

Abstract
Background
Research on cerebral stroke symptoms using hospital records has reported that women experience more nontraditional symptoms of stroke (eg, mental status change, pain) than men do. This is an important issue because nontraditional symptoms may delay the decision to get medical assistance and increase the difficulty of correct diagnosis. In the present study, we investigate sex differences in the stroke experience as described in stories on weblogs.
Objective
The goal of this study was to investigate the feasibility of using the Internet as a source of data for basic research on stroke experiences.
Methods
Stroke experiences described in blogs were identified by using StoryUpgrade, a program that searches blog posts using a fictional prototype story. In this study, the prototype story was a description of a stroke experience. Retrieved stories coded by the researchers as relevant were used to update the search query and retrieve more stories using relevance feedback. Stories were coded for first- or third-person narrator, traditional and nontraditional patient symptoms, type of stroke, patient sex and age, delay before seeking medical assistance, and delay at hospital and in treatment.
Results
There were 191 relevant stroke stories of which 174 stories reported symptoms (52.3% female and 47.7% male patients). There were no sex differences for each traditional or nontraditional stroke symptom by chi-square analysis (all Ps>.05). Type of narrator, however, affected report of traditional and nontraditional symptoms. Female first-person narrators (ie, the patient) were more likely to report mental status change (56.3%, 27/48) than male first-person narrators (36.4%, 16/44), a marginally significant effect by logistic regression (P=.056), whereas reports of third-person narrators did not differ for women (27.9%, 12/43) and men (28.2%, 11/39) patients. There were more reports of at least 1 nontraditional symptom in the 92 first-person reports (44.6%, 41/92) than in the 82 third-person reports (25.6%, 21/82, P=.006). Ischemic or hemorrhagic stroke was reported in 67 and 29 stories, respectively. Nontraditional symptoms varied with stroke type with 1 or more nontraditional symptoms reported for 79.3% (23/29) of hemorrhagic stroke patients and 53.7% (36/67) of ischemic stroke patients (P=.001).
Conclusions
The results replicate previous findings based on hospital interview data supporting the reliability of findings from weblogs. New findings include the effect of first- versus third-person narrator on sex differences in the report of nontraditional symptoms. This result suggests that narrator is an important variable to be examined in future studies. A fragmentary data problem limits some conclusions because important information, such as age, was not consistently reported. Age trends strengthen the feasibility of using the Internet for stroke research because older adults have significantly increased their Internet use in recent years.
Keywords: cerebral stroke, signs and symptoms, sex differences, Internet, blogging
Introduction
Background
The Internet has become a valuable tool in clinical medicine, both as a source of health information and by providing online interventions designed to improve health [1]. Moreover, the Internet also offers a research opportunity through the wealth of information available from search queries or social network posts. For example, the type and frequency of search queries concerning infectious disease have been associated with outbreaks of these diseases [2,3] and analysis of weblog stories has revealed young adults’ mental health concerns [4]. Following this infodemiology approach [5], the present research investigates the feasibility of analyzing weblog posts about cerebral stroke experiences as a source of evidence to test a hypothesis in basic medical research: whether or not there are sex differences in cerebral stroke symptoms.
Our interest in variation between men and women in stroke experiences derives from reports based on hospital records of a variety of sex differences ranging from experience of symptoms to treatment, and from the possibility that these differences may influence stroke outcome. There is evidence that women experience delays from the onset of symptoms to diagnosis and treatment of stroke compared to men [6,7], although this difference is not consistently reported [8]. Such delays are a concern because they may obviate certain treatments that require rapid administration after onset of symptoms. Indeed, women are less likely than men to receive thrombolytic treatment, which may be because women are more likely to experience delay after the onset of symptoms that is beyond the 3-hour treatment window [6,9]. Women receive fewer diagnostic tests than men do, even when controlling for age, ethnicity, insurance status, and risk factors [10]. Moreover, outcomes of stroke are poorer for women compared to men [7,11-14]. Women’s older age at the time of stroke is a likely factor, but delays in treatment and the type of treatment may also be a factor as well [15].
In sum, there are several factors that may contribute to sex differences in type and delay of treatment. We focus on one of them: There are reports that women experience more nontraditional symptoms of stroke than men and this may make correct diagnosis more difficult for women [9,15,16].
Sex Differences in Stroke Symptoms
Stroke is the fourth leading cause of death in the United States, [17] with more women than men dying of stroke each year [14,17]. Traditional symptoms of stroke include hemibody numbness and paresis, language disorders in comprehension and/or production, dysarthria, diplopia and other visual disturbances, facial weakness, ataxia, vertigo, and imbalance. Nontraditional symptoms of stroke include pain, mental status change (disorientation, confusion, or loss of consciousness), headache, lightheadedness, other general neurological symptoms (nausea, hiccups, and nonfocal weakness), and some nonneurological symptoms (chest pain, palpitations, and shortness of breath) [15,18,19]. Although headache has been reported as a symptom of ischemic and hemorrhagic strokes [20,21], headache has been considered a nontraditional symptom because it is not a focal neurological sign and it is common in a number of health problems [18].
Mental status change is the nontraditional stroke symptom most consistently reported as occurring more frequently in women than men [11,13,15,18,22,23]. Other nontraditional symptoms that have been reported as more frequent in women than men, although with less consistency, are pain other than headache [15]; (see [8] for a marginally significant difference), difficulty swallowing [11,24], headache [20], visual disturbances [24], and generalized weakness [23]. In contrast, women were significantly less likely than men to report traditional symptoms of dizziness or problems with walking or balance [15,16,23,25]. Indeed, in one study, women were less likely than men to experience any traditional stroke symptoms or to suspect stroke [8].
The Present Study
In this study, we investigate the feasibility of using stroke experiences described in weblogs as a source of data on sex differences in traditional and nontraditional symptoms. We used newly developed software that identified personal stories on the blogosphere that were relevant to a prototype story. We then analyzed symptoms described in the blogs by a stroke survivor or a third-person narrator. This follows hospital studies of stroke patients that included symptom reports by patients or third parties [16,18,23]. We predict that the identity of the narrator will be significant in reports of mental status change, a symptom often reported as more common in women patients. Mental change may have no effect observable to a third party unlike traditional symptoms, such as hemibody weakness, speech impairment, or loss of balance. Moreover, a patient’s communication of internal mental states to a third party may be constrained by speech impairments associated with stroke. Thus, we will test for the first time whether or not changes in mental status are more likely to be reported as a symptom by a first-person than a third-person narrator, and whether there are sex differences in these reports.
We anticipated that descriptions of stroke experiences would vary widely in the information supplied because of the absence of a prescribed format for blogs, but that salient aspects of the experience, such as symptoms, the identity of the narrator, and delay in treatment, would be included in most descriptions. We also anticipated that the patient population would over- and underrepresent certain demographic groups in the population of stroke patients inasmuch as younger adults use blogs more than older adults and women bloggers make up the majority of this younger age group, whereas men bloggers make up the majority in the older age group [26]. These constraints will be considered in evaluating the feasibility of analysis of weblog data in testing hypotheses concerning sex differences in stroke symptoms.
Methods
Sampling Blogs
Stroke experiences described in weblogs were identified using a program called StoryUpgrade [27]. StoryUpgrade is a system we developed to aid in the retrieval of stories that describe classes of activities or events that we wish to analyze (eg, stories about protest rallies, car crashes, or stroke experiences). The system is supplied with a constant stream of stories pulled from the Web. Each day, the system downloads 1.5 million English-language weblog posts. The system then applies supervised machine learning techniques to classify these posts as personal stories. This classifier has a precision of 0.66 and recall of 0.5, meaning that it detects approximately half of all English-language personal stories, but one-third of posts it considers stories are actually not [28]. These posts are then indexed by using an off-the-shelf information retrieval platform, enabling them to be searched quickly. Figure 1 shows an example set of search results from the StoryUpgrade system. For the present study, the system was backed by 17.4 million personal stories posted to weblogs in 2010 and 2011.
Figure 1.
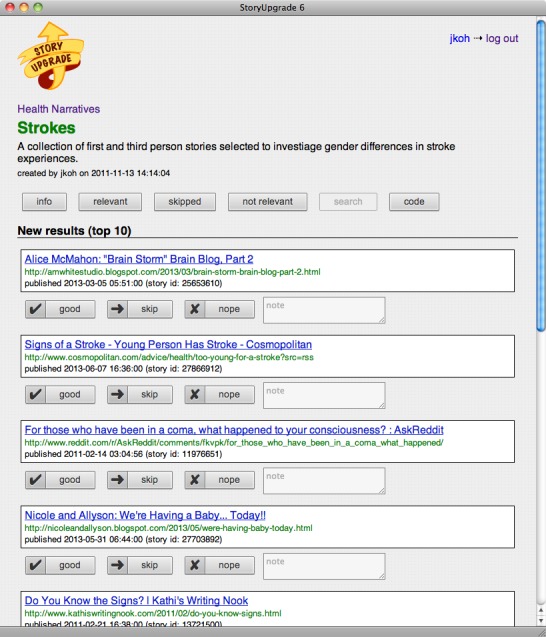
Screenshot of StoryUpgrade showing search results for stroke narratives.
In addition to enabling search queries, the StoryUpgrade system allows a user to provide feedback about the relevance of the retrieved stories to the user’s information need. A user can mark a story as relevant, irrelevant, or the user can simply skip the story. This feedback is then incorporated into the search system, allowing it to retrieve increasingly relevant stories. To accomplish this, the StoryUpgrade system uses the Rocchio algorithm [29]. This technique incorporates the user’s relevance feedback, encoding the information about story relevance provided by the user directly into the query. Words from stories the user considers relevant are weighed heavily, and words from stories the user considers irrelevant are weighed less heavily. This process modifies the original query to be more similar to relevant stories and less similar to irrelevant stories. The skip category allows a user to remove a story from the queue of stories to be judged without it impacting the weights of words in the query [30].
For this study, we wrote a fictional prototype story to be used as a query to the StoryUpgrade system. This prototype story was written in a colloquial style typical of blogs. It described a stroke experience including keywords for traditional and nontraditional symptoms (eg, “my speech did not make sense and was slurred,” “could not pick up my arm or leg on one side,” “I felt confused”), as well as “911,” “emergency room,” “paramedics,” and “diagnosed with stroke.” These keywords were selected based on symptoms and events that appear in hospital admission interviews or medical records of stroke patients [8,15,23]. The prototype story is presented in Multimedia Appendix 1.
The technique of writing a prototype story is one that has worked well with the StoryUpgrade system in other contexts. It is effective because it seeds the system with a vocabulary similar to what an actual blogger might use when writing a relevant story. An important concern of this technique is how it may bias the search results toward stories that feature details and phrasing included in the prototype story. Although this bias must be taken under consideration when analyzing the stories retrieved by StoryUpgrade, the bias is mitigated by the relevance feedback system previously described. As a StoryUpgrade user marks stories as relevant, the vocabulary from these stories is incorporated into the search query, casting a wider net for relevant stories. For instance, an initially retrieved story may describe the author experiencing slurred speech, a symptom described in the prototype story. This same story may describe vertigo, a symptom not included in the prototype story, or the author may say she “couldn’t think clearly,” describing confusion in a way that was not done in the prototype story. Although the initially retrieved stories may be biased toward the initial query, this bias is reduced as the user marks stories as relevant.
In this study, all stories retrieved by StoryUpgrade were read by 2 of the authors and marked as relevant if they contained information about a stroke experience in either a first- or third-person account, and marked as irrelevant if the story was not about a stroke. Irrelevant stories were dropped from further analysis. Stories that did not identify the sex of the stroke patient or were in blogs that denied access, such as expired pages or blogs requiring a subscription or permission, were ignored by being placed in the skip category (281 stories in this study). Using this procedure, we identified 191 relevant stories and 244 irrelevant stories.
Coding
We developed codes for first- or third-person narrator, whether or not a third-person narrator witnessed the event, the relation of the third-person narrator to the patient, patient sex and age, patient symptoms, assistance to obtain medical attention (eg, 911) , delay before seeking assistance, delay at hospital, treatment, and stroke outcome. If the specific age of the patient was not available, age range was coded if explicit information was available.
Classification of symptoms as traditional or nontraditional was based on the American Stroke Association’s stroke warning signs [31] as well as symptom classifications used in previous research on sex differences [15,18,19]. Traditional symptoms were hemiparesis/hemiplegia (for body, for face, or both body and face), impaired speech or comprehension, visual disturbance, ataxia/discoordination, vertigo, and difficulty with balance. Nontraditional symptoms were pain (excluding headache), mental status change (disorientation, confusion, loss of consciousness), headache, lightheadedness, other neurologic symptoms (nausea, hiccups, nonfocal weakness), and nonneurologic symptoms (chest pain, palpitations, shortness of breath). Although the American Stroke Association identifies confusion as a symptom, we categorized it as nontraditional consistent with previous research on sex differences. Each traditional and nontraditional symptom was coded for each patient as a dichotomous variable (reported or not reported). Symptoms were coded that occurred in the interval from the onset of the stroke experience until medical assistance was secured. Two of the authors coded all stories. An example of the form used to code each story is shown in Figure 2. Initial agreement in codes across the 2 coders was 83% and discrepancies in codes were discussed and resolved.
Figure 2.
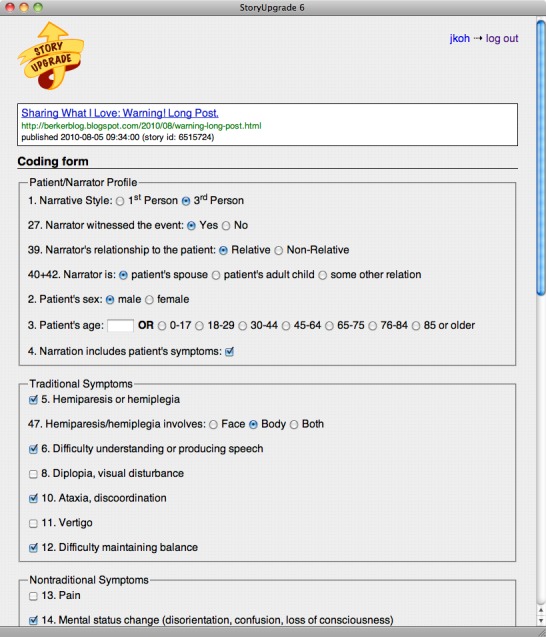
Screenshot of StoryUpgrade annotation tool for coding stroke narratives.
Statistical Analysis
Each relevant story was assigned to a category for patient sex, stroke type, and type of narrator, with third-person narrators also categorized by whether or not they witnessed the stroke and their relation to the patient. The frequency of occurrence of each traditional and nontraditional symptom was compared between men and women and between ischemic and hemorrhagic stroke types using chi-square tests. Logistic regression was used to compare nontraditional symptoms as a group, and mental status change, in particular, by narrator type and sex.
Results
We obtained data from 191 stroke stories that met the inclusion criteria, with 52.4% (100/191) about female stroke patients and 47.6% (91/191) about male stroke patients. Of these stories, 174 reported symptoms (52.3%, 91/174 for women patients; 47.7%, 83/174 for men patients). Of the 174 stories reporting symptoms, 85 (48.9%) stories included age. Table 1 presents the age distribution by sex. Given the age distribution of bloggers [26], our sample overrepresented younger adults, yielding proportionately more reports about patients aged 45 to 64 years than 65 years and older. This contrasts with the monotonic increase in risk of stroke that occurs with age during adulthood [17,19]. However, 89 stories (51.1%) did not include age and it is unknown if the patients in these stories had an age distribution similar to Table 1.
Table 1.
Age distribution for women (n=40) and men (n=45) patients reporting age.
| Age (years) | Patients, n (%) | |
|
|
Women | Men |
| 0-17 | 2 (5) | 1 (2) |
| 18-29 | 9 (23) | 5 (11) |
| 30-44 | 16 (40) | 8 (18) |
| 45-64 | 8 (20) | 19 (42) |
| 65-75 | 3 (8) | 8 (18) |
| 76-84 | 0 (0) | 3 (7) |
| 85+ | 2 (5) | 1 (2) |
Of the 191 stories, 50.8% (97/191) were narrated by the patient and 49.2% (94/191) were narrated by a third person. These percentages did not differ by sex of the patient, as shown by chi-square analysis (Table 2). When a third person was the narrator, he or she was a witness to the stroke for 39.6% (19/48) of women and 45.7% (21/46) of men, a nonsignificant sex difference. Most (83%, 78/94) third-person narrators were a relative of the patient and the type of relative varied for men and women patients in the chi-square analysis (P=.008). The narrators for women patients were more likely to be their adult child (60.0%, 24/40) or other relative (25.0%, 10/40) than for men patients (39.5%, 15/38 and 13.2%, 5/38, respectively). Men patients were more likely to have their spouse as narrator (47.4%, 18/38) than women patients were (15.0%, 6/40).
Table 2.
Profiles of narrators for women (n=100) and men (n=91) patients.
| Narrator characteristics | Patients, n (%) | P | ||
|
|
Women | Men |
|
|
| Narrator |
|
|
.72 | |
|
|
First-person | 52 (52.0) | 45 (49.5) |
|
|
|
Third-person | 48 (48.0) | 46 (51.5) |
|
| Third-person witness to stroke |
|
|
.55 | |
|
|
Yes | 19 (39.6) | 21 (45.7) |
|
|
|
No | 29 (60.4) | 25 (54.3) |
|
| Third-person relationship-relative |
|
|
.008 | |
|
|
Adult child | 24 (60.0) | 15 (39.5) |
|
|
|
Other | 10 (25.0) | 5 (13.2) |
|
|
|
Spouse | 6 (15.0) | 18 (47.4) |
|
| Third-person relationship-nonrelative |
|
|
n/a | |
|
|
Friend | 2 (25.0) | 3 (37.5) |
|
|
|
Stranger | 6 (75.0) | 5 (62.5) |
|
Chi-square analyses of the number of men and women experiencing specific stroke symptoms showed no significant sex differences for traditional or nontraditional symptoms, as seen in Table 3. The largest sex differences were for mental status change and visual disturbances, with women reporting more of these symptoms, although neither difference reached statistical significance. In a further analysis, we evaluated sex differences in mental status change separately for first- and third-person narrators (the small number of reports of visual disturbances precluded a similar analysis of this symptom). The narrators for the 91 women and 83 men patients included in the symptom analysis were 53% (92/174) first person and 47% (82/174) third person across sex. First-person narrators reported more mental status change than third-person narrators (P=.01). When mental status change was analyzed by patient sex (see Table 4), first-person narrators were more likely to report mental status change when the narrator was a woman patient (56%, 27/48) than a man patient (36%, 16/44), although this effect narrowly missed statistical significance (P=.056). However, third-person narrators showed no difference in their reports of mental status change for women (28%, 12/43) and men patients (28%, 11/39).
Table 3.
Stroke symptoms reported for women (n=91) and men (n=83) patients.
| Symptom type | Patients, n (%) | P | |||
|
|
Women | Men |
|
||
| Traditional symptoms |
|
|
|
||
|
|
Hemiparesis/hemiplegia | 68 (74.7) | 63 (75.9) | .86 | |
|
|
|
Body | 30 (44.1) | 33 (52.4) | .33 |
|
|
|
Face | 2 (2.9) | 4 (6.3) |
|
|
|
|
Both body and face | 36 (52.9) | 26 (41.3) |
|
|
|
Impaired speech or comprehension | 59 (64.8) | 47 (56.6) | .27 | |
|
|
Visual disturbance | 11 (12.1) | 5 (6.0) | .17 | |
|
|
Ataxia, discoordination | 16 (17.6) | 11 (13.3) | .43 | |
|
|
Vertigo | 13 (14.3) | 13 (15.7) | .80 | |
|
|
Difficulty with balance | 7 (7.7) | 8 (9.6) | .65 | |
| Nontraditional symptoms |
|
|
|
||
|
|
Pain (excluding headache) | 5 (5.5) | 5 (6.0) | .88 | |
|
|
Mental status change | 39 (42.9) | 27 (32.5) | .16 | |
|
|
Headache | 16 (17.6) | 11 (13.3) | .62 | |
|
|
Lightheadedness | 5 (5.5) | 3 (3.6) | .55 | |
|
|
Other neurologic symptoms | 13 (14.3) | 9 (10.8) | .67 | |
|
|
Nonneurologic symptoms | 4 (4.4) | 5 (6.0) | .63 | |
Table 4.
Reports of mental status change for women (n=91) and men (n=83) patients by narrator.
| Mental status change | Patients, n (%) | P value | ||
|
|
Women | Men |
|
|
| First-person narrator |
|
|
.056 | |
|
|
Yes | 27 (56.3) | 16 (36.4) |
|
|
|
No | 21 (43.7) | 28 (63.6) |
|
| Third-person narrator |
|
|
.97 | |
|
|
Yes | 12 (27.9) | 11 (28.2) |
|
|
|
No | 31 (72.1) | 28 (71.8) |
|
We tested whether this same pattern of effects for patient sex and type of narrator was found for all other nontraditional symptoms combined, excluding mental status change. With 174 male and female patients combined, more of the 92 first-person narrators (44.6%, 41/92) reported at least 1 nontraditional symptom than the 82 third-person narrators (25.6%, 21/82, P=.006). As shown in Table 5, this same pattern was seen for each sex separately with no significant differences between male and female patients in the narrator effect. This pattern of more nontraditional symptoms reported by first- versus third-person narrators was not because third-person narrators reported fewer symptoms in general: 90% or more of both first- and third-person narrators reported traditional symptoms for both men and women patients.
Table 5.
Reports of nontraditional symptoms (excluding mental status change) for women (n=91) and men (n=82) patients by narrator.
| Number of nontraditional symptoms | Patients, n (%) | P | ||
|
|
Women | Men |
|
|
| First-person narrator |
|
|
.80 | |
|
|
≥1 | 22 (45.8) | 19 (43.2) |
|
|
|
None | 26 (54.2) | 25 (56.8) |
|
| Third-person narrator |
|
|
.62 | |
|
|
≥1 | 12 (27.9) | 9 (23.1) |
|
|
|
None | 31 (72.1) | 30 (76.9) |
|
Of the stories describing symptoms, 96 reported a medical diagnosis of an ischemic (n=67) or hemorrhagic (n=29) stroke. We compared the number of reports of each traditional and nontraditional symptom by ischemic and hemorrhagic stroke patients (see Table 6). Chi-square analysis showed differences between the 2 stroke types for 2 specific symptoms: ischemic stroke patients were significantly more likely to experience vertigo (P=.008), whereas hemorrhagic stroke victims were significantly more likely to experience headaches (P=.002). Categorizing stroke symptoms as traditional or nontraditional symptoms, 79% (23/29) of hemorrhagic stroke patients experienced nontraditional symptoms whereas only 54% (36/67) of ischemic stroke patients did (P=.001). Looking at percentage of patients in Table 6, symptoms of general pain, mental status change, and headache seemed to contribute most to this effect of stroke type on nontraditional symptoms.
Table 6.
Reports of stroke symptoms by ischemic (n=67) and hemorrhagic (n=29) stroke.
| Symptom type | Stroke type, n (%) | P | |||
|
|
Ischemic | Hemorrhage |
|
||
| Traditional symptoms |
|
|
|
||
|
|
Hemiparesis/hemiplegia | 56 (84) | 20 (69) | .11 | |
|
|
|
Body | 19 (34) | 9 (45) | .30 |
|
|
|
Face | 5 (9) | 0 (0) |
|
|
|
|
Both body and face | 32 (57) | 11 (55) |
|
|
|
Impaired speech or comprehension | 42 (63) | 19 (66) | .79 | |
|
|
Visual disturbance | 8 (12) | 3 (10) | .82 | |
|
|
Ataxia, discoordination | 13 (19) | 2 (7) | .12 | |
|
|
Vertigo | 18 (27) | 1 (3) | .01 | |
|
|
Difficulty with balance | 5 (7) | 2 (7) | .92 | |
| Nontraditional symptoms |
|
|
|
||
|
|
Pain (excluding headache) | 3 (4) | 4 (14) | .11 | |
|
|
Mental status change | 21 (31) | 14 (48) | .11 | |
|
|
Headache | 7 (10) | 11 (38) | .002 | |
|
|
Lightheadedness | 5 (7) | 0 (0) | .13 | |
|
|
Other neurologic symptoms | 10 (15) | 5 (17) | .77 | |
|
|
Nonneurologic symptoms | 5 (7) | 2 (7) | .92 | |
Virtually all stroke patients sought medical assistance (96%-97%) regardless of sex, although 44% (35/80) of women patients delayed getting assistance and 32% (24/76) of men patients delayed, a difference that did not reach statistical significance (P=.12). There was no sex difference in time to get treatment in the hospital; 90% to 91% of both women and men patients received treatment immediately upon arrival.
Discussion
Principal Findings
The results demonstrate that weblogs are a useful source of stories of stroke experiences and that most stories describe symptoms. The reliability of the description of experiences in the weblog stories is supported by their replication of several previous findings in studies based on hospital interview data: the more frequent reports of traditional than nontraditional symptoms [15], evidence that women patients experience mental status change (here in the analysis by narrator) as a symptom more than men [11,13,15,18,22,23], the greater frequency of ischemic than hemorrhagic strokes [8,11,15], and the greater frequency of headaches and other nontraditional symptoms in hemorrhagic strokes [25,32].
The results also offer some new findings involving variables that affect symptom reports and sex differences, but that have been relatively unexplored in previous studies. As hypothesized, mental status change was reported more by first- than third-person narrators. The most obvious explanation is that this symptom is a change in an internal state that the patient is aware of but may not be visible to a third-person observer, unlike other symptoms that involve observable effects (eg, hemiplegia, impaired speech). Moreover, the frequency of report of mental status change showed no sex difference with third-person narrators, but was greater for women than men patients with first-person narrators, although this missed statistical significance (P=.056). Further research is needed to follow up this finding with a study including a greater number of patients that will allow control of variables confounded with sex in the present study, most importantly age. The age distribution suggests that the sample of women patients was younger than the sample of men patients, although narrators did not consistently supply information on patient age. Nonetheless, the narrator effect is consistent with the hypothesis that mental status change may be more available to the patient than to third-person narrators because it is an internal state.
Another significant effect of narrator was on reports of nontraditional symptoms. First-person narrators produced more nontraditional symptoms than third-person narrators, excluding the symptom of mental status change. This difference may be because other nontraditional symptoms involve internal states and are difficult for a third party to observe (eg, headache, pain). Thus, the results suggest that a first- or third-person narrator significantly affects the type of symptom reported and also whether or not sex differences are observed for symptoms, such as mental status change.
Third-person narrators are frequently called upon to describe symptoms to first responders or hospital personnel. Indeed, first- and third-person narrators are common in studies of stroke symptoms based on hospital interviews or records (eg, [11,15,16,18,23]). The present study, however, is the first to suggest that type of narrator is an influential variable and to demonstrate its significant association with specific symptoms. Previous studies have not evaluated effects of type of narrator. The present results suggest that type of narrator is an important variable to include in analysis of symptoms in hospital stroke studies, especially in the analysis of sex differences.
Limitations
The results also demonstrate the limitations of using weblogs as a source of data. Important information about the patient, especially age, was often not reported. The stories were from public blogs and written by people who were not given specific instructions about which details to include. This creates a fragmentary data problem that is inherent in this type of research. Additionally, the StoryUpgrade system does not provide a complete picture of all stroke experiences narrated on the Web. The system does not find all stories posted to weblogs, and as new technologies emerge for sharing personal experiences (eg, platforms such as Twitter and Facebook), additional techniques will be required to capture these stories. With respect to patient age, the distribution of ages that were included in stories showed overrepresentation of younger adult patients and very few patients older than 76 years. This contrasts with the monotonic increase in risk of stroke that occurs with age during adulthood [17,19]. The atypical representation of relatively young adult patients in weblogs may reflect, in part, the surprise and shock when a relatively young adult suffers a stroke, an illness associated with old age. Such an emotional response may motivate a blog. The most important factor for the observed age distribution in this study, however, is likely that younger adults use weblogs more than older adults [26] and adults aged 65 years and older use the Internet substantially less than younger adults.
Conclusions
Our results demonstrate that our method of using weblogs as a source of data on stroke experiences can produce interesting new findings that have important implications for understanding sex differences and that generate hypotheses to test in future research. Older adults’ rapidly increasing use of the Internet [33] suggests that their representation in future Internet research will only grow, reducing a limitation of the present research. Using weblogs to collect data for medical research has the advantage of being relatively fast and inexpensive because it greatly reduces the time and cost of gathering data, relative to hospital studies. The price for this, however, is that data are fragmentary without a standard format for generating data.
Finally, the description of symptoms in blogs is important in terms of testing sex differences, but also for the insight it provides into the nature of stroke symptoms communicated to people who frequent weblogs or search the Internet to obtain information about strokes. That is, the Internet has become a key destination for people seeking information about disease [34]; thus, stories in blogs are likely to influence how people conceptualize stroke symptoms.
Overall, we see an important place for techniques such as these in medical research. They provide health scientists with a useful effective tool to explore medical issues. Very quickly, a health researcher can examine the experiences of people confronted with a medical issue of interest. Although these experiences will be colored by biases introduced by the query process and the population of bloggers, the information gleaned may be useful to formulate new questions and hypotheses that warrant additional investigation. Without the time and expense required for a full-scale traditional hospital study, health professionals can leverage the experiences of Web users to formulate promising avenues for future research.
Acknowledgments
The authors thank Lewis Morgenstern, MD for sharing with us his knowledge of sex differences in stroke and stimulating the development of this study. The projects or efforts depicted were or are sponsored in part by the US Army. The content or information presented does not necessarily reflect the position or the policy of the Government, and no official endorsement should be inferred.
Multimedia Appendix 1
Prototype story used for initial search query of blogs.
Footnotes
Conflicts of Interest: None declared.
References
- 1.Christensen H, Calear AL, Andersson G, Thorndike FP, Tait RJ. Beyond efficacy: the depth and diversity of current internet Interventions. J Med Internet Res. 2012;14(3):e92. doi: 10.2196/jmir.2206. http://www.jmir.org/2012/3/e92/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bernardo TM, Rajic A, Young I, Robiadek K, Pham MT, Funk JA. Scoping review on search queries and social media for disease surveillance: a chronology of innovation. J Med Internet Res. 2013;15(7):e147. doi: 10.2196/jmir.2740. http://www.jmir.org/2013/7/e147/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Eysenbach G. Infodemiology: tracking flu-related searches on the web for syndromic surveillance. AMIA Annu Symp Proc. 2006:244–8. http://europepmc.org/abstract/MED/17238340. [PMC free article] [PubMed] [Google Scholar]
- 4.Marcus MA, Westra HA, Eastwood JD, Barnes KL, Mobilizing Minds Research Group What are young adults saying about mental health? An analysis of Internet blogs. J Med Internet Res. 2012;14(1):e17. doi: 10.2196/jmir.1868. http://www.jmir.org/2012/1/e17/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Eysenbach G. Infodemiology and infoveillance: framework for an emerging set of public health informatics methods to analyze search, communication and publication behavior on the Internet. J Med Internet Res. 2009;11(1):e11. doi: 10.2196/jmir.1157. http://www.jmir.org/2009/1/e11/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Foerch C, Misselwitz B, Humpich M, Steinmetz H, Neumann-Haefelin T, Sitzer M, Arbeitsgruppe Schlaganfall Hessen Sex disparity in the access of elderly patients to acute stroke care. Stroke. 2007 Jul;38(7):2123–6. doi: 10.1161/STROKEAHA.106.478495. http://stroke.ahajournals.org/cgi/pmidlookup?view=long&pmid=17525398. [DOI] [PubMed] [Google Scholar]
- 7.Reeves MJ, Bushnell CD, Howard G, Gargano JW, Duncan PW, Lynch G, Khatiwoda A, Lisabeth L. Sex differences in stroke: epidemiology, clinical presentation, medical care, and outcomes. Lancet Neurol. 2008 Oct;7(10):915–26. doi: 10.1016/S1474-4422(08)70193-5. http://europepmc.org/abstract/MED/18722812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gargano JW, Wehner S, Reeves MJ. Do presenting symptoms explain sex differences in emergency department delays among patients with acute stroke? Stroke. 2009 Apr;40(4):1114–20. doi: 10.1161/STROKEAHA.108.543116. http://stroke.ahajournals.org/cgi/pmidlookup?view=long&pmid=19211483. [DOI] [PubMed] [Google Scholar]
- 9.Turtzo LC, McCullough LD. Sex differences in stroke. Cerebrovasc Dis. 2008;26(5):462–74. doi: 10.1159/000155983. http://europepmc.org/abstract/MED/18810232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Smith MA, Lisabeth LD, Brown DL, Morgenstern LB. Gender comparisons of diagnostic evaluation for ischemic stroke patients. Neurology. 2005 Sep 27;65(6):855–8. doi: 10.1212/01.wnl.0000176054.72325.0f. [DOI] [PubMed] [Google Scholar]
- 11.Di Carlo A, Lamassa M, Baldereschi M, Pracucci G, Basile AM, Wolfe CD, Giroud M, Rudd A, Ghetti A, Inzitari D, European BIOMED Study of Stroke Care Group Sex differences in the clinical presentation, resource use, and 3-month outcome of acute stroke in Europe: data from a multicenter multinational hospital-based registry. Stroke. 2003 May;34(5):1114–9. doi: 10.1161/01.STR.0000068410.07397.D7. http://stroke.ahajournals.org/cgi/pmidlookup?view=long&pmid=12690218. [DOI] [PubMed] [Google Scholar]
- 12.Di Carlo A, Lamassa M, Consoli D, Inzitari D, Gall SL, Donnan G, Dewey H, Thrift A. Sex differences in presentation, severity, and management of stroke in a population-based study. Neurology. 2010 Aug 17;75(7):670–1; author reply 671. doi: 10.1212/WNL.0b013e3181ec68b5. [DOI] [PubMed] [Google Scholar]
- 13.Niewada M, Kobayashi A, Sandercock PA, Kamiński B, Członkowska A, International Stroke Trial Collaborative Group Influence of gender on baseline features and clinical outcomes among 17,370 patients with confirmed ischaemic stroke in the international stroke trial. Neuroepidemiology. 2005;24(3):123–8. doi: 10.1159/000082999. [DOI] [PubMed] [Google Scholar]
- 14.Petrea RE, Beiser AS, Seshadri S, Kelly-Hayes M, Kase CS, Wolf PA. Gender differences in stroke incidence and poststroke disability in the Framingham heart study. Stroke. 2009 Apr;40(4):1032–7. doi: 10.1161/STROKEAHA.108.542894. http://stroke.ahajournals.org/cgi/pmidlookup?view=long&pmid=19211484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Labiche LA, Chan W, Saldin KR, Morgenstern LB. Sex and acute stroke presentation. Ann Emerg Med. 2002 Nov;40(5):453–60. doi: 10.1067/mem.2002.128682. [DOI] [PubMed] [Google Scholar]
- 16.Stuart-Shor EM, Wellenius GA, DelloIacono DM, Mittleman MA. Gender differences in presenting and prodromal stroke symptoms. Stroke. 2009 Apr;40(4):1121–6. doi: 10.1161/STROKEAHA.108.543371. http://stroke.ahajournals.org/cgi/pmidlookup?view=long&pmid=19211480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB, American Heart Association Statistics Committee Stroke Statistics Subcommittee Heart disease and stroke statistics--2012 update: a report from the American Heart Association. Circulation. 2012 Jan 3;125(1):e2–e220. doi: 10.1161/CIR.0b013e31823ac046. http://circ.ahajournals.org/cgi/pmidlookup?view=long&pmid=22179539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lisabeth LD, Brown DL, Hughes R, Majersik JJ, Morgenstern LB. Acute stroke symptoms: comparing women and men. Stroke. 2009 Jun;40(6):2031–6. doi: 10.1161/STROKEAHA.109.546812. http://stroke.ahajournals.org/cgi/pmidlookup?view=long&pmid=19228858. [DOI] [PubMed] [Google Scholar]
- 19.Persky RW, Turtzo LC, McCullough LD. Stroke in women: disparities and outcomes. Curr Cardiol Rep. 2010 Jan;12(1):6–13. doi: 10.1007/s11886-009-0080-2. http://europepmc.org/abstract/MED/20425178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tentschert S, Wimmer R, Greisenegger S, Lang W, Lalouschek W. Headache at stroke onset in 2196 patients with ischemic stroke or transient ischemic attack. Stroke. 2005 Feb;36(2):e1–3. doi: 10.1161/01.STR.0000151360.03567.2b. http://stroke.ahajournals.org/cgi/pmidlookup?view=long&pmid=15604424. [DOI] [PubMed] [Google Scholar]
- 21.Vestergaard K, Andersen G, Nielsen MI, Jensen TS. Headache in stroke. Stroke. 1993 Nov;24(11):1621–4. doi: 10.1161/01.str.24.11.1621. http://stroke.ahajournals.org/cgi/pmidlookup?view=long&pmid=8236332. [DOI] [PubMed] [Google Scholar]
- 22.Glader EL, Stegmayr B, Norrving B, Terént A, Hulter-Asberg K, Wester PO, Asplund K, Riks-Stroke Collaboration Sex differences in management and outcome after stroke: a Swedish national perspective. Stroke. 2003 Aug;34(8):1970–5. doi: 10.1161/01.STR.0000083534.81284.C5. http://stroke.ahajournals.org/cgi/pmidlookup?view=long&pmid=12855818. [DOI] [PubMed] [Google Scholar]
- 23.Jerath NU, Reddy C, Freeman WD, Jerath AU, Brown RD. Gender differences in presenting signs and symptoms of acute ischemic stroke: a population-based study. Gend Med. 2011 Oct;8(5):312–9. doi: 10.1016/j.genm.2011.08.001. http://europepmc.org/abstract/MED/21925968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Roquer J, Campello AR, Gomis M. Sex differences in first-ever acute stroke. Stroke. 2003 Jul;34(7):1581–5. doi: 10.1161/01.STR.0000078562.82918.F6. http://stroke.ahajournals.org/cgi/pmidlookup?view=long&pmid=12805490. [DOI] [PubMed] [Google Scholar]
- 25.Rathore SS, Hinn AR, Cooper LS, Tyroler HA, Rosamond WD. Characterization of incident stroke signs and symptoms: findings from the atherosclerosis risk in communities study. Stroke. 2002 Nov;33(11):2718–21. doi: 10.1161/01.str.0000035286.87503.31. http://stroke.ahajournals.org/cgi/pmidlookup?view=long&pmid=12411667. [DOI] [PubMed] [Google Scholar]
- 26.Schler J, Koppel M, Argamon S, Pennebaker J. Effects of age and gender on blogging. Proceedings of AAAI Spring Symposium on Computational Approaches for Analyzing Weblogs; March 27-29, 2006; Palo Alto, CA. 2006. pp. 199–205. http://www.aaai.org/Papers/Symposia/Spring/2006/SS-06-03/SS06-03-039.pdf. [Google Scholar]
- 27.Gordon A, Swanson R. StoryUpgrade: Finding stories in weblogs. Proceedings of AAAI International Conference on Weblogs and Social Media; March 31–April 2, 2008; Seattle, WA. 2008. Mar 31, http://www.aaai.org/Papers/ICWSM/2008/ICWSM08-037.pdf. [Google Scholar]
- 28.Gordon A, Swanson R. Identifying personal stories in millions of weblog entries. Third International Conference on Weblogs and Social Media, Data Challenge Workshop; May 20, 2009; San Jose, CA. 2009. May 20, http://www.aaai.org/Papers/Workshops/2009/WS-09-01/WS09-01-003.pdf. [Google Scholar]
- 29.Rocchio J. Relevance feedback in information retrieval. In: Salton G, editor. The SMART Retrieval System: Experiments in Automatic Document Processing. Upper Saddle River, NJ: Prentice Hall; 1971. pp. 313–323. [Google Scholar]
- 30.Gordon A, Wienberg C, Sood S. Different strokes of different folks: Searching for health narratives in weblogs. Proceedings of the ASE/IEEE International Conference on Social Computing; September 3-6, 2012; Amsterdam. 2012. http://ieeexplore.ieee.org/xpl/login.jsp?tp=&arnumber=6406391&url=http%3A%2F%2Fieeexplore.ieee.org%2Fstamp%2Fstamp.jsp%3Ftp%3D%26arnumber%3D6406391. [Google Scholar]
- 31.American Stroke Association. [2014-03-07]. Stroke warning signs http://www.strokeassociation.org/STROKEORG/WarningSigns/Stroke-Warning-Signs-and-Symptoms_UCM_308528_SubHomePage.jsp.
- 32.Efstathiou SP, Tsioulos DI, Zacharos ID, Tsiakou AG, Mitromaras AG, Mastorantonakis SE, Pefanis AV, Mountokalakis T. A new classification tool for clinical differentiation between haemorrhagic and ischaemic stroke. J Intern Med. 2002 Aug;252(2):121–9. doi: 10.1046/j.1365-2796.2002.01013.x. [DOI] [PubMed] [Google Scholar]
- 33.Zickuhr K, Madden M. Older adults and internet use. Washington, DC: Pew Internet & American Life Project; 2012. Jun 06, [2014-03-03]. http://pewinternet.org/~/media//Files/Reports/2012/PIP_Older_adults_and_internet_use.pdf. [Google Scholar]
- 34.Cohen RA, Stussman B. Centers for Disease Control and Prevention. 2009. [2014-03-02]. Health E-Stat: Health information technology use among men and women aged 18-64: Early release of estimates from the National Health Interview Survey, January-June 2009 http://www.cdc.gov/nchs/data/hestat/healthinfo2009/healthinfo2009.htm.