

Abstract
We report a 16-year-old girl with a multiple primary rhabdomyosarcoma of right upper extremity who developed contralateral breast metastasis in her clinical course. She was diagnosed to have multiple primary rhab-domyosarcoma of the right upper extremity with lung metastasis one year prior to finding a mass in her left breast. The excisional biopsy of the breast mass confirmed metastatic rhabdomyosarcoma. Despite aggressive chemotherapy and subcutaneous total mastectomy, she developed a widespread bone and lung metastasis in few months and expired. Metastatic rhabdomyosarcoma of the breast is very rare but it should be considered in adolescent females with primary alveolar rhabdomyosarcoma, specially located on an extremity.
Key words: breast, metastasis, rhabdomyosarcoma.
Introduction
Rhabdomyosarcoma is the most common soft tissue Sarcoma in childhood accounting for half of all pediatric soft tissue sarcoma. It can involve the breast as either primary or secondary. The incidence of breast metastasis in rhabdomyosarcoma is reported to be approximately 6%1 and is mainly seen in adolescent girls.2 Here, we describe a 16-year-old girl with multiple primary rhabdomyosarcoma of the upper extremity who developed contralateral breast metastasis.
Case Report
A 16-year-old woman was presented to our breast clinic with a palpable lump in the left breast. She had undergone chemotherapy because of multiple rhabdomyocarcoma of the right hand and the forearm with the right lung metastasis 11 months before. She was in remission when she found her left breast mass.
On examination, she had a 20 mm discrete palpable non-tender mass in the upper inner quadrant of the left breast. An ultrasound of the breast confirmed the presence of four well-defined hypo echoic solid masses ranging from 6 to 20 mm compatible with multiple fibro adenomas.
A fine needle aspiration biopsy (FNAB) showed some round cells, which was inconclusive. The excision of the largest mass in upper inner quadrant of the left breast was performed and a histological analysis was consistent with rhabdomyosarcoma. Subsequent staging evaluations, including abdominal ultra sound, computed tomography (CT), magnetic resonance imaging (MRI) of the extremities and bone scan did not reveal any local recurrence or new systemic metastasis. She had undergone a systemic treatment but after four cycles, she was readmitted because of a huge right axillary mass and the diffused involvement of the left breast (Figures 1 and 2). The palliative resection of the right axillary tumor and the subcutaneous mastectomy were done (Figures 3 and 4). Despite the aggressive systemic therapy, the clinical course was marked by lung metastasis and the progression of the disease.
Figure 1.

Axillary involvement and contralateral breast metastasis in 16 yr old girl with alveolar rhabdomyosarcoma of the hand and forearm.
Figure 2.

Multiple primary lesion of hand and forearm.
Figure 3.
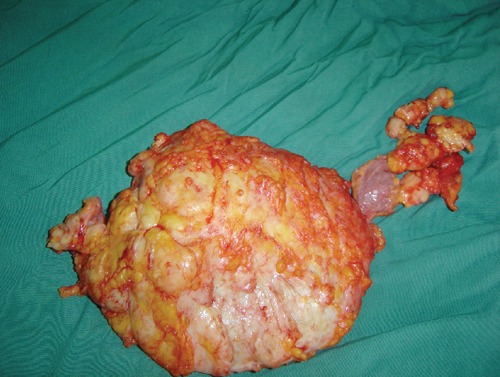
Specimen of palliative subcutaneous mastectomy.
Figure 4.
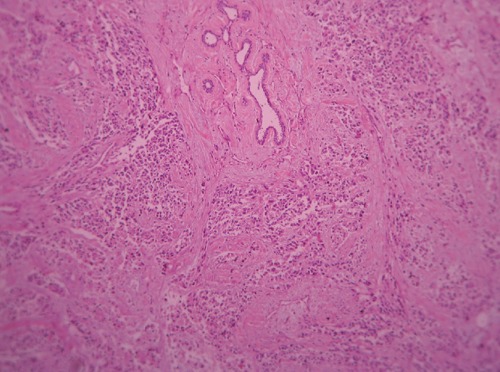
Breast's unremarkable epithelial component is seen in upper central and metastatic sarcoma in its periphery.
Discussion
Metastases to the breast from solid tumors, excluding contralateral breasts, are quite rare. The primary lesion in most cases of metastasis to the breast is melanoma, lung and ovarian carcinoma in adults and rhabdomyosarcoma in children.3,4
In one series,5 9 out of 13 pediatric cases with breast metastasis are reported to be from rhabdomyosarcoma.
Metastatic rhabdomyosarcoma of the breast usually occurs in adolescent girls and is often bilateral.1,2,6–8
As the age increases, breast is not a favorite site of metastasis because the amount of fibrous tissue increases and the blood supply decreases, probably due to hormonal states.9
Howarth reported1 seven out of 108 consecutively diagnosed patients with rhabdomyosarcoma, who had developed clinically evident metastatic tumors of the breast. Sex distribution and age of these patients indicated that the physiologic state of the breast was an important determining factor in the development of such metastasis. All these patients had primary tumors located on an extremity or the buttock.
Metastatic rhabdomyosarcoma to the breast often presents a solitary nodular mass. Multiple lesions and the diffused involvement are less common.10,11
Ultra sonograpy is the ideal imaging modality to evaluate breast lesions in children and may be used to guide a FNAB. Although their ultrasonography appearance is non-specific, they often appear as hypoechoic round or lobulated nodules with either posterior enhancement or indifferent shadowing.
CT and MRI can demonstrate the nature of these lesions. On MRI, the metastases from rhabdomyosarcoma were characterized by multiple tumors with high signal intensity on T2 – weighted images and fast annular contrast enhancement.12 MRI appeared to be the best technique for the evaluation of the residual disease after therapy.13 Positron emission tomography CT imaging can be used for primary staging and the follow up of metastasis in all pediatric solid tumors.14
Although primary rhabdomyosarcoma of the breast can be diagnosed by FNAB, the secondary involvement often needs tissue biopsy and the histological type is often alveolar. Indeed, metastatic rhabdomyosarcoma to the breast is almost confined to adolescent females having tumors with an alveolar histology.1,8 Few cases of breast metastasis from embryonal type were also reported.15–17 Rhabdomyosarcoma is treated with multidisciplinary approaches of chemotherapy, surgery and radiotherapy. For alveolar rhabdomyosarcoma, there is no established protocol of chemotherapy, and surgery plays a significant role in the treatment. Extent of surgery ranging from the excision of a mass to radical mastectomy. However, the prognosis for alveolar rhabdomyosarcoma cases is still poor. Santos Miranda et al.18 reported a long-term survival of the alveolar rhabdomyosarcoma of the maxillary sinus with breast metastasis.
We found only four reports of19–22 similar cases with alveolar rhabdomyosarcoma of the extremities in the literature. In a series of 189 patients with metastatic rhabdomyosarcoma reported by D'Angelo from Italian Soft Tissue Sarcoma Committee there were 7 adolescent with breast involvement. The primary tumor was located in the extremities in three of them. All these cases had a dismal prognosis like our case. Our patient is unique because the initial presentation of the primary lesion with multiple involvements of the hand and forearm. We conclude that adolescent females with alveolar rhabdomyosarcoma of the extremities have a risk of developing breast metastasis, which is a poor prediction of survival.
Acknowledgments:
the authors would like to thank the patient's parents because of their cooperation and the permission of this report.
References
- 1.Howarth CB, Caces JN, Pratt CB. Breast metastases in children with rhabdomyosarcoma. Cancer. 1980;46:2520–4. doi: 10.1002/1097-0142(19801201)46:11<2520::aid-cncr2820461134>3.0.co;2-h. [DOI] [PubMed] [Google Scholar]
- 2.Herrera LJ, Lugo-Vicente H. Primary embryonal rhabdomyosarcoma of the breast in an adolescent female. J Pediatr Surg. 1998;33:1582–4. doi: 10.1016/s0022-3468(98)90506-1. [DOI] [PubMed] [Google Scholar]
- 3.Shetty MR. Diagnosis and natural history of extramammary tumors metastatic to the breast. J Am Coll Surg. 1995;180:381–2. [PubMed] [Google Scholar]
- 4.Bohman LG, Bassett LW, Gold RH, Voet R. Breast metastases from extramammary malignancies. Radiology. 1982;144:309–12. doi: 10.1148/radiology.144.2.7089284. [DOI] [PubMed] [Google Scholar]
- 5.Rogers DA, Lobe TE, Rao BN, et al. Breast malignancy in children. J Pediatr Surg. 1994;29:48–51. doi: 10.1016/0022-3468(94)90521-5. [DOI] [PubMed] [Google Scholar]
- 6.Birjawi GA, Haddad MC, Tawil AN, Khoury NJ. Metastatic rhabdomyosarcoma to the breast. Eur Radiol. 2001;11:555–8. doi: 10.1007/s003300000632. [DOI] [PubMed] [Google Scholar]
- 7.Feder JM, de Paredes ES, Hogge JP, Wilken JJ. Unusual breast lesions: radiologic-pathologic correlation. Radiographics. 1999;19:11–26. doi: 10.1148/radiographics.19.suppl_1.g99oc07s11. [DOI] [PubMed] [Google Scholar]
- 8.Hays DM, Donaldsom SS, Shimada H, et al. Primary and metastatic rhabdomyosarcoma in the breast: neoplasms of adolescent females, a report from the Intergroup Rhabdomyosarcoma Study. Med Pediatr Oncol. 1997;29:181–9. doi: 10.1002/(sici)1096-911x(199709)29:3<181::aid-mpo4>3.0.co;2-9. [DOI] [PubMed] [Google Scholar]
- 9.Vergier B, Trojani M, de Mascarel I, et al. Metastases to the breast: differential diagnosis from primary breast carcinoma. J Surg Oncol. 1991;48:112–6. doi: 10.1002/jso.2930480208. [DOI] [PubMed] [Google Scholar]
- 10.Perlet C, Sittek H, Forstpointner R, et al. Metastatic to the breast from rhabdomyosarcoma: appearances on MRI. Eur Radiol. 1999;9:1113–6. doi: 10.1007/s003300050801. [DOI] [PubMed] [Google Scholar]
- 11.Garcia CJ, Espinoza A, Dinamarca V, et al. Breast US in children and adolescents. Radiographics. 2000;20:1605–12. doi: 10.1148/radiographics.20.6.g00nv171605. [DOI] [PubMed] [Google Scholar]
- 12.Paulus DD, Libshitz HI. Metastasis to the breast. Radiol Clin North Am. 1982;20:561–8. [PubMed] [Google Scholar]
- 13.Wurdinger S, Schutz K, Fuchs D, Kaiser WA. Two cases of metastases to the breast on MR Mammography. Eur Radiol. 2001;11:802–6. doi: 10.1007/s003300000636. [DOI] [PubMed] [Google Scholar]
- 14.Dausse F, Balu-Maestro C, Chapellier C, Leblanc-Talent P. Rhabdomyosarcoma of the breast. Clin Imaging. 2005;29:337–41. doi: 10.1016/j.clinimag.2005.01.028. [DOI] [PubMed] [Google Scholar]
- 15.Keorochana G, Chanplakorn P, Laohacharoensombat W, Larbeharoensub N. Spinal and bilateral breast metastases of embryonal rhabdomyosarcoma. J Med Assoc Thai. 2007;90:813–8. [PubMed] [Google Scholar]
- 16.Lai CR, Hsu CY, Tsay SH, Hung-Chiang Adult embryonal rhabdomyosarcoma metastatic to the breast and diagnosed by fine needle aspiration. A case report. Acta Cytol. 1997;41:845–8. doi: 10.1159/000332714. [DOI] [PubMed] [Google Scholar]
- 17.Santos Miranda JA, González San Segundo C, Carretero Albiñana L. [Breast metastasis from embryonal rhabdomyosarcom apropos 2 cases and a review of the literature] Rev Clin Esp. 2000;200:21–5. doi: 10.1016/s0014-2565(00)70546-7. [Article in Spanish] [DOI] [PubMed] [Google Scholar]
- 18.Persic M, Roberts JT. Alveolar rhabdomyosarcoma metastatic to the breast: Long-term survivor. Clin Oncol (R coll Radiol) 1999;11:417–8. doi: 10.1053/clon.1999.9096. [DOI] [PubMed] [Google Scholar]
- 19.Daramola AO, Banjo AA, Ajekigbe AT, Popoola AO. Metastatic alveolar rhabdomyosarcoma to the breast: A case report. Niger Postgrad Med J. 2008;15:137–40. [PubMed] [Google Scholar]
- 20.Kwan WH, Choi PH, Li CK, et al. Breast metastasis in adolescents with alveolar rhabdomyosarcoma of the extremities: report of two cases. Pediatr Hematol Oncol. 1996;13:277–85. doi: 10.3109/08880019609030828. [DOI] [PubMed] [Google Scholar]
- 21.Tan GC, Shiran MS, Hayati AR, et al. Alveolar rhabdomyosarcoma of the left hand with bilateral breast metastases in an adolescent female. J Chin Med Assoc. 2008;71:639–42. doi: 10.1016/s1726-4901(09)70007-3. [DOI] [PubMed] [Google Scholar]
- 22.D'Angelo P, Carli M, Ferrari A, et al. Breast metastases in children and adolescents with rhabdomyosarcoma: experience of the Italian Soft Tissue Sarcoma Committee. Pediatr Blood Cancer. 2010;55:1306–9. doi: 10.1002/pbc.22729. [DOI] [PubMed] [Google Scholar]