Also, intraosseous route has a greater influence on systemic circulation compared to mucosal or submucosal routes.46,47 However, such concern for systemic complication has not been reproduced in clinical situations up to date. Out of the existing clinical studies which investigated cardiovascular effect of topically-applied epinephrine, none reported significant cardiovascular response during the surgical procedure.15,16,48 Vy et al. suggested that systemic absorption of epinephrine would be limited because first-applied epinephrine causes immediate vasoconstriction on the bone surface.16
Nevertheless, it should be noted that cardiovascular emergencies have been continuously induced during surgeries in oral & maxillofacial region, even at low concentrations (1 : 100,000 - 1 : 80,000).49,50,51,52 Therefore, cardiovascular stability of epinephrine is still unclear, and further investigation is needed to identify the amount of systemic absorption and the cardiovascular influence of epinephrine during endodontic microsurgery.
3. Clinical suggestion
There is no clinical evidence that epinephrine induce ischemic necrosis of periapical tissues, or cardiovascular complications in endodontic microsurgery up to date. However, it should be noted that epinephrine is applied in remarkably high concentration and volume in endodontic microsurgery, and the administration route is influential to systemic circulation. Therefore, it is imperative to restrict epinephrine administration to minimal extent until further investigation guarantees the safety of epinephrine from local and systemic complications. Kim and Rethnam recommended the use of only one epinephrine pellet and subsequent sterile dry cotton pellets.1 For situation which requires larger amount of epinephrine, clinician should calculate the total amount of applied epinephrine. Commercial products such as Racellet pellet (Pascal Company, Inc., Bellvue, WA, USA) would be useful for this estimation.
Ferric sulfate
FS (Fe2(SO4)3) is a chemical compound. Since it was first introduced in the dermatologic field as Monsel's solution in 1856, FS has been popularly used in the dental field as local hemostatic agent during crown and bridge impression, pulpotomy, and periradicular surgery.1,2,34,53,54,55 In the clinical setting, 15 - 20% FS solution is commonly used.15,32
1. Hemostatic property
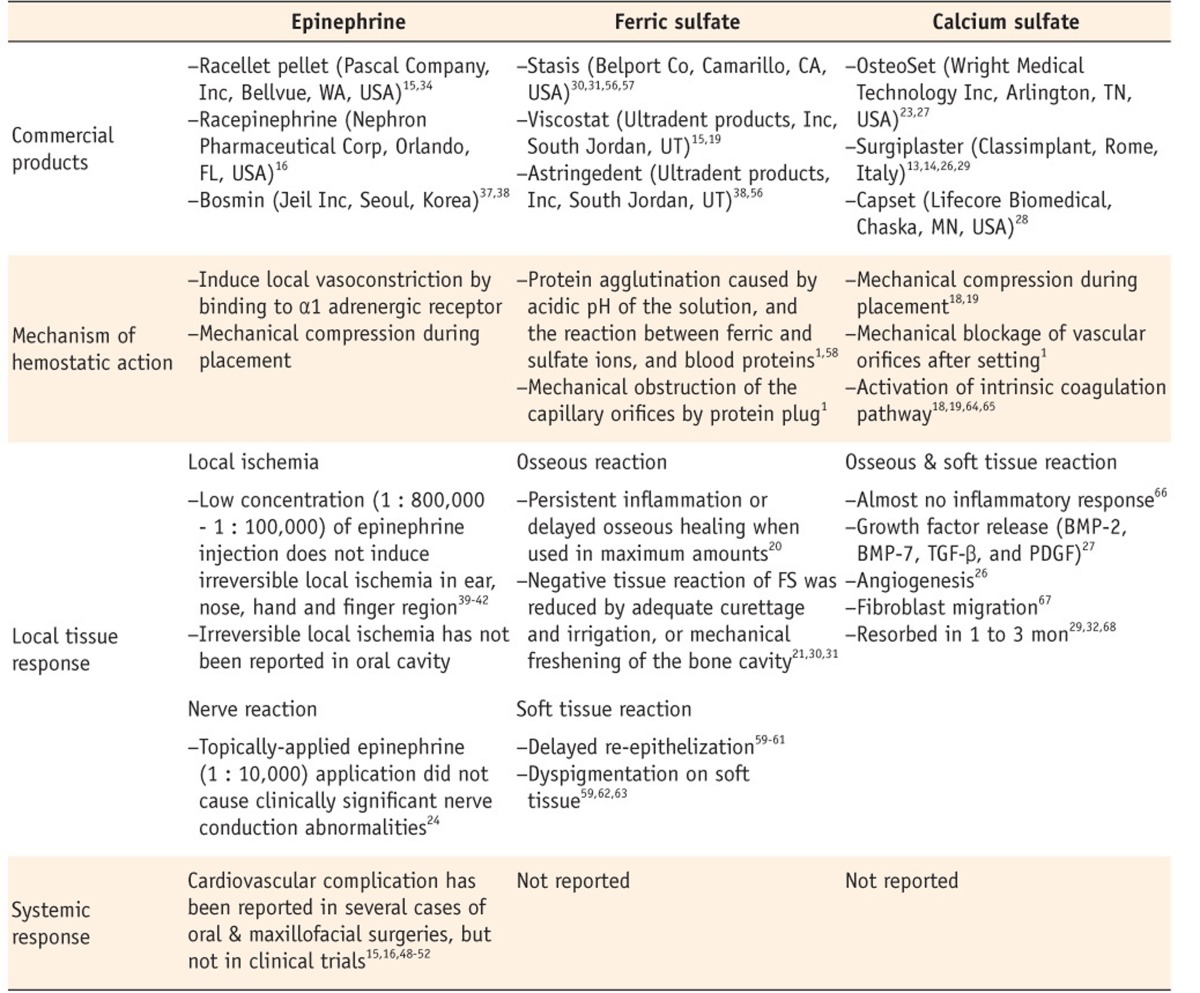
Ease of application is an obvious advantage of FS as local hemostatic agent. When applied on bleeding spot, FS immediately forms dark-brownish clot without additional pressure, and the hemostasis could be maintained up to 5 minutes.1,20 This is attributed to the hemostatic mechanism of FS (Table 3).
Table 3.
Properties of epinephrine, ferric sulfate, and calcium sulfate as local hemostatic agent
However, hemostatic ability of FS is not superior compared with other local hemostatic agents, according to the existing clinical and in vivo studies. Von Arx et al. compared the hemostatic efficacy of FS with bone wax and aluminium chloride in rabbit calvarium model, and reported that bleeding reduction of FS group is not significantly different from other experimental groups.30 In similar rabbit model, Scarano et al. reported that FS shows inferior hemostatic ability compared to calcium sulfate.19 Also a clinical study by Vickers et al. that used FS in periradicular surgery reported that FS revealed less hemostatic efficacy than topically-applied epinephrine.15
2. Biological response
Lemon et al. tested the effect of FS on osseous wound healing in rabbit model.20 FS-treated group revealed extensive foreign body reaction, healing retardation, and abscess formation in some cases when FS was used in maximum amounts and left in the bone cavity for 18 and 46 days. In another corresponding study, Jeansonne et al. reported that such persistent inflammation or delayed osseous healing were not noticeable when FS was properly curetted and irrigated from the bone cavity.21 Von Arx et al. also showed that negative tissue reaction of FS could be minimized when FS was adequately removed by additional curettage and saline irrigation.30 Jensen et al. recommended mechanical freshening of the bone cavity after the surgical procedure to reduce undesirable tissue reactions.31
However, it should be noted that unset retrograde filling material could be damaged by the flushing of irrigating solution or water spray. Therefore such managements (i.e, mechanical freshening, sufficient curettage and irrigation) are not recommended when retrograde filling material with long-setting time such as ProRoot MTA (Dentsply Tulsa Dental, Johnson City, TN, USA) is used.31
Influence of FS on the soft tissue has not been broadly investigated in the dental field. However literatures from dermatologic surgery could be helpful because Monsel's solution (20% ferric subsulfate) has been popularly used and investigated in the dermatologic field.69,70 Although being an effective local hemostatic measure, Monsel's solution resulted in several post-operative complications such as delayed re-epithelization and dyspigmentation on soft tissue.59,60,61,62,63 Armstrong et al. compared the effect of collagen matrix and Monsel's solution on punch biopsy wounds, and observed more inflammation, higher incidence of wound infection, and slower re-epithelialization rate on the group treated by Monsel's solution at 4 weeks.61
3. Clinical suggestion
Although adverse tissue reaction from FS could be reduced by thorough curettage and irrigation on surgical site, it draws more uncertainty on normal healing compared with other local hemostatic agents. Also, retro-filling material with long-setting time could be damaged by such additional removal procedure. Therefore, FS should be applied in bone cavity to a minimum extent. Kim and Kratchman recommended to apply FS only on small bleeding points of cortical bone surface.34 It should be noted that FS also interferes soft tissue healing. Therefore clinicians should carefully handle FS and avoid contact with the surgical flap during endodontic microsurgery.
Calcium sulfate
CS naturally exists as the dihydrate (CaSO4·2H2O), which is also known as 'gypsum'. Through the heating process called calcination, CS dihydrate is transformed to CS hemihydrate (CaSO4·½H2O), which is known as 'plaster of paris'.66
CaSO4·2H2O + heat → CaSO4·½H2O + 1½H2O
Most medical products are manufactured in hemihydrate form. When mixed with water, hemihydrate rapidly reverts to the dihydrate form, constructing rigid crystal network in vivo.66
CaSO4·½H2O + 1½H2O → CaSO4·2H2O
1. Hemostatic property
Although CS has been used as a biomaterial in both dental and medical area for decades, recently it received attention as local hemostatic agent. Kim and Rethnam stated the usefulness of CS as local hemostatic agent during endodontic microsurgery in 1997.1 They pointed out excellent biocompatibility, resorbability, and inexpensive price as the advantages of CS,1 and recommended its application when the size of the periapical bony crypt is large.34 Scarano et al. reported that CS reveals significantly better hemostatic ability above FS or gauze tamponade in simulated bone cavity on rabbit model.19 Scarano et al. also tested the effectiveness of CS to maintain surgical field dry during surgical exposure and orthodontic bracket bonding of impacted teeth.18 CS-applied group showed superior result on bonding prognosis, compared to control group which only applied gauze tamponade.
2. Biological response
CS is known to be absorbed rapidly and completely in vivo, causing almost no inflammatory response.66 Moreover, CS is reported to be positively related to growth factor release (BMP-2, BMP-7, TGF-β, and PDGF), angiogenesis, and fibroblast migration, which could enhance bone healing.26,27,67 For this reason, CS has been broadly investigated and shows successful clinical outcomes in dental fields for treating periodontal intrabony defect, sinus augmentation, and guided tissue regeneration.13,71,72,73,74. Effectiveness of CS as bio-graft material has also been advocated in surgical endodontic field. Murashima et al. reported that large periradicular defects and through-and-through periradicular defects were adequately healed by CS placement in beagle dog model.25 Pecora et al. also reported that CS grafts improved the clinical outcome of periradicular surgery in through-and-through defects compared to control group.14 Some studies are still questioning the effectiveness of CS as bone graft material, and comment that CS does not significantly improve bony healing.23,28,75 Nevertheless, it is mostly accepted that application of calcium sulfate does not retard bony healing. These results indicate that CS could be used as hemostatic agent in periradicular surgery without biologically negative effects, which is agreed upon by Apaydin and Torabinejad.28
3. Clinical suggestion
CS reveals many qualities close to the ideal local hemostatic agent, which shows highly biocompatible and bio-resorbable properties, effective achievement and maintenance of hemostasis, ease of manipulation, and cost-effectiveness. CS application seems to be a desirable treatment option especially in the large lesions and the through-and-through lesions that needs additional bone graft or mechanical barrier.
Carrier materials
Several local hemostatic agents prepared in liquid form (i.e. epinephrine solution, FS solution) needs carrier material to be delivered to the surgical site. Such carrier materials directly contact the surgical site, and often left in the bony crypt during the surgical procedure, to maintain hemostasis and to prevent excess filling materials from falling into the cavity. Therefore, biologic response of carrier material is another important issue for adequate healing of periapical structures.
1. Cotton pellet
Cotton pellet is one of the most widely-used carrier materials in endodontic microsurgery. However, because it is not bio-resorbable, the remaining cotton fiber has been suggested as a factor that causes inflammation and healing retardation.16 Several case reports are warning the undesirable tissue reaction induced by cotton remnants.76,77 Sexton et al. reported intensive foreign body reaction from a remaining cottons sponge, which developed a large soft tissue mass in femur, and termed the mass as 'cottonballoma'.77 Kalbermatten et al. also reported pseudotumor of femur, which was induced by remnants of the cotton sponge.76
2. Absorbable collagen sponge
As bio-incompatible nature of cotton materials draws more uncertainty on periapical healing, absorbable collagen materials are being highlighted as carrier material. Collagen sponges already have been actively used in dental area, such as revascularization and perforation repair procedures, due to its space-maintaining and bio-absorbable property.78,79 Collagen seems to be a suitable material as carrier material for local hemostatic agents in endodontic microsurgery. Collagen sponge is able to contain plenty of fluid in limited volume, and it could be removed with no residual fiber or debris.16,80,81 Most important point is that collagen dose not interfere with bone and soft tissue healing, because it is biologically absorbed even when it is left in the surgical cavity.82
3. Clinical suggestion
Vy et al. successfully achieved local hemostasis during endodontic surgery by application of absorbable collagen sponges (CollaCote, Integra LifeSciences Corporation, Plainsboro, NJ, USA) soaked in 2.25% racemic epinephrine, reducing the potential complications by remaining cotton fiber.16 Biocompatible carrier material such as absorbable collagen would be an alternative to present cotton-based carrier materials. Cotton pellet could be used as carrier, if there are no alternatives. However, all of the cotton fibers should be removed from the bony crypt prior to closure of the surgical site to prevent interference of periapical healing.
Conclusions
Use of local hemostatic agent is essential for proper hemostasis during endodontic microsurgery. However, inadequate selection and application of local hemostatic agents could cause undesirable biological responses, deteriorating the prognosis of endodontic microsurgery. Although hemostatic efficacy is an important requirement of local hemostatic agents for proper management of root during endodontic microsurgery, adequate healing of periapical structures cannot be guaranteed unless biologic stability of local hemostatic agents is considered. Therefore, clinicians should be aware of the biologic properties of local hemostatic agents and their carrier materials, and should pay attention to the potential complications when using them on endodontic microsurgery. Further researches are needed to ensure the safety of local hemostatic agents, and to enhance biologic properties of the materials, making them closer to the ideal local hemostatic agent.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Kim S, Rethnam S. Hemostasis in endodontic microsurgery. Dent Clin North Am. 1997;41:499–511. [PubMed] [Google Scholar]
- 2.Witherspoon DE, Gutmann JL. Haemostasis in periradicular surgery. Int Endod J. 1996;29:135–149. doi: 10.1111/j.1365-2591.1996.tb01360.x. [DOI] [PubMed] [Google Scholar]
- 3.Cho YW, Kim E. Is stopping of anticoagulant therapy really required in a minor dental surgery? - How about in an endodontic microsurgery? Restor Dent Endod. 2013;38:113–118. doi: 10.5395/rde.2013.38.3.113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Finn MD, Schow SR, Schneiderman ED. Osseous regeneration in the presence of four common hemostatic agents. J Oral Maxillofac Surg. 1992;50:608–612. doi: 10.1016/0278-2391(92)90443-4. [DOI] [PubMed] [Google Scholar]
- 5.Ibarrola JL, Bjorenson JE, Austin BP, Gerstein H. Osseous reactions to three hemostatic agents. J Endod. 1985;11:75–83. doi: 10.1016/s0099-2399(85)80123-0. [DOI] [PubMed] [Google Scholar]
- 6.Johnson P, Fromm D. Effects of bone wax on bacterial clearance. Surgery. 1981;89:206–209. [PubMed] [Google Scholar]
- 7.Papay FA, Morales L, Jr, Ahmed OF, Neth D, Reger S, Zins J. Comparison of ossification of demineralized bone, hydroxyapatite, Gelfoam, and bone wax in cranial defect repair. J Craniofac Surg. 1996;7:347–351. doi: 10.1097/00001665-199609000-00006. [DOI] [PubMed] [Google Scholar]
- 8.Thaller SR, Kim JC, Kawamoto HK. Calvarial bone graft donor site: a histological study in a rabbit model. Ann Plast Surg. 1989;23:390–395. doi: 10.1097/00000637-198911000-00002. [DOI] [PubMed] [Google Scholar]
- 9.Nappi JF, Lehman JA., Jr The effects of Surgicel on bone formation. Cleft Palate J. 1980;17:291–296. [PubMed] [Google Scholar]
- 10.Alkan A, Inal S, Yildirim M, Baş B, Ağar E. The effects of hemostatic agents on peripheral nerve function: an experimental study. J Oral Maxillofac Surg. 2007;65:630–634. doi: 10.1016/j.joms.2005.12.076. [DOI] [PubMed] [Google Scholar]
- 11.Boyes-Varley JG, Cleaton-Jones PE, Lownie JF. Effect of a topical drug combination on the early healing of extraction sockets in the vervet monkey. Int J Oral Maxillofac Surg. 1988;17:138–141. doi: 10.1016/s0901-5027(88)80169-3. [DOI] [PubMed] [Google Scholar]
- 12.Hjortdal O. The fate of resorbable hemostatic implants in rats. Acta Odontol Scand. 1970;28:323–336. doi: 10.3109/00016357009032038. [DOI] [PubMed] [Google Scholar]
- 13.De Leonardis D, Pecora GE. Augmentation of the maxillary sinus with calcium sulfate: one-year clinical report from a prospective longitudinal study. Int J Oral Maxillofac Implants. 1999;14:869–878. [PubMed] [Google Scholar]
- 14.Pecora G, De Leonardis D, Ibrahim N, Bovi M, Cornelini R. The use of calcium sulphate in the surgical treatment of a 'through and through' periradicular lesion. Int Endod J. 2001;34:189–197. doi: 10.1046/j.1365-2591.2001.00369.x. [DOI] [PubMed] [Google Scholar]
- 15.Vickers FJ, Baumgartner JC, Marshall G. Hemostatic efficacy and cardiovascular effects of agents used during endodontic surgery. J Endod. 2002;28:322–323. doi: 10.1097/00004770-200204000-00015. [DOI] [PubMed] [Google Scholar]
- 16.Vy CH, Baumgartner JC, Marshall JG. Cardiovascular effects and efficacy of a hemostatic agent in periradicular surgery. J Endod. 2004;30:379–383. doi: 10.1097/00004770-200406000-00001. [DOI] [PubMed] [Google Scholar]
- 17.Csillag M, Nyiri G, Vag J, Fazekas A. Dose-related effects of epinephrine on human gingival blood flow and crevicular fluid production used as a soaking solution for chemo-mechanical tissue retraction. J Prosthet Dent. 2007;97:6–11. doi: 10.1016/j.prosdent.2006.10.004. [DOI] [PubMed] [Google Scholar]
- 18.Scarano A, Carinci F, Cimorelli E, Quaranta M, Piattelli A. Application of calcium sulfate in surgical-orthodontic treatment of impacted teeth: a new procedure to control hemostasis. J Oral Maxillofac Surg. 2010;68:964–968. doi: 10.1016/j.joms.2009.12.020. [DOI] [PubMed] [Google Scholar]
- 19.Scarano A, Artese L, Piattelli A, Carinci F, Mancino C, Iezzi G. Hemostasis control in endodontic surgery: a comparative study of calcium sulfate versus gauzes and versus ferric sulfate. J Endod. 2012;38:20–23. doi: 10.1016/j.joen.2011.09.019. [DOI] [PubMed] [Google Scholar]
- 20.Lemon RR, Steele PJ, Jeansonne BG. Ferric sulfate hemostasis: effect on osseous wound healing. Left in situ for maximum exposure. J Endod. 1993;19:170–173. doi: 10.1016/s0099-2399(06)80681-3. [DOI] [PubMed] [Google Scholar]
- 21.Jeansonne BG, Boggs WS, Lemon RR. Ferric sulfate hemostasis: effect on osseous wound healing. II. With curettage and irrigation. J Endod. 1993;19:174–176. doi: 10.1016/S0099-2399(06)80682-5. [DOI] [PubMed] [Google Scholar]
- 22.Pecora G, Andreana S, Margarone JE, 3rd, Covani U, Sottosanti JS. Bone regeneration with a calcium sulfate barrier. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84:424–429. doi: 10.1016/s1079-2104(97)90043-3. [DOI] [PubMed] [Google Scholar]
- 23.Clokie CM, Moghadam H, Jackson MT, Sandor GK. Closure of critical sized defects with allogenic and alloplastic bone substitutes. J Craniofac Surg. 2002;13:111–121. doi: 10.1097/00001665-200201000-00026. [DOI] [PubMed] [Google Scholar]
- 24.Miller Q, Meekin G, Murdock C. The effect of topical epinephrine on peripheral nerve conduction. Laryngoscope. 2002;112:1888–1891. doi: 10.1097/00005537-200210000-00035. [DOI] [PubMed] [Google Scholar]
- 25.Murashima Y, Yoshikawa G, Wadachi R, Sawada N, Suda H. Calcium sulphate as a bone substitute for various osseous defects in conjunction with apicectomy. Int Endod J. 2002;35:768–774. doi: 10.1046/j.1365-2591.2002.00565.x. [DOI] [PubMed] [Google Scholar]
- 26.Strocchi R, Orsini G, Iezzi G, Scarano A, Rubini C, Pecora G, Piattelli A. Bone regeneration with calcium sulfate: evidence for increased angiogenesis in rabbits. J Oral Implantol. 2002;28:273–278. doi: 10.1563/1548-1336(2002)028<0273:BRWCSE>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 27.Walsh WR, Morberg P, Yu Y, Yang JL, Haggard W, Sheath PC, Svehla M, Bruce WJ. Response of a calcium sulfate bone graft substitute in a confined cancellous defect. Clin Orthop Relat Res. 2003;406:228–236. doi: 10.1097/01.blo.0000030062.92399.6a. [DOI] [PubMed] [Google Scholar]
- 28.Apaydin ES, Torabinejad M. The effect of calcium sulfate on hard-tissue healing after periradicular surgery. J Endod. 2004;30:17–20. doi: 10.1097/00004770-200401000-00003. [DOI] [PubMed] [Google Scholar]
- 29.Orsini G, Ricci J, Scarano A, Pecora G, Petrone G, Iezzi G, Piattelli A. Bone-defect healing with calcium-sulfate particles and cement: an experimental study in rabbit. J Biomed Mater Res B Appl Biomater. 2004;68:199–208. doi: 10.1002/jbm.b.20012. [DOI] [PubMed] [Google Scholar]
- 30.von Arx T, Jensen SS, Hänni S, Schenk RK. Haemostatic agents used in periradicular surgery: an experimental study of their efficacy and tissue reactions. Int Endod J. 2006;39:800–808. doi: 10.1111/j.1365-2591.2006.01152.x. [DOI] [PubMed] [Google Scholar]
- 31.Jensen SS, Yazdi PM, Hjørting-Hansen E, Bosshardt DD, von Arx T. Haemostatic effect and tissue reactions of methods and agents used for haemorrhage control in apical surgery. Int Endod J. 2010;43:57–63. doi: 10.1111/j.1365-2591.2009.01637.x. [DOI] [PubMed] [Google Scholar]
- 32.Azargoon H, Williams BJ, Solomon ES, Kessler HP, He J, Spears R. Assessment of hemostatic efficacy and osseous wound healing using HemCon dental dressing. J Endod. 2011;37:807–811. doi: 10.1016/j.joen.2011.02.023. [DOI] [PubMed] [Google Scholar]
- 33.Katzung BG, Masters S, Trevor A. Basic and clinical pharmacology. 12th ed. Columbus, OH: McGraw-Hill Education; 2011. pp. 129–149. [Google Scholar]
- 34.Kim S, Kratchman S. Modern endodontic surgery concepts and practice: a review. J Endod. 2006;32:601–623. doi: 10.1016/j.joen.2005.12.010. [DOI] [PubMed] [Google Scholar]
- 35.Chu WS, Park SH, Ahn DK, Kim SK. Effect of local anesthesia on pulpal blood flow in mechanically stimulated teeth. J Korean Acad Conserv Dent. 2006;31:257–262. [Google Scholar]
- 36.Lee JS, Kim SK. The influence of epinephrine concentration in local anesthetics on pulpal and gingival blood flows. J Korean Acad Conserv Dent. 2003;28:475–484. [Google Scholar]
- 37.Kim E, Song JS, Jung IY, Lee SJ, Kim S. Prospective clinical study evaluating endodontic microsurgery outcomes for cases with lesions of endodontic origin compared with cases with lesions of combined periodontal-endodontic origin. J Endod. 2008;34:546–551. doi: 10.1016/j.joen.2008.01.023. [DOI] [PubMed] [Google Scholar]
- 38.Song M, Jung IY, Lee SJ, Lee CY, Kim E. Prognostic factors for clinical outcomes in endodontic microsurgery: a retrospective study. J Endod. 2011;37:927–933. doi: 10.1016/j.joen.2011.04.005. [DOI] [PubMed] [Google Scholar]
- 39.Chowdhry S, Seidenstricker L, Cooney DS, Hazani R, Wilhelmi BJ. Do not use epinephrine in digital blocks: myth or truth? Part II. A retrospective review of 1111 cases. Plast Reconstr Surg. 2010;126:2031–2034. doi: 10.1097/PRS.0b013e3181f44486. [DOI] [PubMed] [Google Scholar]
- 40.Häfner HM, Röcken M, Breuninger H. Epinephrine-supplemented local anesthetics for ear and nose surgery: clinical use without complications in more than 10,000 surgical procedures. J Dtsch Dermatol Ges. 2005;3:195–199. doi: 10.1111/j.1610-0378.2005.04758.x. [DOI] [PubMed] [Google Scholar]
- 41.Lalonde D, Bell M, Benoit P, Sparkes G, Denkler K, Chang P. A multicenter prospective study of 3,110 consecutive cases of elective epinephrine use in the fingers and hand: the Dalhousie Project clinical phase. J Hand Surg Am. 2005;30:1061–1067. doi: 10.1016/j.jhsa.2005.05.006. [DOI] [PubMed] [Google Scholar]
- 42.Sylaidis P, Logan A. Digital blocks with adrenaline. An old dogma refuted. J Hand Surg Br. 1998;23:17–19. doi: 10.1016/s0266-7681(98)80210-6. [DOI] [PubMed] [Google Scholar]
- 43.Denkler K. A comprehensive review of epinephrine in the finger: to do or not to do. Plast Reconstr Surg. 2001;108:114–124. doi: 10.1097/00006534-200107000-00017. [DOI] [PubMed] [Google Scholar]
- 44.Jang Y, Kim E. Cardiovascular effect of epinephrine in endodontic microsurgery: a review. Restor Dent Endod. 2013;38:187–193. doi: 10.5395/rde.2013.38.4.187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Troullos ES, Goldstein DS, Hargreaves KM, Dionne RA. Plasma epinephrine levels and cardiovascular response to high administered doses of epinephrine contained in local anesthesia. Anesth Prog. 1987;34:10–13. [PMC free article] [PubMed] [Google Scholar]
- 46.Gogerty JH, Strand HA, Ogilvie AL, Dille JM. Vasopressor effects of topical epinephrine in certain dental procedures. Oral Surg Oral Med Oral Pathol. 1957;10:614–622. doi: 10.1016/s0030-4220(57)80009-7. [DOI] [PubMed] [Google Scholar]
- 47.Wood M, Reader A, Nusstein J, Beck M, Padgett D, Weaver J. Comparison of intraosseous and infiltration injections for venous lidocaine blood concentrations and heart rate changes after injection of 2% lidocaine with 1:100,000 epinephrine. J Endod. 2005;31:435–438. doi: 10.1097/01.don.0000148146.10314.1a. [DOI] [PubMed] [Google Scholar]
- 48.Besner E. Systemic effects of racemic epinephrine when applied to the bone cavity during periapical surgery. Va Dent J. 1972;49:9–12. [PubMed] [Google Scholar]
- 49.Ferry DR, Henry RL, Kern MJ. Epinephrine-induced myocardial infarction in a patient with angiographically normal coronary arteries. Am Heart J. 1986;111:1193–1195. doi: 10.1016/0002-8703(86)90023-2. [DOI] [PubMed] [Google Scholar]
- 50.Foster CA, Aston SJ. Propranolol-epinephrine interaction: a potential disaster. Plast Reconstr Surg. 1983;72:74–78. doi: 10.1097/00006534-198307000-00017. [DOI] [PubMed] [Google Scholar]
- 51.Lee JY, Hong SJ, Chon JY, Kwon SY. Cardiac arrest induced by submucosal injection of epinephrine in a patient with variant angina. Rhinology. 2010;48:251–253. doi: 10.4193/Rhin09.059. [DOI] [PubMed] [Google Scholar]
- 52.Umino M, Ohwatari T, Shimoyama K, Nagao M. Unexpected atrial fibrillation during tooth extraction in a sedated elderly patient. Anesth Prog. 1994;41:77–80. [PMC free article] [PubMed] [Google Scholar]
- 53.Monsel L. Proprieté hémostatique du sulfate de peroxyde de Fer. Rec Mem Med Milit. 1856;17:424. [Google Scholar]
- 54.Fischer DE. Tissue management: a new solution to an old problem. Gen Dent. 1987;35:178–182. [PubMed] [Google Scholar]
- 55.Smith NL, Seale NS, Nunn ME. Ferric sulfate pulpotomy in primary molars: a retrospective study. Pediatr Dent. 2000;22:192–199. [PubMed] [Google Scholar]
- 56.von Arx T, Jensen SS, Hänni S. Clinical and radiographic assessment of various predictors for healing outcome 1 year after periapical surgery. J Endod. 2007;33:123–128. doi: 10.1016/j.joen.2006.10.001. [DOI] [PubMed] [Google Scholar]
- 57.von Arx T, Jensen SS, Hänni S, Friedman S. Five-year longitudinal assessment of the prognosis of apical microsurgery. J Endod. 2012;38:570–579. doi: 10.1016/j.joen.2012.02.002. [DOI] [PubMed] [Google Scholar]
- 58.Evans BE. Local hemostatic agents. N Y J Dent. 1977;47:109–114. [PubMed] [Google Scholar]
- 59.Davis JR, Steinbronn KK, Graham AR, Dawson BV. Effects of Monsel's solution in uterine cervix. Am J Clin Pathol. 1984;82:332–335. doi: 10.1093/ajcp/82.3.332. [DOI] [PubMed] [Google Scholar]
- 60.Sawchuk WS, Friedman KJ, Manning T, Pinnell SR. Delayed healing in full-thickness wounds treated with aluminum chloride solution. A histologic study with evaporimetry correlation. J Am Acad Dermatol. 1986;15:982–989. doi: 10.1016/s0190-9622(86)70261-2. [DOI] [PubMed] [Google Scholar]
- 61.Armstrong RB, Nichols J, Pachance J. Punch biopsy wounds treated with Monsel's solution or a collagen matrix. A comparison of healing. Arch Dermatol. 1986;122:546–549. [PubMed] [Google Scholar]
- 62.Amazon K, Robinson MJ, Rywlin AM. Ferrugination caused by Monsel's solution. Clinical observations and experimentations. Am J Dermatopathol. 1980;2:197–205. doi: 10.1097/00000372-198000230-00002. [DOI] [PubMed] [Google Scholar]
- 63.Duray PH, Livolsi VA. Recurrent dysplastic nevus following shave excision. J Dermatol Surg Oncol. 1984;10:811–815. doi: 10.1111/j.1524-4725.1984.tb01185.x. [DOI] [PubMed] [Google Scholar]
- 64.Horbett TA. Principles underlying the role of adsorbed plasma proteins in blood interactions with foreign materials. Cardiovasc Pathol. 1993;2(Supplement):137–148. [Google Scholar]
- 65.Ziats NP, Pankowsky DA, Tierney BP, Ratnoff OD, Anderson JM. Adsorption of Hageman factor (factor XII) and other human plasma proteins to biomedical polymers. J Lab Clin Med. 1990;116:687–696. [PubMed] [Google Scholar]
- 66.Thomas MV, Puleo DA. Calcium sulfate: properties and clinical applications. J Biomed Mater Res B Appl Biomater. 2009;88:597–610. doi: 10.1002/jbm.b.31269. [DOI] [PubMed] [Google Scholar]
- 67.Payne JM, Cobb CM, Rapley JW, Killoy WJ, Spencer P. Migration of human gingival fibroblasts over guided tissue regeneration barrier materials. J Periodontol. 1996;67:236–244. doi: 10.1902/jop.1996.67.3.236. [DOI] [PubMed] [Google Scholar]
- 68.Guarnieri R, Pecora G, Fini M, Aldini NN, Giardino R, Orsini G, Piattelli A. Medical grade calcium sulfate hemihydrate in healing of human extraction sockets: clinical and histological observations at 3 months. J Periodontol. 2004;75:902–908. doi: 10.1902/jop.2004.75.6.902. [DOI] [PubMed] [Google Scholar]
- 69.Larson PO. Topical hemostatic agents for dermatologic surgery. J Dermatol Surg Oncol. 1988;14:623–632. doi: 10.1111/j.1524-4725.1988.tb03390.x. [DOI] [PubMed] [Google Scholar]
- 70.Palm MD, Altman JS. Topical hemostatic agents: a review. Dermatol Surg. 2008;34:431–445. doi: 10.1111/j.1524-4725.2007.34090.x. [DOI] [PubMed] [Google Scholar]
- 71.Scarano A, Degidi M, Iezzi G, Pecora G, Piattelli M, Orsini G, Caputi S, Perrotti V, Mangano C, Piattelli A. Maxillary sinus augmentation with different biomaterials: a comparative histologic and histomorphometric study in man. Implant Dent. 2006;15:197–207. doi: 10.1097/01.id.0000220120.54308.f3. [DOI] [PubMed] [Google Scholar]
- 72.Orsini M, Orsini G, Benlloch D, Aranda JJ, Lazaro P, Sanz M, De Luca M, Piattelli A. Comparison of calcium sulfate and autogenous bone graft to bioabsorbable membranes plus autogenous bone graft in the treatment of intrabony periodontal defects: a split-mouth study. J Periodontol. 2001;72:296–302. doi: 10.1902/jop.2001.72.3.296. [DOI] [PubMed] [Google Scholar]
- 73.Aichelmann-Reidy ME, Heath CD, Reynolds MA. Clinical evaluation of calcium sulfate in combination with demineralized freeze-dried bone allograft for the treatment of human intraosseous defects. J Periodontol. 2004;75:340–347. doi: 10.1902/jop.2004.75.3.340. [DOI] [PubMed] [Google Scholar]
- 74.Kim CK, Chai JK, Cho KS, Moon IS, Choi SH, Sottosanti JS, Wikesjo UM. Periodontal repair in intrabony defects treated with a calcium sulfate implant and calcium sulfate barrier. J Periodontol. 1998;69:1317–1324. doi: 10.1902/jop.1998.69.12.1317. [DOI] [PubMed] [Google Scholar]
- 75.Shaffer CD, App GR. The use of plaster of paris in treating infrabony periodontal defects in humans. J Periodontol. 1971;42:685–690. doi: 10.1902/jop.1971.42.11.685. [DOI] [PubMed] [Google Scholar]
- 76.Kalbermatten DF, Kalbermatten NT, Hertel R. Cotton-induced pseudotumor of the femur. Skeletal Radiol. 2001;30:415–417. doi: 10.1007/s002560100358. [DOI] [PubMed] [Google Scholar]
- 77.Sexton CC, Lawson JP, Yesner R. Case report 174: 'Cottonballoma' of femur (due to retained surgical sponge with foreign body giant cell reaction) Skeletal Radiol. 1981;7:211–213. doi: 10.1007/BF00361868. [DOI] [PubMed] [Google Scholar]
- 78.Petrino JA, Boda KK, Shambarger S, Bowles WR, McClanahan SB. Challenges in regenerative endodontics: a case series. J Endod. 2010;36:536–541. doi: 10.1016/j.joen.2009.10.006. [DOI] [PubMed] [Google Scholar]
- 79.Ferris DM, Baumgartner JC. Perforation repair comparing two types of mineral trioxide aggregate. J Endod. 2004;30:422–424. doi: 10.1097/00004770-200406000-00011. [DOI] [PubMed] [Google Scholar]
- 80.Stein MD, Salkin LM, Freedman AL, Glushko V. Collagen sponge as a topical hemostatic agent in mucogingival surgery. J Periodontol. 1985;56:35–38. doi: 10.1902/jop.1985.56.1.35. [DOI] [PubMed] [Google Scholar]
- 81.Chvapil M. Collagen sponge: theory and practice of medical applications. J Biomed Mater Res. 1977;11:721–741. doi: 10.1002/jbm.820110508. [DOI] [PubMed] [Google Scholar]
- 82.Mannai C, Leake D, Pizzoferrato A, Ciapetti G, Spangiogi C. Histological evaluation of purified bovine tendon collagen sponge in tooth extraction sites in dogs. Oral Surg Oral Med Oral Pathol. 1986;61:315–323. doi: 10.1016/0030-4220(86)90408-1. [DOI] [PubMed] [Google Scholar]