

Abstract
Retained intraocular graphite foreign bodies are uncommon. Although they are generally inert, they have been reported to cause severe inflammatory reaction and progressive damage to intraocular structures. We report a case of a six-year-old girl with a retained intraocular graphite pencil lead foreign body in the anterior chamber of the eye and discuss the various considerations in the management of such cases.
Key words: graphite, intraocular foreign body.
Introduction
Intraocular foreign bodies have been reported to constitute 18–41% of all open globe injuries.1 Organic foreign bodies are generally associated with severe inflammatory reaction and infection, while the nature of reaction elicited by inorganic foreign bodies depends on the material of the foreign body.2 Retained graphite foreign bodies in the eye are uncommon.3–7 Graphite, which is the major constituent of pencil lead, has been reported to remain inert in the eye for a long time.3 However, it has also been reported to cause severe endophthalmitis-like reaction in the eye.4 We report a rare case of retained graphite pencil tip in the anterior chamber of a six-year-old girl.
Case Report
A six-year-old girl presented to us with history of mild pain in the left eye of two days duration. The child’s mother gave a history of trauma with a graphite lead pencil about four months ago at school when she was accidentally poked in the left eye by another child. The child had not been examined by an ophthalmologist after the incident as she was apparently asymptomatic at the time.
On examination, the best corrected visual acuity was 20/20 in the right eye and 20/40 in the left eye. There was a full thickness corneal scar (Figure 1) in the left eye. A small area of iris atrophy with a sphincter tear was noted at the edge of the pupil at the 6 o’ clock position. There was a black foreign body resembling a graphite pencil lead tip, measuring about 1.5 mm in size, on the iris at the 7 o’ clock position (Figure 1). Some refractile particles were seen on the iris around the foreign body. There was no inflammatory reaction in the anterior chamber. The intraocular pressure was 14 mmHg in both eyes. Gonioscopy showed open angles with no additional foreign bodies. The lens was clear and the fundus visualized through the undilated pupil was normal. Ocular ultrasonography of the left eye did not reveal any abnormality in the posterior segment. The right eye was normal.
Figure 1.

Slit lamp photograph of the left eye showing the corneal scar and the graphite pencil lead tip on the iris.
The child was posted for foreign body removal under general anesthesia. A corneal incision was made at 5 o’ clock position with a 2.8 mm keratome. The anterior chamber was filled with 2% methyl cellulose and the foreign body (Figure 2) was removed in toto with a Bechert-McPherson forceps. The remaining graphite particles were aspirated out with a Simcoe cortex aspiration cannula using an anterior chamber maintainer. Post-operatively, the patient was put on tapering doses of topical steroids and cycloplegics. On follow up, one month later, the best corrected visual acuity in the left eye was 20/40. There was no inflammation; the lens was clear and the fundus was normal.
Figure 2.
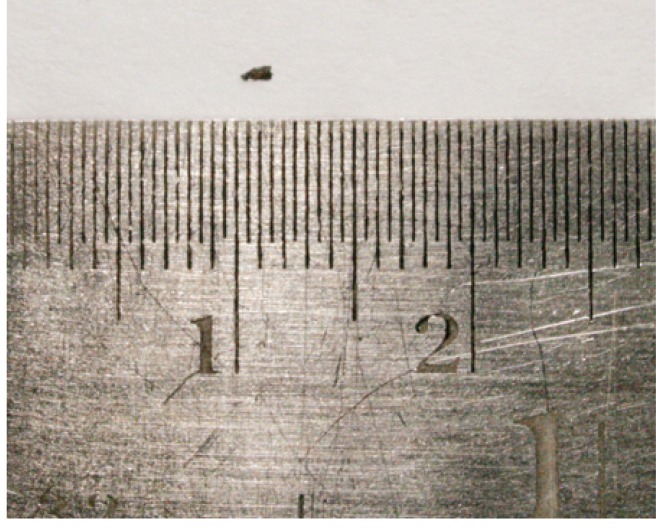
The graphite pencil lead tip that was removed from the eye.
Discussion
The reaction of the eye to a retained intraocular foreign body varies depending on its composition. Foreign bodies comprised of materials like gold, silver and platinum have been reported to remain inert in the intraocular environment.8 There are only a few reports of ocular trauma with retention of graphite pencil lead in the eye.3–7 Retained graphite has been described in the conjunctiva, cornea, angle of the anterior chamber and the posterior segment. A case of pencil-tip injury to the orbit with retained graphite foreign body associated with delayed orbital infection has also been described.9
Pencil leads are made of graphite, kaolinite, wax or other animal fat.4 In addition, a wood surround is applied to make the pencil. Graphite foreign bodies may remain inert in the eye for a long time.3 However, the potential toxicity of the other constituents of pencil lead like animal fats and clay is not clearly known. There has been a report of severe endophthalmitis-like reaction incited by retained graphite foreign bodies in the vitreous.4 In this case, it is unclear whether the reaction was induced by the other constituents of pencil lead like the aluminium in the kaolinite or if there was an associated infection.
In our case, we decided to surgically remove the intraocular foreign body in spite of the fact that it had obviously remained in the eye for some time (as evidenced by the healed corneal scar and presence of iris atrophy) without inciting an inflammatory response or causing much damage to the intraocular structures. There was a distinct possibility of causing damage to the lens and inciting an inflammatory reaction during surgical removal of the foreign body. This risk had to be weighed against that of the damage the foreign body might cause if it was left in the eye. There was a chance that the foreign body would get dislodged into the angle at a later stage and cause progressive damage to the angle structures and the cornea as in the case reported by Han et al.5
Honda et al.3 have reported a case of a five-year-old child with a graphite foreign body lodged in the peripheral retina, whom they followed up for six years with serial electroretinograms, fundus photographs and fundus fluorescein angiography.
There was no evidence of any damage to the eye caused by the foreign body at the end of their follow up. However, in our case, such meticulous follow-up would have been quite impossible as the child’s family belonged to a poor socio-economic background and the parents would not have been able to afford the cost of repeated hospital visits and investigations. Our case also differed from Honda et al.’s case in that the foreign body was in the anterior segment and therefore, was at a more accessible site. There was a higher chance of removal of the foreign body without causing damage to the intraocular structures in our case.
In conclusion, graphite foreign bodies may be retained in the eye without causing any inflammation or damage to the intraocular structures. On the other hand, there is also the possibility of progressive damage to intraocular structures by these foreign bodies due to various mechanisms. Therefore, the decision about surgical removal of the foreign body has to be made on an individual basis after taking multiple factors into consideration and estimating the risk-benefit ratio in each patient.
References
- 1.Zhang Y, Zhang M, Jiang C, Qiu HY. Intraocular foreign bodies in China: clinical characteristics, prognostic factors, and visual outcomes in 1,421 eyes. Am J Ophthalmol. 2011;152:66–73.:e73. doi: 10.1016/j.ajo.2011.01.014. [DOI] [PubMed] [Google Scholar]
- 2.Lit ES, Young LH. Anterior and posterior segment intraocular foreign bodies. Int Ophthalmol Clin. 2002;42:107–20. doi: 10.1097/00004397-200207000-00013. [DOI] [PubMed] [Google Scholar]
- 3.Honda Y, Asayama K. Intraocular graphite pencil lead without reaction. Am J Ophthalmol. 1985;99:494–5. doi: 10.1016/0002-9394(85)90031-5. [DOI] [PubMed] [Google Scholar]
- 4.Hamanaka N, Ikeda T, Inokuchi N, et al. A case of intraocular foreign body due to graphite pencil lead complicated by endophthalmitis. Ophthalmic Surg Lasers. 1999;30:229–31. [PubMed] [Google Scholar]
- 5.Han ER, Wee WR, Lee JH, Hyon JY. A case of retained graphite anterior chamber foreign body masquerading as stromal keratitis. Korean J Ophthalmol. 2011;25:128–31. doi: 10.3341/kjo.2011.25.2.128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jeng H, Whitcher JP, Margolis TP. Intracorneal graphite particles. Cornea. 2004;23:319–20. doi: 10.1097/00003226-200404000-00021. [DOI] [PubMed] [Google Scholar]
- 7.Guy JR, Rao NA. Graphite foreign body of the conjunctiva simulating melanoma. Cornea. 1985–1986;4:263–5. [PubMed] [Google Scholar]
- 8.Sihota R, Tandon R, editors. 20th ed. New Delhi: Elsivier; 2007. Parsons’ diseases of the eye. [Google Scholar]
- 9.Seider N, Gilboa M, Lautman E, Miller B. Delayed presentation of orbito-cerebral abscess caused by pencil-tip injury. Ophthal Plast Reconstr Surg. 2006;22:316–7. doi: 10.1097/01/iop.0000226920.54294.0c. [DOI] [PubMed] [Google Scholar]