

Abstract
VACTERL association (OMIM 192350) is a non-random combination of multiple congenital malformations including vertebral, anal, cardiac, tracheoesophageal, renal and limb anomalies. The wide spectrum of defects suggests the occurrence of defective development during early embryogenesis. The authors report a case of a complex polymalformative association detected by ultrasound in the first trimester of pregnancy. The ensuing fetal study revealed the presence of vertebral, anorectal, renal and limb anomalies and therefore was considered a case of VACTERL association. This complex association generally entails a poor prognosis. Its early detection allows discussion of management options, including medical termination of pregnancy.
Key words: VACTERL association, VATER association, first trimester diagnosis
Introduction
Definition and prevalence
VACTERL (Vertebral defects, Anal atresia, Cardiovascular malformation, Tracheo-Esophageal fistula with esophageal atresia, Radial/Renal dysplasia and Limb anomalies) is a non-random and typically sporadic association of malformations in structures derived from the embryonic mesoderm.
Studies have estimated a prevalence of 1:10,000 to 1:40,000 newborns.1
In 1972 Quan and Smith first proposed this association,2 initially with the acronym of VATER (V, vertebral defects; A, anal atresia; TE, tracheoesophageal fistula with esophageal atresia; R, radial dysplasia).
VACTERL is an acronym for an expanded definition of the association that includes cardiac (C) and Renal (R) malformations, and additional limb anomalies (L) other than radial dysplasia.3
Vertebral anomalies, which usually consist of absent or dysplastic vertebrae, have been reported in 60-80% of patients. Vertebral defects are not easily detected by prenatal ultrasonography.
Anal atresia is found in up to 90% of patients. This defect is rarely diagnosable in utero. Occasionally, distended bowel can be visualized, more likely beyond 27 weeks. However, anal atresia detection by ultrasound has already been reported at 12 weeks of gestation.4
Cardiac malformations occur in 40-80% of cases.1 The most frequent cardiac malformations include ventricular septal defects, atrial defects and tetralogy of Fallot.5
Approximately 50 to 80% of patients present with tracheoesophageal fistula, which can be suspected in utero in the presence of polyhydramnios or absent gastric bubble.
Renal anomalies, which occur in up to 80% of cases, can include unilateral or bilateral renal agenesis, horseshoe kidney and cystic and/or dysplastic kidneys.6
Limb defects are present in up to 50% of cases. Although limb malformations were classically defined as radial anomalies, VACTERL association currently encompasses other limb anomalies, as polydactyly, syndactyly and lower limb defects.5
Genitourinary anomalies, although not considered one of the component features, are a subset of malformations frequently observed in VACTERL association.7 Genitourinary anomalies are more commonly observed in patients also affected by malformations of lower intestinal and renal systems, but may be present in patients without the referred anomalies. Genitourinary defects described in patients with VACTERL association include ambiguous genitalia, genitourinary fistula, cryptorchidism and hypospadias.7
Defects in practically every organ system have been described in patients with VACTERL and are considered additional criteria for this association: facial asymmetry, external ear malformation, lung lobation defects, among others.
Etiology
The majority of cases are sporadic and environmental influences have been described. Maternal diabetes, in utero exposures to estrogen/ progesterone, statins, doxorubicin and lead have been implicated as environmental risk factors for this association.1,8
Mutations in sonic hedgehog pathway genes have been implicated in VACTERL association. A mutation in the homebox D13 gene (HOXD13), a downstream target of sonic hedgehog, has been identified in one patient.1,9
Diagnosis
Diagnosis of VACTERL association is based on clinical findings. Most investigators consider the presence of at least three of the cardinal features as a condition for diagnosis. However, only 1% of cases present the full spectrum of anomalies.10 Clinical presentation is diverse, ranging from mild cases undiagnosed until adulthood to severe cases that are obvious the prenatal or neonatal period.
Prenatal diagnosis is challenging considering many key features of this association are not easily detectable before birth.1 First trimester diagnosis is difficult and scarcely described in literature.11
Outcome
Neonates with VACTERL require significant surgical treatment and the quality of the care given to the newborn is crucial. Despite treatment, prognosis is generally poor but largely depends on the extension of malformations.
We report a rare case of VACTERL association in which the characteristic defects were detected in the first trimester of pregnancy.
Case Report
A 20-year-old primigravid, Caucasian woman was referred to our Fetal Medicine Unit at 11 weeks’ gestation for first trimester aneuploidy screening. Maternal blood sampling for β-HCG and PAPP-A measurement was performed on the first appointment at 11 weeks.
There was no relevant personal or family medical history or exposure to any known teratogen. She was under no medication, except folate supplementation. The couple was nonconsanguineous.
Abdominal ultrasound performed at 13 weeks of amenorrhoea revealed an intrauterine gestational sac containing a live fetus with a crown-rump length of 53 mm. A detailed sonographic examination detected caudal dysplasia with hypoplastic lower limbs (Figure 1) as well as an intra-abdominal cystic formation (Figure 2A), which was thought to correspond to the gastric bubble. The differential diagnosis of caudal regression and VACTERL association was considered.
Figure 1.

Hypoplastic lower right limb with malformed foot (arrow).
Figure 2.
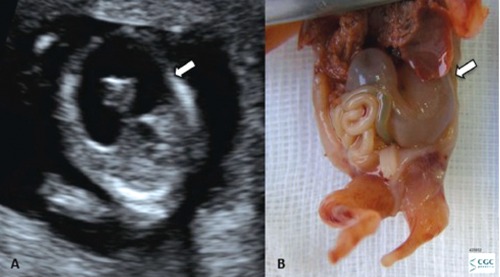
A) Ultrasound image of intra-abdominal cyst corresponding to the distended stomach (arrow); B) Fetal abdomen macroscopic examination: distended stomach (arrow).
The risk for aneuploidies, based on ultrasound and biochemical markers, was low (Trisomy 21 – 1:21163, Trisomy 13/18 – 1:37147).
Regardless the uncertainty of the definitive diagnosis, the poor prognosis was discussed and the couple opted for medical termination of pregnancy, which was performed using a combined regimen of oral Mifepristone and vaginal Misoprostol. The procedure had no reported complications. A vaginal ultrasound was performed after fetal expulsion and confirmed uterine vacuity.
The fetal patho-histological study confirmed the sonographic findings and revealed additional multiple malformations: low-set ears, hypoplastic unilobated lungs, absent spleen, hypertrophic pyloric stenosis with marked stomach distension (Figure 2B), horseshoe dysplastic and cystic kidney with a single ureter, rudimentary bladder, bilateral intraabdominal testes, urethral and anal atresia, distended bowel, recto-perineal fistula and ambiguous genitalia. Craniosynostosis, hydrocephalus and coloboma were not observed in fetal autopsy.
Asymmetric lower limbs were also noticed, with absent foot and rudimentary leg on the left and syndactyly (lobster claw malformation) of the right foot (Figures 3 and 4).
Figure 3.

Fetal lateral view: upper limbs macroscopically normal; asymmetric lower limbs with absent foot and rudimentary leg on the left. Umbilical cord with three vessels and a lateral placental insertion.
Figure 4.

Syndactyly with lobster claw malformation of the right foot.
Placental study revealed nonspecific changes with increased fibrin deposits and lateral insertion of the umbilical cord, which had three vessels. Placental weight and maturity were considered appropriate for the gestational age (Figure 3). No other alterations were found in the umbilical cord or placenta.
Fetal karyotype was normal (46 XY).
Fetal x-ray revealed absent sacral and lower lumbar vertebrae, absent lower limb bones on the left and hypoplastic right femur and tibia as well as absent right fibula. Absent pelvic bones on the left and hypoplastic on the right were also reported (Figure 5).
Figure 5.

Fetal x-ray revealing absent lower limb bones on the left and hypoplastic right femur (arrow).
Discussion
Due to simultaneous occurrence of vertebral anomalies (absent sacral and lower lumbar vertebrae), anal atresia, limb defect (right tibial hypoplasia, absent lower left limb bones) and renal defects (horseshoe dysplastic cystic kidney), this complex polymalformative association represents a case of VACTERL association. There were no cardiac malformations or tracheoesophageal fistula.
Although limb malformations were classically defined as radial defects, the definition of VACTERL currently includes a wider range of limb malformations. In this specific case, despite radial ray defects were not present, a preaxial lower limb anomaly (tibial hypoplasia) was observed. Lower limb defects affect 20-35% of VACTERL patients.12 It has been described that tibial hypoplasia/aplasia represents the most common of lower limb malformations, occurring in over two thirds of patients.13
Defects of practically every organ system have been reported in association with VACTERL. 14 Minor defects commonly observed in VACTERL were also found in this case (low-set ears, lung lobation defect, genital and gonadal anomalies and lobster claw malformation of lower extremity).14,15 Although hypertrophic pyloric stenosis and asplenia are not typical features of VACTERL, such anomalies have already been described in cases of VACTERL association.7,16,17 Cryptorchidism was also observed in this case. Although it is not a feature frequently observed in VACTERL association, cryptorchidism has already been reported previously.18 These non-VACTERL anomalies observed in the present case probably represent another spectrum of the disease.
Genital anomalies were observed in this case. Several studies have suggested that genitourinary malformations could be considered a secondary feature of VACTERL association, as malformations affecting renal and genital systems often occur together due to the closely related embryological origin of both systems.19
The vast majority of cases are sporadic and only rare cases of familial links have been described. The risk of having an affected relative is low, therefore screening of first-degree relatives of an affected individual is not advocated.
Because VACTERL association consists of anomalies of multiple systems, chromosomal disorders such as trisomy 18 and trisomy 13 must be excluded by karyotype study. VACTERL association also shows some phenotypic overlap with other conditions, as DiGeorge, Feingold, Fryns, Pallister-Hall and Townes-Brocks syndromes.1
Although prenatal diagnosis is challenging, its suspicion is extremely important due to the generally poor prognosis of this association. When diagnosis before viability is possible, management options can be discussed with the couple, including medical termination of pregnancy. Early detection allows a safer termination of pregnancy, if this option is considered. Even when the decision to continue the pregnancy is taken, prenatal diagnosis is very important to improve outcome. In this cases, planning for delivery in a tertiary centre and neonatal differentiated care have impact on prognosis.
References
- 1.Solomon BD.VACTERL/VATER Association. Orphanet J Rare Dis 2011;6:56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Quan L, Smith DW.The VATER association: vertebral defects, anal atresia, thracheoesophageal fistula with esophageal atresia, radial dysplasia. Birth Defects 1972;8:75-8 [DOI] [PubMed] [Google Scholar]
- 3.Temtamy SA, Miller JD.Extending the scope of the VATER association: Definition of the VATER syndrome. J Pediatr 1974;85: 345-9 [DOI] [PubMed] [Google Scholar]
- 4.Lam YH, Shek T, Tang MH.Sonographic features of anal atresia at 12 weeks. Ultrasound Obstet Gynecol 2002;19:523-4 [DOI] [PubMed] [Google Scholar]
- 5.Salati S, Rabah S.VACTERL Association. Online J Health Allied Sci 2010;9:15 [Google Scholar]
- 6.Solomon B, Raam MS, Pineda-Alvarez DE.Analysis of genitourinary anomalies in patients with VACTERL association. Congenit Anom 2011;51:87-91 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Solomon B, Raam MS, Pineda-Alvarez DE.Analysis of genitourinary anomalies in patients with VACTERL association. Congenit Anom 2011;51:87-91 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dawrant MJ, Giles S, Bannigan J, Puri P.Adriamycin produces a reproducible teratogenic model of vertebral, anal, cardiovascular, tracheal, esophageal, renal, and limb anomalies in the mouse. J Pediatr Surg 2007;42:1652-8 [DOI] [PubMed] [Google Scholar]
- 9.OMIM: Online Mendelian Inheritance in Man. VATER Association (192350) Available from: http://www.omim.org/clinicalSynopsis/192350 Accessed: 23/10/2011
- 10.Khoury MJ, Cordero JF, Greenberg F, et al. A population study of the VACTERL association: evidence for its etiologic heterogeneity. Pediatrics 1983;71:815-20 [PubMed] [Google Scholar]
- 11.Krapp M, Geipel A, Germer U, et al. Firsttrimester sonographic diagnosis of distal urethral atresia with megalouretra in VACTERL association. Prenat Diagn 2002;22: 422-4 [DOI] [PubMed] [Google Scholar]
- 12.Jamal E, Sen C, Michie C.A guideline for investigating a suspected VACTERL association. West Lond Med J 2011;3:33-7 [Google Scholar]
- 13.Castori M, Rinaldi R, Cappellacci S, Grammatico P.Tibial developmental field defect is the most common lower limb malformation pattern in VACTERL association. Am J Med Genet 2008;146:1259-66 [DOI] [PubMed] [Google Scholar]
- 14.Jong E, Felix J, Deurloo J, et al. Non-VACTERL-type anomalies are frequent in patients with esophageal atresia/tracheoesophageal fistula and full or partial VACTERL association. Birth Defects Res 2008;82:92-7 [DOI] [PubMed] [Google Scholar]
- 15.Dusmet M, Fête F, Crusi A, Cox JN.VATER association: report of a case with three unreported malformations. J Med Genet 1988;25:57-60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ipek M, Zenciroglu A, Aydin M, et al. An uncommon association of VACTERL complex with hypertrophic pyloric stenosis and horseshoe lung. Genet Couns 2010;21:289-92 [PubMed] [Google Scholar]
- 17.Chung B, Shaffer LG, Keating S, et al. From VACTERL-H to heterotaxy: variable expressivity of ZIC3-related disorders. Am J Med Genet A 2011;155:1123-8 [DOI] [PubMed] [Google Scholar]
- 18.Solomon B, Pineda-Alvarez D, Raam M, et al. Analysis of component findings in 79 patients diagnosed with VACTERL association. Am J Med Genet A 2010;152A:2236-44 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Botto L, Khoury M, Mastroiacovo P, et al. The spectrum of congenital anomalies of the VATER association: an international study. Am J Med Genet 1997;71:8-15 [DOI] [PubMed] [Google Scholar]