

Abstract
Background:
Intravenous patient-controlled analgesia (PCA) with morphine is commonly used for post-operative pain after major surgery. Ketamine has analgesic property at lower doses, and in combination with opioids it could have synergistic effect. The aim of this study is to determine effects of the addition of ketamine to morphine for PCA after orthopedic surgery.
Materials and Methods:
In this double-blind randomized clinical trial, 60 patients were randomly allocated to receive PCA consisting: Group 1 (morphine 0.2 mg/ml), Group 2 (morphine 0.2 mg/ml + ketamine 1 mg/ml), and Group 3 (morphine 0.1 mg/ml + ketamine 2 mg/ml). In this, anesthesiologists managed study, patients had orthopedic surgery. Assessments were made at 24 h and 48 h post-operatively. Visual analog scale (VAS) was used for recording pain score. PCA morphine use was recorded at 24 h and 48 h. VAS scores over 48 h were analyzed with analysis of variance for repeated measures. Significance level was taken as 0.05.
Results:
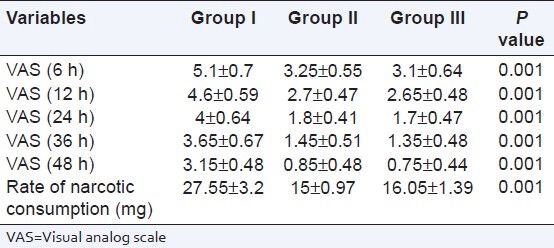
There is no significant difference between demographic information of the three groups (P > 0.05). Control of pain in Group 2 and Group 3 was better than in Group 1 (only morphine) (P = 0.001) but there was no significant difference between Group 2 and Group 3 (P > 0.05). Rate of narcotic consumption in groups 2 and 3 was significantly lower than Group 1 (P < 0.05).
Conclusion:
After orthopedic surgery, the addition of ketamine to morphine for intravenous PCA was superior to Intravenous PCA opioid alone. The combination induces a significant reduction in pain score and cumulative morphine consumption.
Keywords: Intravenous patient-controlled analgesia, ketamine, morphine, orthopedic surgery
INTRODUCTION
Intravenous patient-controlled analgesia (PCA) with morphine is commonly used for post-operative pain after major surgery. Narcotic drugs by inhibiting the release of Substance P in spinal cord and also, with direct effects on opiate receptors in the posterior horn of the spinal cord can cause analgesia.[1]
Due to the adverse effects associated with opioids (such as nausea, respiratory depression, tolerance and sedation), it is necessary to reduce opioid dosage and improve the quality of analgesia, by the use of adjuvant drugs.[2,3] In experimental trials, ketamine has been shown to prevent opioid tolerance, and lower morphine consumption. Low-dose ketamine has analgesic properties and when used with opioids can be synergistic and may antagonize the effect on the NMDA receptors with magnesium-dependent block of channels.[4,5]
Several studies have shown the effects of Ketamine in improving drug induced analgesia.[6,7,8] This study was designed to determine if the addition of ketamine to morphine for Intravenous PCA results in increased analgesic efficacy and lower pain scores compared with morphine PCA alone after orthopedic surgery. This study also explored the possibility of reducing the dose of morphine while maintaining analgesia.
MATERIALS AND METHODS
This is a double-blind clinical trial. After obtaining written, informed consent, 60 patients were randomly allocated to receive PCA post-operatively, consisting: Group 1 (morphine 0.2 mg/ml), Group 2 (morphine 0.2 mg/ml + ketamine 1 mg/ml), and Group 3 (morphine 0.1 mg/ml + ketamine 2 mg/ml). Patients were ASA physical status I-II, aged 20-60 and underwent orthopedic surgery.
Auto fuser post-operative pain control pump with 100 ml volume (Bolus 2 cc, Infusion 5 cc in hour and duration 60 min) was connected to patients in recovery unit. Pain score of patient recorded by visual analog scale (VAS), Sedation score by Ramsey Sedation score (0-5) and incidence of nausea and vomiting by N and V score (1-4) at hours 6-12-24-36-48 after pump connection and registered in designed forms. In cases with VAS higher than 3 or sedation score zero, drug dose was increased 20% and 2 mg morphine was injected for patients. In cases with VAS = 0 and (or) drug side-effects the dose decreased about 20%. In cases with nausea and vomiting metoclopramide (10 mg) was administered.
After 2 day, according to clinical condition and patient satisfaction the drug dose was decreased slowly and stopped. The necessary information such as age, sex, anesthesia method, time of surgery, VAS score and sedation score, nausea, vomiting and other complications were noted in the designed forms.
We used SPSS.15 software for analysis of data using mean (± SD), ANOVA and Chi-square tests. P < 0.05 was considered significant.
RESULTS
Age, sex and duration of surgery were similar in patients of the three groups (P > 0.05). At the end of the study the differences in VAS score and rate of drug consumption was statistically significant between patients in three groups (P = 0.001) [Table 1].
Table 1.
Compare pain score visual analog scale and rate of drug consumption in three groups
Rate of nausea, vomiting and other complications did not have statistically significant differences between patients in three groups (P > 0.05).
DISCUSSION
The objective of this review was to compare the efficacy and safety of intravenous patient-controlled opioid and ketamine to with that of opioid alone for the management of acute post-operative pain. Six studies have shown that the addition of ketamine to morphine resulted in improved post-operative analgesia and five have shown no improvement.[1,9,10,11,12,13,14,15,16,17,18]
This study showed that using low-dose of ketamine with morphine in PCA can reduce post-operative pain scores and reduce the rate of drug consumption. Adding ketamine has significant effect on VAS scores and drug dose (P = 0.001) due to analgesia property of this drug and possibly due to the effects of drug on cholinergic and mono aminergic mechanisms.[19] On the other hand ketamine can prevent acute tolerance to drugs that could contribute to the decrease in the morphine consumption.[20,21] In fact, nociceptive stimulation can cause activation of NMDA receptors, worsening the post-operative pain and by adding ketamine, this effect may be aborted.[21] The results of our study mimic those obtained in other studies on this combination.
Six studies have in the past shown improved post-operative analgesia with the addition of ketamine to opioids, which our study also shows.[11,12,13,15,16,18] Five showed no significant clinical improvement.[1,9,10,14,17] Six studies showed a statistically significant decrease in pain intensity with ketamine compared with morphine alone.[9,12,13,14,16,18] Four studies found no improvement in pain control when adding ketamine to morphine.[1,10,14,17] Six studies found a statistically significant decrease in morphine consumption in the ketamine group and five did not.[1,9,10,14,17] Three studies found a statistically shorter duration of PCA use in the ketamine group compared with the morphine group.[9,12,16]
In the Dickenson et al., study, mean Ketamine dose used was 1.2 mg/h and adding ketamine has dramatic effect after elective Micro-discectomy.[22] In the Reeves et al., study, mean of used ketamine in firstly 24 h after major abdominal surgery was 3.2 mg/h but they did not find any effect.[17] Adriaenssens et al., showed that Ketamine 10 mg/h has a decreasing effect on drug dose and nausea after abdominal surgery.[23] In this study, there is no significant difference in complications such as sedation, nausea and vomiting and sleep disorders between three groups (P > 0.05). The incidence of sedation in group 3 was higher than other groups because of the high-dose of ketamine. Weinbroum et al., showed that sedation rate in Ketamine group compared to morphine only group is low and analgesia is better for patient,[8] which is similar with our study result.
In another study, the rate of nausea and vomiting in ketamine group is lower than morphine alone group[24] that is similar to our study. In yet another study, the rate of sleep disorder and sedation in ketamine group was more than morphine group but not statistically significant.[17] In seven studies, opioid-related side-effects were statistically significantly higher in the morphine group compared with the ketamine group.[10,11,12,13,14,16] Side-effects included nausea, pruritus, sedation, urinary retention >24 h, and desaturation.[10,11,12,13,15,16] Four studies did not find any statistically significant difference[9,17,18] which is similar to our study results.
CONCLUSION
Results showed that adding low-dose ketamine to morphine in PCA, can lead to better control of pain in patients after orthopedic surgery and decrease rate of narcotic consumption. The combination shows a significant reduction in pain score and cumulative morphine consumption. The benefit of adding ketamine to morphine in intravenous PCA after surgery remains unclear and larger double-blinded randomized studies are required to confirm these findings in future.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Sveticic G, Farzanegan F, Zmoos P, Zmoos S, Eichenberger U, Curatolo M. Is the combination of morphine with ketamine better than morphine alone for postoperative intravenous patient-controlled analgesia? Anesth Analg. 2008;106:287–93. doi: 10.1213/01.ane.0000289637.11065.8f. [DOI] [PubMed] [Google Scholar]
- 2.Guyton JL. Fractures of hip, acetabulum, and pelvis. In: Canale ST, editor. Campbell's operative orthopedics. 9th ed. St. Louis: Mosby; 1998. pp. 2181–276. [Google Scholar]
- 3.Paqueron X, Lumbroso A, Mergoni P, Aubrun F, Langeron O, Coriat P, et al. Is morphine-induced sedation synonymous with analgesia during intravenous morphine titration? Br J Anaesth. 2002;89:697–701. [PubMed] [Google Scholar]
- 4.Alvarez P, Saavedra G, Hernández A, Paeile C, Pelissier T. Synergistic antinociceptive effects of ketamine and morphine in the orofacial capsaicin test in the rat. Anesthesiology. 2003;99:969–75. doi: 10.1097/00000542-200310000-00033. [DOI] [PubMed] [Google Scholar]
- 5.Richebé P, Rivat C, Rivalan B, Maurette P, Simonnet G. Low doses ketamine: Antihyperalgesic drug, non-analgesic. Ann Fr Anesth Reanim. 2005;24:1349–59. doi: 10.1016/j.annfar.2005.07.069. [DOI] [PubMed] [Google Scholar]
- 6.Kapfer B, Alfonsi P, Guignard B, Sessler DI, Chauvin M. Nefopam and ketamine comparably enhance postoperative analgesia. Anesth Analg. 2005;100:169–74. doi: 10.1213/01.ANE.0000138037.19757.ED. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Suzuki M, Tsueda K, Lansing PS, Tolan MM, Fuhrman TM, Ignacio CI, et al. Small-dose ketamine enhances morphine-induced analgesia after outpatient surgery. Anesth Analg. 1999;89:98–103. doi: 10.1097/00000539-199907000-00017. [DOI] [PubMed] [Google Scholar]
- 8.Weinbroum AA. A single small dose of postoperative ketamine provides rapid and sustained improvement in morphine analgesia in the presence of morphine-resistant pain. Anesth Analg. 2003;96:789–95. doi: 10.1213/01.ANE.0000048088.17761.B4. [DOI] [PubMed] [Google Scholar]
- 9.Burstal R, Danjoux G, Hayes C, Lantry G. PCA ketamine and morphine after abdominal hysterectomy. Anaesth Intensive Care. 2001;29:246–51. doi: 10.1177/0310057X0102900304. [DOI] [PubMed] [Google Scholar]
- 10.Hercock T, Gillham MJ, Sleigh J, Jones SF. The addition of ketamine to patient-controlled morphine analgesia does not improve quality of analgesia after total abdominal hysterectomy. Acute Pain. 1999;2:68–72. [Google Scholar]
- 11.Javery KB, Ussery TW, Steger HG, Colclough GW. Comparison of morphine and morphine with ketamine for postoperative analgesia. Can J Anaesth. 1996;43:212–5. doi: 10.1007/BF03011736. [DOI] [PubMed] [Google Scholar]
- 12.Kollender Y, Bickels J, Stocki D, Maruoani N, Chazan S, Nirkin A, et al. Subanaesthetic ketamine spares postoperative morphine and controls pain better than standard morphine does alone in orthopaedic-oncological patients. Eur J Cancer. 2008;44:954–62. doi: 10.1016/j.ejca.2008.02.021. [DOI] [PubMed] [Google Scholar]
- 13.Michelet P, Guervilly C, Hélaine A, Avaro JP, Blayac D, Gaillat F, et al. Adding ketamine to morphine for patient-controlled analgesia after thoracic surgery: Influence on morphine consumption, respiratory function, and nocturnal desaturation. Br J Anaesth. 2007;99:396–403. doi: 10.1093/bja/aem168. [DOI] [PubMed] [Google Scholar]
- 14.Murdoch CJ, Crooks BA, Miller CD. Effect of the addition of ketamine to morphine in patient-controlled analgesia. Anaesthesia. 2002;57:484–8. doi: 10.1046/j.0003-2409.2001.02409.x. [DOI] [PubMed] [Google Scholar]
- 15.Nesher N, Ekstein MP, Paz Y, Marouani N, Chazan S, Weinbroum AA. Morphine with adjuvant ketamine vs higher dose of morphine alone for immediate postthoracotomy analgesia. Chest. 2009;136:245–52. doi: 10.1378/chest.08-0246. [DOI] [PubMed] [Google Scholar]
- 16.Nesher N, Serovian I, Marouani N, Chazan S, Weinbroum AA. Ketamine spares morphine consumption after transthoracic lung and heart surgery without adverse hemodynamic effects. Pharmacol Res. 2008;58:38–44. doi: 10.1016/j.phrs.2008.06.003. [DOI] [PubMed] [Google Scholar]
- 17.Reeves M, Lindholm DE, Myles PS, Fletcher H, Hunt JO. Adding ketamine to morphine for patient-controlled analgesia after major abdominal surgery: A double-blinded, randomized controlled trial. Anesth Analg. 2001;93:116–20. doi: 10.1097/00000539-200107000-00025. [DOI] [PubMed] [Google Scholar]
- 18.Unlügenç H, Ozalevli M, Güler T, Iºik G. Postoperative pain management with intravenous patient-controlled morphine: Comparison of the effect of adding magnesium or ketamine. Eur J Anaesthesiol. 2003;20:416–21. doi: 10.1017/s0265021503000644. [DOI] [PubMed] [Google Scholar]
- 19.Schmid RL, Sandler AN, Katz J. Use and efficacy of low-dose ketamine in the management of acute postoperative pain: A review of current techniques and outcomes. Pain. 1999;82:111–25. doi: 10.1016/S0304-3959(99)00044-5. [DOI] [PubMed] [Google Scholar]
- 20.Miyamoto H, Saito Y, Kirihara Y, Hara K, Sakura S, Kosaka Y. Spinal coadministration of ketamine reduces the development of tolerance to visceral as well as somatic antinociception during spinal morphine infusion. Anesth Analg. 2000;90:136–41. doi: 10.1097/00000539-200001000-00030. [DOI] [PubMed] [Google Scholar]
- 21.Joly V, Richebe P, Guignard B, Fletcher D, Maurette P, Sessler DI, et al. Remifentanil-induced postoperative hyperalgesia and its prevention with small-dose ketamine. Anesthesiology. 2005;103:147–55. doi: 10.1097/00000542-200507000-00022. [DOI] [PubMed] [Google Scholar]
- 22.Dickenson AH. NMDA receptor antagonists: Interactions with opioids. Acta Anaesthesiol Scand. 1997;41:112–5. doi: 10.1111/j.1399-6576.1997.tb04624.x. [DOI] [PubMed] [Google Scholar]
- 23.Adriaenssens G, Vermeyen KM, Hoffmann VL, Mertens E, Adriaensen HF. Postoperative analgesia with i.v. patient-controlled morphine: Effect of adding ketamine. Br J Anaesth. 1999;83:393–6. doi: 10.1093/bja/83.3.393. [DOI] [PubMed] [Google Scholar]
- 24.Bell RF, Dahl JB, Moore RA, Kalso E. Peri-operative ketamine for acute post-operative pain: A quantitative and qualitative systematic review (Cochrane review) Acta Anaesthesiol Scand. 2005;49:1405–28. doi: 10.1111/j.1399-6576.2005.00814.x. [DOI] [PubMed] [Google Scholar]