

Abstract
Soft tissue injuries constitute 30-50% of all sports related injuries; however, injury to the latissimus dorsi muscle is quite rare with only a few cases reported in the literature. Herein, we describe an acute traumatic tear of the latissimus dorsi muscle in an elite track athlete, which has not been reported in the track and field sports before. The injury was caused by forceful resisted arm adduction that took place at hurdling and starting from the block. A pseudotumor appearance in the axillary region was misdiagnosed as a mass. The diagnosis was made by ultrasound alone and the patient was managed conservatively.
Key words: ultrasound, latissimus dorsi tear
Introduction
Traumatic injuries related to muscles and tendons of the shoulder girdle are common among athletes; however, injury to the latissimus dorsi (LD) muscle is quite rare.1 In this case report, we will present acute traumatic tear of the LD muscle close to the myotendinous junction in a female track and field athlete (100 m hurdler).
LD tears related to a sports activity have been reported in rock climbers,2 rodeo steer wrestlers,3 golfers,1 skiers,4,5 body builders,6 baseball players,7 tennis players,8 gymnasts, volleyball and basketball players;9 but, extensive literature search has not revealed any track athletes. This is the first LD tear ever reported in a track athlete. Unlike other cases, ultrasound (US) was used to depict the LD tear in detail and the tear was managed non-surgically in a conservative manner.
Case Report
The patient was a 27-year old female elite track and field athlete (100 m hurdler) who has been competing for the last 10 years in many games, including the Olympic games. She felt contraction around the right axillary region during a weight-training workout (snatch) and a week later, she felt sudden tearing pain after a vigorous start from the crouched position in the blocks. Pain, ecchymosis and swelling at the axilla were the most apparent complaints when she visited a physician 4 days later. Nonsterodial anti-inflammatory drugs and muscle relaxants were prescribed. However her symptoms continued and she was referred to Sports Medicine Department of a tertiary medical center with the presumptive diagnosis of axillary lymphadenopathy 6 weeks after the injury. A soft tissue swelling (3×5 cm) with a gap in the mid portion and ecchymosis along the right posterolateral axillary region was noted on physical examination (Figure 1). There was no neurologic or vascular anomaly. Shoulder adduction and internal rotation were slightly limited and painful. Manual muscle tests of isometric strength (internal rotation and adduction) were 4/5. US revealed a complete (17 mm long) tear of LD muscle close to the myotendinous junction on the right axillary region. Muscle fibers at both ends were slightly retracted and freely moving. Accompanying hematoma was quite minimal, likely due to late admittance (Figure 2).
Figure 1.

Ecchymosis, swelling and contour changes around right axillary region due to latissimus dorsi muscle tear.
Figure 2.
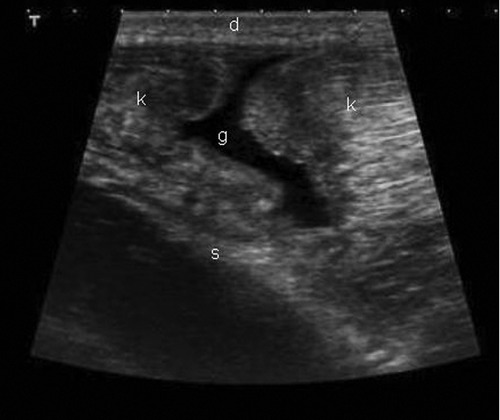
Latissimus dorsi muscle tear is clearly depicted in the longitudinal ultrasound image from posterior axillary approach. Thick latissimus muscle with fibrillar structure is lying just beneath the skin (d) and located anterior to scapula (s). Ruptured ends (k) of latissimus muscle close to the myotendinous section are retracted and the gap (g) between these parts is obvious as an anechoic center.
LD muscle is a large fan-shaped muscle that covers the whole posterolateral aspect of the trunk. The fan-shaped edge originates from multiple sites such as the thoracic, lumbar and sacral spinous processes and the iliac crest then tapers superiorly to insert as a single long tendon to the intertubercular groove of the humerus. Therefore, injuries often occur close to the insertion site9 (Figure 3). In our case, a mild grade I muscle sprain to LD, which occurred during snatch exercises, most likely predisposed the muscle to consequent tearing injury. The actual tear (grade II) occurred later when the patient was trying to generate power to run from the crouched position in the block by pushing her trunk forcibly forward while arms were extended, adducted and fixed on the ground. Similar mechanisms were described for slam-dunking in basketball and vaulting in gymnastics.4,9
Figure 3.
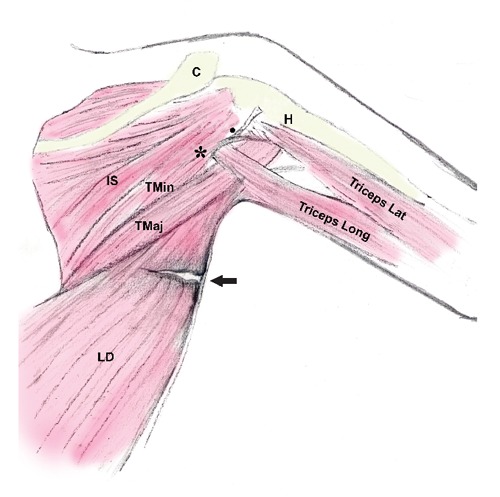
The topographic anatomy of the muscles in the dorsal aspect of the right shoulder and the location of the tear (arrow) in the latissimus dorsi muscle are illustrated in this schematic figure. The triangular space (*) which contains the scapular circumflex artery is medial to the long head of the triceps muscle between teres minor and major muscles and the quadrangular space (●) which contains and the posterior humeral circumflex vessels and the axillary nerve is lateral to the long head of the triceps muscle. The radial nerve passes through the potential space between the long and the lateral head of the triceps muscle. IS, infraspinatus muscle; TMin, teres minor muscle; TMaj, teres major muscle; LD, latissimus dorsi muscle; Triceps Long, long head of the triceps; Triceps Lat, lateral head of the triceps; C, clavicle; H, humerus.
On the basis of patient preference, a conservative approach was preferred rather than surgery; because competitions were close and requiring immediate treatment plan. Presence of an intramuscular tear in an auxiliary muscle, not actively and dominantly involved in running, increased the likelihood of a successful conservative treatment. This was a late admittance case in which 6 weeks had already passed from the time of initial injury; therefore classic physical treatment modalities [protection, rest, ice, compression and elevation (PRICE)] were not closely followed.10 Antiinflammatory and analgesic medication, kinesiotaping were prescribed. Three-plane shoulder range of motion (ROM) exercises were initiated (10-15 times × 2 sets per day). Within a week, complaints subsided, ROM was full and movements were pain free. Palpation was slightly painful and tender but no swelling was noted. The patient resumed full athletic activity after two weeks of treatment, which made 8 weeks in total after the initial injury. The patient did not have any complaint in the follow-up exam 6 weeks later.
Discussion
Latissimus dorsi muscle is one of the largest and strongest muscles of the back, having the main function of adduction, internal rotation and extension of the shoulder.4,11 The muscle is used to pull the trunk up or to lift or to pull an object forcefully towards the body and it is these exercises that render the muscle prone to traumatic injuries combined with overtraining, incompetent technique and inadequate rehabilitation.1,11 LD is used widely as a free flap for reconstructive surgery and a mild decrease (a decrease of approximately 15-25%) in strength is noted if harvested in the normal population.4,11 Most probably, injuries to LD muscle are either misdiagnosed or neglected due to lack of serious functional disturbance and problems. But in elite athletes of competitive sports, such mild decreases of strength may become important. The most significant loss is observed in the extension.2,4,5
The main difference of our case from others is that this is an intramuscular tear close to the myotendinious junction in a field/track athlete. Myotendinous junction involvement has been reported by Parks et al. in a tennis player.8 Injuries tend to involve the tendon more than the muscle. Tears involving the muscle belly are quite rare, reported in a series of traumatic injuries related to baseball7 and as a complication of anterior spinal surgery.1 Intramuscular tears tend to respond well to conservative treatment whereas surgery is often reserved for tears involving the tendon, for complete tears and avulsions in elite athletes; however, case series suggest that conservative treatment may also be a successful option in this setting.10,12-14 Whether LD muscle is actively involved or not, as in pitchers, also affects the recovery and indications for surgery. LD is often an auxiliary muscle working synergistically with teres major, posterior muscles of the deltoid and long head of triceps brachii. These muscles generally take over the function of LD and aid in recovery.15
Spinner et al.1 reported an LD and teres major muscle tendon tear in a 38-year old golf player that eventually resumed full activity in one month with conservative treatment.1 Butterwick reported a steer wrestler who resumed to competition successfully after two weeks of conservative treatment involving exercises and immobilization.12 In two separate case series consisting of 10 patients with teres major and latissimus dorsi injuries, including elite baseball pitchers, successful recoveries were reported with a conservative treatment of approximately 2 to 3 months.13,14 Henry and Scerpella et al.4 reported an acute traumatic avulsion tear of LD muscle tendon in a water skier who returned to sports activities within 6 months after surgery.4 Return to physical activity tends to take longer time after surgery (4-6 months) in comparison to the conservative treatment (1-3 months).10,14 Outcomes of surgical and nonsurgical management are both good.1,9 Surgical treatment may be opted in patients when full recovery of muscle function is intended and if the patient is willing to devote time to surgery and rehabilitation away from activities.2-4,9 In our case, the patient opted for conservative treatment including anti-inflammatory, analgesic management and physical therapy.
Most LD tears present a burning sensation and axillary pain along the posteromedial region of the arm, lasting for days. Generally, trauma and a shearing sensation are present and injury mechanism has sudden and forceful resisted arm adduction.5 Hurdling technique in athletics requires a strong pull down of contralateral arm of leading leg. Starting from the block, a strong-arm action provides inertia for an effective forward rush and LD muscle plays an important role in both actions. A pseudotumor appearance in axillary region is not uncommon after LD muscle tear.9 Anderson et al.9 have analyzed 5 cases with US, between the years 1998-2002, which were perceived as sarcoma or as a lymphadenopathy as in our case.9 Magnetic resonance imaging is widely used to diagnose LD rupture, has a larger field of view (FOV), can better differentiate the teres major and LD tendons from each other, may better depict avulsion injuries with large bone fragments and may also rule out bone edema, tumors of the humerus or scapula (osteosarcoma or osteoid osteoma) or additional injuries on the shoulder girdle.1 US is a useful diagnostic tool in the imaging of soft tissue anatomy, especially for tears and hematomas and it allows dynamic imaging while it is highly operator-dependent with a relatively small FOV.16
Conclusions
LD tears may occasionally be seen in track/field athletes and may go unrecognized. Conservative treatment is quite successful especially if LD maintains auxiliary function and if the tear is intramuscular.
References
- 1.Spinner RJ, Speer KP, Mallon WJ.Avulsion injury to the conjoined tendons of the latissimus dorsi and teres major muscles. Am J Sports Med. 1998; 26:847-9 [DOI] [PubMed] [Google Scholar]
- 2.Livesey JP, Brownson P, Wallace WA.Traumatic latissimus dorsi tendon tear. J Shoulder Elbow Surg. 2002; 11:642-4 [DOI] [PubMed] [Google Scholar]
- 3.Hiemstra LA, Butterwick D, Cooke M, Walker RE.Surgical management of latissimus dorsi rupture in a steer wrestler. Clin J Sport Med. 2007; 17:316-8 [DOI] [PubMed] [Google Scholar]
- 4.Henry JC, Scerpella TA.Acute traumatic tear of the latissimus dorsi tendon form its insertion. A case report. Am J Sports Med. 2000; 28:577-9 [DOI] [PubMed] [Google Scholar]
- 5.Lim JK, Tilford ME, Hamersly SF, Sallay PI.Surgical repair of an acute latissimus dorsi tendon avulsion using suture anchors through a single incision. Am J Sports Med. 2006; 34:1351-5 [DOI] [PubMed] [Google Scholar]
- 6.Budoff JE, Gordon L.Surgical repair of traumatic latissimus dorsi avulsion: a case report. Am J Orthop. 2000; 29:638-9 [PubMed] [Google Scholar]
- 7.Barnes DA, Tullos HS.An analysis of 100 symptomatic baseball players. Am J Sports Med. 1978; 6:62-7 [DOI] [PubMed] [Google Scholar]
- 8.Park JY, Lhee SH, Keum JS.Rupture of latissimus dorsi muscle in a tennis player. Orthopedics 2008;31 pii: orthosupersite.com/view.asp?rID=31522 [PubMed] [Google Scholar]
- 9.Anderson SE, Hertel R, Johnston JO, et al. Latissimus dorsi tendinosis and tear: imaging features of a pseudotumor of the upper limb in five patients. Am J Roentgen. 2005; 185:1145-51 [DOI] [PubMed] [Google Scholar]
- 10.Fernandes TL, Pedrinelli A, Hernandez AJ.Muscle injury: physiology, diagnostic treatment and clinical presentation. Rev Bras Orthop. 2011; 46:247-55 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Burks R, Burke W, Stevanovic M.Rehabilitation following repair of a torn latissimus dorsi tendon. Phys Ther. 2006; 86:411-23 [PubMed] [Google Scholar]
- 12.Butterwick DJ, Mohtadi NG, Meeuwisse WH, Frizzell JB.Rupture of latissimus dorsi in an athlete. Clin J Sports Med. 2003; 13:189-91 [DOI] [PubMed] [Google Scholar]
- 13.Schickendantz MS, Kaar SG, Meister K, et al. Latissimus dorsi and teres major tears in professional baseball pitchers: a case series. Am J Sports Med. 2009; 37:2016-20 [DOI] [PubMed] [Google Scholar]
- 14.Nagda SH, Cohen SB, Noonan TJ, et al. Management and outcomes of latissimus dorsi and teres major injuries in professional baseball pitchers. Am J Sports Med. 2011; 39:2181-6 [DOI] [PubMed] [Google Scholar]
- 15.Grosclaude M, Najihi N, Lädermann A, et al. Teres major muscle tear in two professional ice hockey players: cases study and literature review. Orthop Traumatol Surg Res. 2012; 98:122-5 [DOI] [PubMed] [Google Scholar]
- 16.Stainsby BE, Piper SL, Gringmuth R.Management approaches to acute muscular strain and hematoma in national level soccer players: a report of two cases. J Can Chiropr Assoc. 2012; 56:262-8 [PMC free article] [PubMed] [Google Scholar]