

Abstract
Introduction:
Anxiety is one of the components of patient stress in the dental office and is recognized as one of the main factors that negatively affect treatment. The control of anxiety can be performed through conscious sedation, for which benzodiazepine is the drug of choice in dental practice, however present side-effects.
Objective:
The objective of the following study is to evaluate the efficacy of Valeriana officinalis L. (Valerian) for control of anxiety during the third molar surgery.
Materials and Methods:
A single oral dose of either Valerian (100 mg) or placebo was randomly administered 1 h before each surgical procedure to 20 volunteers between 17 and 31 years of age. Anxiety level was assessed by physiological parameters (blood pressure and heart rate [HR]) and the observation of signs. Descriptive analysis, Chi-square test, Friedman test, Wilcoxon test and effect size test were performed (P < 0.05).
Results:
According to the researcher's (80%) and surgeon's (75%) evaluations, the patients treated with Valerian were calmer and more relaxed during surgery. Valerian had a greater effect on the maintenance of systolic blood pressure and HR after surgery.
Conclusion:
Valerian was more effective at controlling anxiety than a placebo when used for the conscious sedation of adult patients submitted to impacted lower third molar surgery.
KEY WORDS: Anxiety, oral surgery, phytotherapy
Anxiety is one of the components of patient stress in the dental office and is recognized as one of the main factors that negatively affect treatment.[1] The control of anxiety can be performed through conscious sedation, for which benzodiazepine is the drug of choice in dental practice due to its efficacy, margin of clinical safety and ease of administration.[2,3] In Brazil, dentists do not have the habit of using conscious sedation with benzodiazepines frequently in the clinic, due to several issues, among which the deficiency in their training with regard to this type of medication.[4]
However, benzodiazepine may cause side-effects, such as rash, headache and increased effect of alcohol, or may have a paradoxical effect.[5,6] Moreover, the use of such agents requires patients to be accompanied to appointments and comes with the recommendation of not driving vehicles or operating heavy equipment while under the effect of the drug.[7] In order to minimize or avoid the side-effects of benzodiazepine, other drugs have been administered to control anxiety, such as phytotherapeutic products containing Valerian extract.
Valeriana officinalis is an herbaceous plant from the family Valerianaceae and is incorporated into a large number of phytotherapeutic products due to it anxiolytic and hypnotic properties.[8] Pharmaceutical blends containing Valerian extract have been used in a number of countries due to the lack of side-effects commonly described for benzodiazepine.[9] Recent studies have demonstrated that Valerian offers efficacy and clinical safety in the treatment of anxiety in the medical field[10] and can restrain pharmacological reactivity in situations of psychological stress induced under laboratory conditions.[11] In the field of dentistry, one study found that medication containing Valerian significantly reduced the level of anxiety in patients submitted to minor oral surgery.[12]
As few studies have assessed the use of Valerian in dentistry, well-controlled studies that can provide a greater amount of evidence regarding the efficacy of this product with regard to conscious sedation are needed. The aim of the present study was to assess the effect of Valerian for the conscious sedation of dental patients submitted to oral surgery for the bilateral extraction of impacted lower third molars.
Materials and Methods
A randomized, double-blind, placebo-controlled crossover study was carried out following approval from the Ethics Committee of the Piracicaba Dental School, Universidade Estadual de Campinas (Brazil). The study was conducted in compliance with the Helsinki Declaration and all participants signed an informed consent form after receiving an explanation of the general objectives and procedures of the study. The trial was conducted in accordance with the Consolidated Standards of Reporting Trials statement and is registered at clinicaltrials.gov with number NCT01612130.
Sample selection
A study sample comprised of 20 volunteers, of which 8 were males and 12 were females with age ranges between 17 and 31 years of age participated in the study. All subjects had been referred to the Oral-maxillofacial surgery sector of Piracicaba Dental School, Universidade Estadual de Campinas (Brazil) for the bilateral extraction of asymptomatic impacted mandibular third molars in similar positions based on the Pell and Gregory classification.[13] The medical histories revealed that no volunteer exhibited any type of general health problem. The following were the exclusion criteria: Use of any type of medication in the 15 days prior to the onset of the study; history of hypersensitivity to the drugs, substances or materials employed in the experiment; pregnancy or lactation.
Treatments
1 h prior to each surgical procedure, the participant received a single oral dose of 100 mg of Valerian or placebo (drugstore Professor Accorsi – medicinal plants, Piracicaba, SP, Brazil) in capsule form. Neither the patient researcher nor surgeons knew which medication was administrated in each surgery. The capsules had the same concentration, size and appearance and were coded as medication 1 and 2, which were only identified at the end of the experiment. Randomization was performed by the researcher, who used two envelopes to determine the medication to be employed first and the side of the face to be operated first.
In both surgeries, 4 mg of dexamethasone (Prodome Química e Farmacêutica Ltda., Campinas, SP, Brazil) were administered for the prevention of post-operative pain and swelling. Intra-oral and extra-oral antisepsis was performed with an aqueous solution of 0.12% and 2% chlorhexidine digluconate (Pharmacy compounding Proderma Ltda., Piracicaba, SP, Brazil), respectively. For local anesthesia, a maximal volume of 3.6 mL of a 2% lidocaine solution with adrenalin at 1:100.000 (DFL S.A., Rio de Janeiro, RJ, Brazil) was employed. Surgical antibiotic prophylaxis was not performed in any cases. The mandibular third molar extractions were performed by three experienced surgeons, with a 30-day interval between the two sides. The same surgical technique was employed in both surgeries.
Assessment of degree of anxiety
The degree of patient anxiety was assessed through the use of questionnaires and physical parameters. This assessment was carried out in three distinct phases:
Phase 1
Baseline: The initial appointment, 1 week prior to the scheduled date of the first surgery. The dental anxiety scale (DAS) was used to classify the participants with regard to their degree of anxiety (not anxious, mildly anxious, moderately anxious and very anxious).[14] Moreover, heart rate (HR) and systolic and diastolic blood pressure (SBP and DBP, using the auscultation method) were determined with the volunteer at rest. These measurements served as the baseline data of the physical parameters, which were also used in the assessment of anxiety.
Phase 2
During each surgery, the researcher and surgeon observed the manifestation of signs and symptoms associated to anxiety (restlessness/agitation/nervous ticks, paleness, excessive perspiration, tingling sensation in hands, feet or lips, change in breathing rhythm or depth). In the presence of one or more of these signs and symptoms, the patient was classified as anxious. If there was no manifestation of anxiety, the patient was classified as calm or relaxed. The patient's vital signs were also assessed at different times. BP and HR were determined 30 min after the administration of the medication and after 15 min of rest following the surgery.
Phase 3
At the end of each surgical procedure, the volunteers received a self-assessment questionnaire to be filled out the day following each surgery in order to assess the experience provided by both treatments (V. officinalis L. or placebo) as well as the occurrence or lack of anterograde amnesia. Moreover, possible adverse or side effects of treatment (sleepiness, dizziness, muscle relaxation, gastrointestinal problems and signs of allergy) and the patient's preference for one of the two surgical procedures were assessed 24 h after the second surgery.
Due to the possibility of some degree of respiratory depression caused by V. officinalis L., a digital pulse oximeter (Medical Supplies and Equipment CO, Houston, Texas, USA) was used to detect signs of hypoxia in susceptible patients or for simple monitoring during the surgery. The percentage of oxygen saturation was monitored during the initial appointment (baseline), 30 min after the administration of the medication and throughout the entire surgical procedure.
Statistical analysis
Data analysis was carried out using Statistical Package for Social Sciences (SPSS for Windows, version 17.0, SPSS Inc., Chicago, IL, USA) and involved frequency distribution, association tests and analysis of variance. Since the data did not present normal distribution, measured by the Shapiro-Wilk test, non-parametric tests were used for further analysis. The association between the type of protocol and assessment of anxiety by the surgeon and researcher was determined using the Chi-square test. Agreement between the surgeon and researcher was determined using the Kappa concordance index. Data on cardiovascular parameters (BP and HR) were submitted to Friedman test in partitions subdivided in time and Wilcoxon test for pairwise comparisons, adjusted for multiple contrasts (P < 0.0166). The Wilcoxon test was used to compare measures between the two protocols. Level of significance was set at P ≤ 0.05. In order to determine the clinical significance of results, effect size analyses were carried out comparing the results with the use of Valerian and the placebo. This test - proposed in 1992 - quantifies the effect of the difference between two groups in an association between the variation in mean and standard deviation values.[14] The calculation of the effect was performed (using the formula  , adjusted for repeated measures, d ×
, adjusted for repeated measures, d ×  ; d = effect size, mA = mean value observed for the experimental group, mB = mean value observed for the control group, σ = standard deviation) with the subtraction of the Valerian results from the placebo results (placebo mean – Valerian mean). Thus, results with a negative sign indicate that the values obtained with the use of the Valerian were higher than those obtained with placebo.
; d = effect size, mA = mean value observed for the experimental group, mB = mean value observed for the control group, σ = standard deviation) with the subtraction of the Valerian results from the placebo results (placebo mean – Valerian mean). Thus, results with a negative sign indicate that the values obtained with the use of the Valerian were higher than those obtained with placebo.
Results
The research was conducted between March and August 2003. A total of 20 patients who started the clinical trial participated of all post-operative stages. All patients presented good health condition during and after all the research. A flow diagram of the progress of the trial according to CONSORT statement is shown in Figure 1. Patients were 17-30 years old (mean age = 20.9), the predetermined codes for the treatments were revealed, wherefore identifying the medication employed in each surgical procedure (Medication 1 = placebo; Medication 2 = V. officinalis L.).
Figure 1.
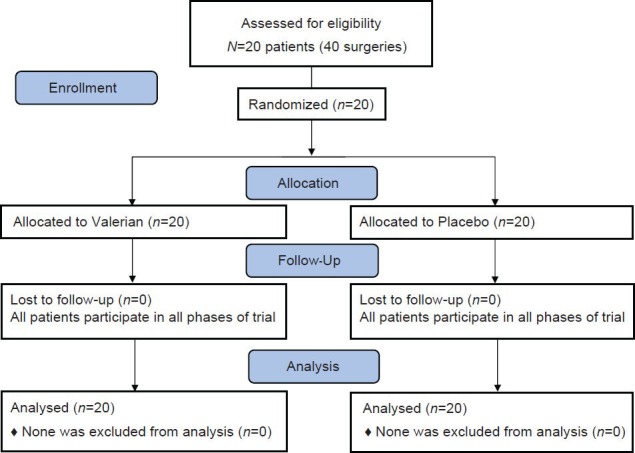
Flow diagram according to CONSORT statement
The assessment of the degree of anxiety of the volunteers using the DAS revealed that 50% were non-anxious. The patients in the other half of the sample were classified as mildly, moderately or very anxious. Wilcoxon test revealed that there were no statistical differences of physiological parameters between anxious and non-anxious patients (P < 0.05). Since in Phase I the result showed no difference in anxiety and physiological parameters with DAS scale, the observation of researcher in Phase 2 was used to classify anxiety.
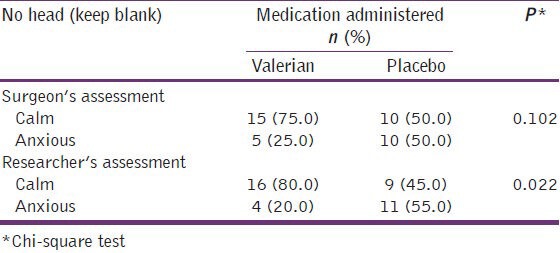
There was agreement between the assessment of anxiety performed by the researcher and surgeon (κ =0.85). In researcher's assessment, the patients medicated with Valerian were calmer and more relaxed (85%) in comparison to those medicated with the placebo (45%) (P = 0.022). A similar result was found in the surgeon's assessment, but the difference did not achieve statistical significance (P = 0.102) [Table 1].
Table 1.
Univariate analysis of association between medication administered and assessment of anxiety performed by researcher and surgeon
When the volunteers were asked as to their preference for one of the surgical procedures at the end of the experiment, 11 (55%) reported a sensation of greater comfort on the procedure in which Valerian was employed. 5 (25%) preferred the procedure in which the placebo was employed and the remaining 4 (20%) had no preference of one procedure over the other.
The self-assessment of patient behavior during the surgeries revealed that 35% in both groups considered themselves to be calm or relaxed, 65% of those medicated with Valerian and 60% of those medicated with the placebo considered themselves mildly anxious and 5% of the patients in the placebo group reported feeling very anxious and afraid during the surgical procedures.
Regarding the occurrence of side effects, 45% (n = 9) of the patients medicated with Valerian reported sleepiness and 35% (n = 7) reported muscle relaxation. The same occurred in 35% (n = 7) and 20% (n = 4) of the patients medicated with the placebo, respectively with no statistical significant difference between medications (P > 0.05). With regard to the occurrence of anterograde amnesia, 85% of the patients recalled all steps of the surgical procedure, 10% remembered the majority of events and 5% remembered very little of the procedures, regardless of the medication administered.
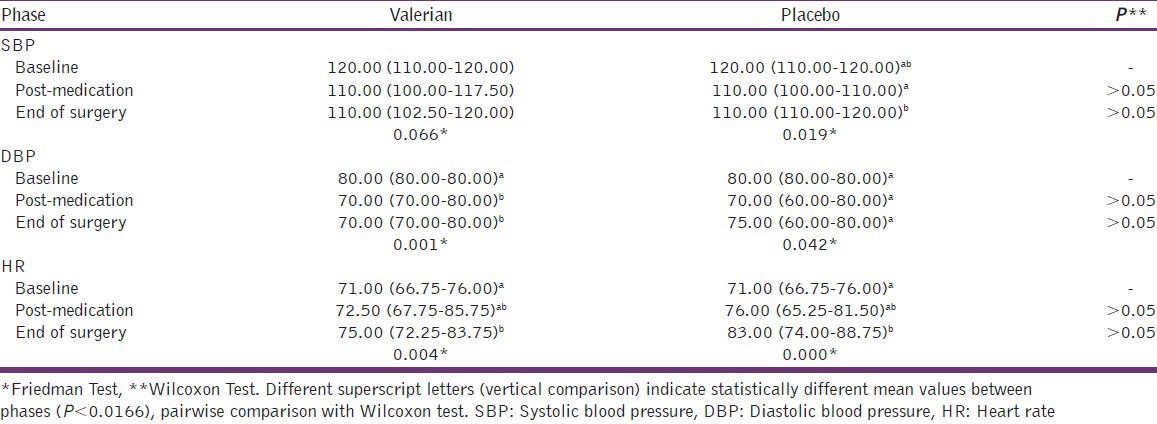
The mean values for SBP, DBP and HR [Table 2] remained within the range of biological normality throughout the entire study. No statistically significant differences were found in patients medicated with Valerian for SBP at different evaluation times (P = 0.066) whereas for placebo (P = 0.019) a statistically difference was found measured by Friedman test. The pairwise comparison using Wilcoxon test showed that there was a tendency of SBP increase between post-medication and the end of surgery in patients medicated with placebo [Table 2]. Concerning DBP for both patients medicated with Valerian (P = 0.001) and placebo (P = 0.042) there was a statistically significant differences at different evaluation times. However, this difference was detected only for Valerian after pairwise comparison. A reduction of DBP was detected after post-medication and the end of surgery for patients using Valerian [Table 2]. The assessment of HR at different evaluation times revealed an increase in this parameter for both patients medicated with Valerian and placebo [Table 2].
Table 2.
Median (centile 25th and centile 75th) values for SBP, DBP and HR at different evaluation times according to medication administered
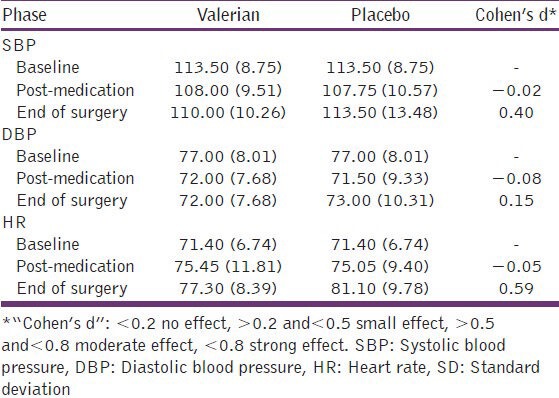
Cohen's effect size test was applied to determine whether there were differences in the physiological parameters (SBP, DBP and HR) in the different evaluation times between the two medications. Table 3 displays the results of this analysis.
Table 3.
Mean (SD) values for SBP, DBP and HR at different evaluation times according to medication administered and Cohen's d* effect
Discussion
Bilateral extraction of impacted lower third molars is one of the best experimental models for the assessment of the efficacy of certain drugs, as it allows the patient to serve as his/her own control, which facilitates the design of a double-blind crossover study. As a more invasive procedure, this type of surgery often generates a greater degree of patient anxiety. Lago-Méndez et al.[15] observed that patients with high dental anxiety may tend to require longer surgery times and also have poorer postoperative recovery after removal of a lower third molar. In this light, the control of dental anxiety in patients undergoing oral surgery becomes imperative.
Anxiety during dental treatment can be identified through patient behavior and the assessment or recognition of physical signs, such as dilated pupils, paleness, excessive perspiration, hyperventilation and an increase in HR and blood pressure.[16] These signs serve as a parameter for classifying patients as either anxious or calm. Both the researcher and surgeon found that the majority of patients medicated with Valerian were calmer and more relaxed in comparison to those who had received the placebo. However statistic significant difference was observed only for researcher observation. The researcher is graduated in pharmacy and trained in anxiety control through conscious sedation and surgeons only have training in dentistry. Perhaps this explains the difference. Gonçalves and França[12] found a similar result, reporting a significant reduction in anxiety among individuals submitted to minor oral surgery using a medication containing a blend of natural substances, including V. officinalis (50 mg). However, the comparison of the data with those of the present study is limited by methodological differences, such as the medication employed and type of surgical procedure.
The dose of V. officinalis L. used in the present study was based on the clinical experience of Kohnen and Oswald,[17] who established a single dose of 100 mg administered 90 min prior to the anxiogenic event. The majority of volunteers (85% of cases) reported remembering all events related to the surgical procedure when treated with V. officinalis L., which demonstrates that this phytotherapeutic agent does not have the property of inducing anterograde amnesia under the conditions analyzed in the present study. V. officinalis L. also demonstrated a good degree of tolerability, as there were no complaints of dizziness, gastrointestinal problems, signs of allergy or the paradoxical effect.
Some drugs referred to as sedatives may also exhibit antispasmodic and hypertensive action.[18] In the present study, the mean BP, HR and oxygen saturation values remained within the range of biological normality throughout the entire study, thereby demonstrating the clinical safety of V. officinalis L., as previously described by Houghton,[8] Kennedy et al.[9] and Wheatley.[10] As there were no statistically significant differences between treatments (Valerian or placebo) using the traditional null hypothesis test, Cohen's effect size test was carried out in order to understand the clinical significance of the results and to determine whether there were differences in the physiological parameters (SBP, DBP and HR) in the different evaluation times between the two medications. At the end of surgery, Valerian presented a better effect than placebo, albeit small (d = 0.35, on the reduction in SBP. Concerning HR the difference between groups was moderate (d = 0.59), suggesting that Valerian offers greater efficacy in the maintenance of HR following surgery [Table 3]. Discussion of physiological parameters results with literature is limited once there are no other studies with this methodology.
Regarding side-effects, the patients described sleepiness and muscle relaxation with both protocols. Valepotriates also exhibit antispasmodic activity, likely by influencing the input of the calcium ion or modifying its binding in the muscle.[19] This effect may be beneficial, as, according to Smyth,[20] muscle tension is one of the physical symptoms of anxiety and can be reduced or minimized with the use of Valerian. Sleepiness was observed in both the patients medicated with Valerian and those who received the placebo. It is therefore suggested that this effect may be attributed to the fatigue caused by the surgeries.
A review of the literature reveals the insufficient amount of information on the quality, safety and efficacy of herbal plants for use in dentistry.[21] As this appears to be one of the first studies to assess the anxiolytic activity of V. officinalis L. in surgical dental procedures, it is hoped that this investigation can serve as a starting point for future studies involving the use of V. officinalis L. and other phytotherapeutic agents in different fields of dentistry.
The article presents some limitations. Sample size calculation was not performed, both anxious and non-anxious patients (determined by DAS scale) at the first appointment were included in the research even though no statistical difference was found between them. As the DAS scale was not a good parameter to assess anxiety of patients the anxious level was assessed by physiological parameters. Evaluation of other more direct indicators of anxious such as stress hormone should provide better understanding of anxiety and including only anxious patients could show a better result of phytotherapy. This study served as a preliminary trial for the future studies of V. officinalis L. in various fields of dentistry. It is believed, however, that Valerian showed anxiolytic activity in the volunteers and, perhaps, may constitute an important pharmacological alternative for the management of anxiety during the dental treatment. With new research showing good results as well, in the future it can represent an alternative to benzodiazepine.
Conclusion
Considering the limitations of the present study, V. officinalis L. administered in a pre-operative dose of 100 mg had a greater anti-anxiety effect than the placebo when used for conscious sedation in adult patients submitted to the extraction of impacted lower third molars.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Freeman R, Clarke HM, Humphris GM. Conversion tables for the Corah and modified dental anxiety scales. Community Dent Health. 2007;24:49–54. [PubMed] [Google Scholar]
- 2.Donaldson M, Gizzarelli G, Chanpong B. Oral sedation: A primer on anxiolysis for the adult patient. Anesth Prog. 2007;54:118–28. doi: 10.2344/0003-3006(2007)54[118:OSAPOA]2.0.CO;2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Göktay O, Satilmiş T, Garip H, Gönül O, Göker K. A comparison of the effects of midazolam/fentanyl and midazolam/tramadol for conscious intravenous sedation during third molar extraction. J Oral Maxillofac Surg. 2011;69:1594–9. doi: 10.1016/j.joms.2010.09.005. [DOI] [PubMed] [Google Scholar]
- 4.de Abreu MH, Acúrcio Fde A, Resende VL. The use of psychotropics by dental patients in Minas Gerais, Brazil. Rev Panam Salud Publica. 2000;7:17–23. doi: 10.1590/s1020-49892000000100003. [DOI] [PubMed] [Google Scholar]
- 5.Gan TJ. Pharmacokinetic and pharmacodynamic characteristics of medications used for moderate sedation. Clin Pharmacokinet. 2006;45:855–69. doi: 10.2165/00003088-200645090-00001. [DOI] [PubMed] [Google Scholar]
- 6.Rice A, Liddell A. Determinants of positive and negative attitudes toward dentistry. J Can Dent Assoc. 1998;64:213–8. [PubMed] [Google Scholar]
- 7.Malamed SF. St. Louis: Mosby; 1995. Sedation: A Guide to Patient Management. [Google Scholar]
- 8.Houghton PJ. The scientific basis for the reputed activity of Valerian. J Pharm Pharmacol. 1999;51:505–12. doi: 10.1211/0022357991772772. [DOI] [PubMed] [Google Scholar]
- 9.Kennedy DO, Little W, Haskell CF, Scholey AB. Anxiolytic effects of a combination of Melissa officinalis and Valeriana officinalis during laboratory induced stress. Phytother Res. 2006;20:96–102. doi: 10.1002/ptr.1787. [DOI] [PubMed] [Google Scholar]
- 10.Wheatley D. Medicinal plants for insomnia: A review of their pharmacology, efficacy and tolerability. J Psychopharmacol. 2005;19:414–21. doi: 10.1177/0269881105053309. [DOI] [PubMed] [Google Scholar]
- 11.Cropley M, Cave Z, Ellis J, Middleton RW. Effect of kava and valerian on human physiological and psychological responses to mental stress assessed under laboratory conditions. Phytother Res. 2002;16:23–7. doi: 10.1002/ptr.1002. [DOI] [PubMed] [Google Scholar]
- 12.Gonçalves EC, França FM. Evaluation of the use of homeophatic anxiolytic in dental surgical procedures as alternative drugs to the benzodiazepinics. Rev Gaúcha Odontol. 2007;55:175–80. [Google Scholar]
- 13.Pell GJ, Gregory BT. Impacted mandibular third molars: Classification and modified techniques for removal. Dent Dig. 1933;39:330–8. [Google Scholar]
- 14.Cohen J. A power primer. Psychol Bull. 1992;112:155–9. doi: 10.1037//0033-2909.112.1.155. [DOI] [PubMed] [Google Scholar]
- 15.Lago-Méndez L, Diniz-Freitas M, Senra-Rivera C, Seoane-Pesqueira G, Gándara-Rey JM, García-García A. Postoperative recovery after removal of a lower third molar: Role of trait and dental anxiety. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:855–60. doi: 10.1016/j.tripleo.2009.07.021. [DOI] [PubMed] [Google Scholar]
- 16.Eitner S, Wichmann M, Paulsen A, Holst S. Dental anxiety - An epidemiological study on its clinical correlation and effects on oral health. J Oral Rehabil. 2006;33:588–93. doi: 10.1111/j.1365-2842.2005.01589.x. [DOI] [PubMed] [Google Scholar]
- 17.Kohnen R, Oswald WD. The effects of valerian, propranolol, and their combination on activation, performance, and mood of healthy volunteers under social stress conditions. Pharmacopsychiatry. 1988;21:447–8. doi: 10.1055/s-2007-1017047. [DOI] [PubMed] [Google Scholar]
- 18.Roelofse JA, van der Bijl P. Cardiac dysrhythmias associated with intravenous lorazepam, diazepam, and midazolam during oral surgery. J Oral Maxillofac Surg. 1994;52:247–50. doi: 10.1016/0278-2391(94)90293-3. [DOI] [PubMed] [Google Scholar]
- 19.Wagner H, Jurcic K. On the spasmolytic activity of valeriana extracts (author's transl) Planta Med. 1979;37:84–6. doi: 10.1055/s-0028-1097303. [DOI] [PubMed] [Google Scholar]
- 20.Smyth JS. Some problems of dental treatment. Part 1. Patient anxiety: Some correlates and sex differences. Aust Dent J. 1993;38:354–9. doi: 10.1111/j.1834-7819.1993.tb05516.x. [DOI] [PubMed] [Google Scholar]
- 21.Groppo FC, Bergamaschi Cde C, Cogo K, Franz-Montan M, Motta RH, de Andrade ED. Use of phytotherapy in dentistry. Phytother Res. 2008;22:993–8. doi: 10.1002/ptr.2471. [DOI] [PubMed] [Google Scholar]