

Abstract
Objectives
The aim of this study was to evaluate the detection of enamel-dentin occlusal caries using photostimulable phosphor plates.
Material and Methods
The ability to detect enamel-dentin occlusal caries in 607 premolars and molars from 47 patients between 10 and 18 years old, referred to the School of Dentistry of the Federal University of Bahia, Brazil, was evaluated based on clinical and radiographic examinations, using the criteria proposed in a previous study. A total of 156 bitewing digital images were obtained using Digora® (Soredex Medical Systems, Helsinki, Finland) phosphor plates. The plates were scanned and the images were captured and displayed on a computer screen. Image evaluation was done using Digora® for Windows 2.1 software, Soredex®. The radiologists were allowed to use enhancement tools to obtain better visibility during scoring of the teeth based on the radiographic criteria proposed in a previous study. Descriptive analysis and chi-squared proportion tests were done at 5% significance level.
Results
The results of clinical examination showed a higher prevalence of teeth with a straight dark line or demineralization of the occlusal fissure (score 1) and a lower prevalence of sealed teeth (score 5). In the bitewing digital images, 47 teeth presented visible radiolucency, circumscribed, in dentin under occlusal enamel (enamel-dentin caries lesions).
Conclusions
Correlating the clinical and radiographic findings, it was found that in the majority of teeth diagnosed by radiographic images as having enamel-dentin caries, no caries could be detected by clinical examination.
Keywords: Dental caries, Bitewing radiographs, Digital radiography, Photostimulable phosphor
INTRODUCTION
The detection of caries lesions is still a matter of investigation in Dentistry. Epidemiologic studies have shown that non-cavitated lesions are more prevalent than cavitated lesions3,8. Extensive lesions can develop in dentin beneath an apparently sound enamel crown, or superficial occlusal lesion, which may ultimately undermine the enamel7.
Enamel-dentin caries, also known as hidden caries, is a phenomenon that leads to formation of highly mineralized, strengthened enamel surfaces, under which the loss of mineral may progress gradually and the carious lesion might extend into dentin without a clinically visible crack at the enamel surface. There is no consensus on the cause of enamel-dentin caries. It has been suggested that, despite the indubitable benefits, the high remineralization capacity of fluoride might mask dentin caries, mainly for those who have lifelong exposure to water fluoridation. An alternative hypothesis is that the phenomenon occurs as a result of interactions between enamel and dentin7,13,14.
When a small, localized, developing enamel lesion crosses the dentinoenamel junction into the dentin, relatively high concentrations of dentin dissolution products could be sufficient to prevent or retard dissolution of enamel but insufficient to confer the same degree of protection on the more soluble dentin. This would leave the dentin lesion to progress undetected beneath an apparently intact or superficially demineralized enamel crown. The potential also exists for remineralization of an occlusal enamel lesion to occur while the dentin continues to dissolve, which could mask the enamel demineralization and further increase the difficulty of detecting the enamel-dentin caries7.
It is not known whether hidden caries exists as a distinct entity and it has been asserted that to use the term simply implies an insufficient clinical examination. However, concern has been expressed at the difficult of detecting occlusal caries lesions under apparently sound enamel7,17,18. Thus, the detection of enamel-dentin caries, or hidden caries, is difficult, and the association of different diagnosis methods is fundamental to determine the presence of these lesions. The radiographic exam, used as a complement of the clinical visual exam, is a disposable tool for dental researchers and professionals4,5,20.
Digital image systems demonstrate diagnostic accuracy comparable to conventional radiography4-6,11,15,22. Digital systems present a significant reduction in exposure to radiation of 50-90%. Digital receptors are more sensitive to radiation than film, require less exposure to radiation, and chemical processing are not needed5,21.
Digora® (Soredex Medical Systems, Helsinki, Finland) is one of the several digital systems that use an optical plate, composed of photofluorescent particles that are sensitive to x-rays, forming a latent image. The optic plate is scanned on a Digora® optic scanner, and the final image is displayed on a computer screen. The final image can be enhanced using the system's software enhancement tools10,21.
The present study evaluated the detection of enamel-dentin occlusal caries using photostimulable phosphor plates. The specific aims were: to evaluate the frequency of enamel-dentin occlusal caries in relation to gender and age; to compare the occurrence of enamel-dentin occlusal caries in different tooth groups; to compare detection of enamel-dentin occlusal caries based on digital images with detection based on clinical findings using the criteria proposed by Weerheijm, Gruythuysen and Van Amerongen19 (1992).
MATERIAL AND METHODS
In agreement with the Departments of Cariology, Pediatric Dentistry, and Dentistry II of the School of Dentistry of the Federal University of Bahia (FOUFBA), new patients aged between 10 and 18 years, which is the age range with the highest prevalence of enamel-dentin caries18, were evaluated clinically. The purpose of the research was explained and patient informed assent forms for minors and patient informed consent forms for adults and parents/guardians were signed. This study was approved by the FOUFBA's Research Ethics Committee (Protocol number 0006.0.368.000-07).
Before the examination sessions, verbal and practical instructions and calibration tests were performed. For the calibration tests, the occlusal surfaces in 10 patients (maxillary and mandibular arches) were evaluated based on the criteria proposed by Weerheijm, Gruythuysen and Van Amerongen19 (1992) (Figure 1), by two researchers, under the same conditions, and with inter-examiner agreement of 0.98 and kappa value of 0.92.
Figure 1.
Weerheijm, Gruythuysen and Van Amerongen19 (1992) criteria for clinical examination
| 0 | Sound (absence of demineralization or color change) |
| 1 | Presence of a straight dark line or demineralization on the occlusal fissure |
| 2 | Presence of a wide dark line, or a straight and dark line, combined with fissure demineralization |
| 3 | Dentine lesion |
| 4 | Restored |
| 5 | Sealed |
After supervised toothbrushing, the teenagers were examined in supine position, under a standard dental operating light, and with compressed air to dry the surfaces to be evaluated. For the visual examination, a plain mouth mirror was necessary to hold back the soft tissue and permit better visualization of the area. The visual examination was completed using a no. 5 probe to remove any residual dental plaque by applying soft pressure. The occlusal surfaces of permanent premolars and molars were clinically evaluated, based on the criteria of Weerheijm, Gruythuysen and Van Amerongen19 (1992). Scores of 1 and 2 represent lesions with depth limited to the enamel and no signs of caries in dentin. The occlusal surfaces were divided into the following groups: sound, a combination of criteria 0, 1, 2 and 5; completely sound, exclusively criteria 0; and presence of disease, criteria 3 and 4.
The bitewing radiographic exam was part of the treatment protocol in this study for patients without dentin lesions; for teeth with dentin lesion with possible pulp lesion, periapical radiographs were used as a complementary diagnostic method.
Using the Digora® digital system, phosphor plates and radiographic bitewing Han-Shin film holders (JON, São Paulo, SP, Brazil), all patients clinically evaluated were radiographed using a Timex 70 C machine (Gnatus, Ribeirão Preto, SP, Brazil), with fixed parameters: 70 kVp, 3 mA, 0.3 seconds. Bitewing views of premolar and molar areas were obtained.
The images were evaluated by two experienced radiologists, at different times, in a dimly lit room, with a cardboard simulating a black mask attached to the monitor, so that the image seen by the observer corresponded to the real image size, and shielding it from the light emitted by the screen. Image evaluation was done using Digora® for Windows 2.1 software, Soredex®. The radiologists were allowed to use zoom and other enhancement tools for better visualization during the scoring of the teeth based on the aforementioned criteria19 (Figure 2). Figure 3 shows the radiographic aspects of the occlusal surfaces according to the criteria adopted in the study19. In case of disagreements, both observers evaluated the images again until they came to a consensus.
Figure 2.
Weerheijm, Gruythuysen and Van Amerongen19 (1992) criteria for radiographic examinations
| 0 | Absence of any visible radiolucency in dentine under occlusal enamel |
| 3 | Presence of visible radiolucency, circumscribed, in dentine under occlusal enamel-enamel-dentine caries lesions (only high quality pattern radiographic images) |
| 4 | Radiopaque image suggesting restoration |
| 6 | Impossible to judge and density measurement and histogram tools may be applied |
Figure 3.
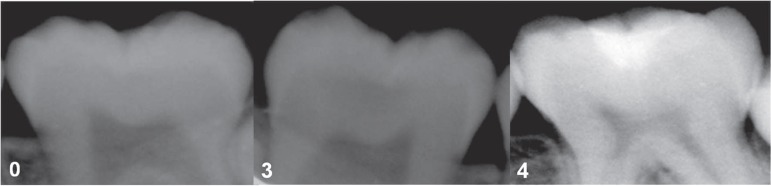
Radiographic aspects of the occlusal surfaces according to Weerheijm, Gruythuysen and Van Amerongen19 (1992) criteria
Technical files were created based on the criteria of Weerheijm, Gruythuysen and Van Amerongen19 (1992) to archive the data from the clinical and radiographic examinations of each patient. The data were correlated. Descriptive analysis and chi-squared proportion tests were done; a p value of ≤0.05 was considered significant.
At a later moment, the teeth with presence of visible radiolucency, circumscribed, in dentin under occlusal enamel (enamel-dentin caries lesions) were opened and the accuracy of the method was evaluated.
RESULTS
Six hundred and seven teeth of 47 patients were evaluated (17 males and 30 females). The mean age was 12.78±2.50 years. Of the 607 clinically evaluated teeth, 121 were second molars, 179 were first molars, 145 were second premolars and 162 were first premolars (Figure 4). The teeth were distributed based on the criteria adopted in the study19 (Figure 5).
Figure 4.

Distribution of evaluated teeth based on tooth groups (1st premolar, 2nd premolar, 1st molar and 2nd molar)
Figure 5.

Distribution of Weerheijm, Gruythuysen and Van Amerongen19 (1992) clinical criteria on the evaluated teeth
Teeth with dark stained straight lines or demineralization on the occlusal fissure (score 1) were the most prevalent (229-37.73%), followed by sound teeth (scored as 0, 224-36.90%). The least prevalent pattern was score 5 at 2.14% of the total sample.
The radiographic evaluation was done by two experienced dental radiologists, who obtained a high inter-examiner reproducibility value (kappa value 0.89). The results for the radiographic evaluation are shown in Figure 6. The distribution of the 47 teeth with enamel-dentin caries based on Weerheijm, Gruythuysen and Van Amerongen19 (1992) clinical criteria is shown on Table 1.
Figure 6.

Distribution of Weerheijm, Gruythuysen and Van Amerongen19 (1992) radiographic criteria on the evaluated teeth
Table 1.
Distribution of teeth with enamel-dentin caries based on Weerheijm, Gruythuysen and Van Amerongen19 (1992) clinical criteria
| Criteria | Enamel-dentine caries lesions (%) |
|---|---|
| 0 | 7 (14.89) |
| 1 | 10 (21.28) |
| 2 | 24 (51.06) |
| 3 | 5 (10.64) |
| 4 | 0 |
| 5 | 1 (2.13) |
Of the 47 patients examined, 24 did not present enamel-dentin occlusal caries, and 23 had enamel-dentin occlusal caries. The distribution of patients by gender with and without enamel-dentin caries is shown on Table 2. The chi-squared test was used to evaluate the difference between the prevalence of enamel-dentin caries lesions for females and males, and there was no significant difference between the two groups (p=0.9672) (Table 2).
Table 2.
Distribution of patients by gender with and without enamel-dentin caries (p=0.9672)
| Enamel-dentine caries | Gender | Total (%) | |
|---|---|---|---|
| Male (%) | Female (%) | ||
| Absence | 9 (37.50) | 15 (62.50) | 24 (51.06) |
| Presence | 8 (34.78) | 15 (65.21) | 23 (48.94) |
| Total | 17 (36.17) | 30 (63.83) | 47 (100.00) |
The presence or absence of enamel-dentin caries was also evaluated for different age groups (10-12 years, 13-15 years and 16-18 years). There was no statistically significant difference (p=0.87) for the prevalence of enamel-dentin lesions among these age groups.
When evaluating different dental groups for the presence of enamel-dentin caries, 14.29% (17 teeth) of the second molars presented enamel-dentin caries, 15.12% (26 teeth) of the first molars, 1.47% (2 teeth) of the second premolars and 1.51% (2 teeth) of the first premolars. This shows that enamel-dentin caries was more frequently found in molars (Figure 7).
Figure 7.

Distribution of Weerheijm, Gruythuysen and Van Amerongen19 (1992) radiographic criteria on the different tooth groups (M= molar; PM= premolar)
Table 3 shows the frequency of different clinical aspects (criteria 0, 1, 2, 3, 4 and 5) in teeth with enamel-dentin caries based on tooth group (second molars, first molars, second premolars or first premolars). First molars and second molars showed a statistically significant difference among the clinical diagnosis criteria, with a predominance of criterion 2 (a wide dark stained line or demineralization in fissure) in a larger number of teeth (p=0.05).
Table 3.
Frequency of different clinical aspects of teeth with enamel-dentin caries related to tooth group (p=0.5)
| Clinical criterion | Enamel-dentine caries | Total (%) | |||
|---|---|---|---|---|---|
| 2nd M (%) | 1st M (%) | 2nd PM (%) | 1st PM (%) | ||
| 0 | 5 (29.41) | 1 (3.85) | 0 | 1 (50.00) | 7 (14.89) |
| 1 | 1 (5.88) | 7 (26.92) | 1 (50.00) | 1 (50.00) | 10 (21.28) |
| 2 | 8 (47.06) | 16 (61.54) | 0 | 0 | 24 (51.06) |
| 3 | 3 (17.65) | 1 (3.85) | 1 (50.00) | 0 | 5 (10.64) |
| 4 | 0 | 0 | 0 | 0 | 0 |
| 5 | 0 | 1 (3.85) | 0 | 0 | 1 (2.13) |
| Total | 17 (36.17) | 26 (55.32) | 2 (4.25) | 2 (4.25) | 47 (100) |
(M= molar; PM= premolar)
When evaluating the distribution of enamel-dentin lesions on maxillary and mandibular teeth, it was found that maxillary premolars and molars were less affected by enamel-dentin caries (16 teeth) than the mandibular premolars and molars (31 teeth), although that difference was not statistically significant (p=0.075) (Table 4).
Table 4.
Distribution of enamel-dentin caries on maxillary and mandibular premolars and molars (p=0.075)
| Enamel-dentine caries | Arch | Total (%) | |
|---|---|---|---|
| Upper (%) | Lower (%) | ||
| Absence | 270 (52.73) | 242 (47.27) | 512 (91.59) |
| Presence | 15 (31.91) | 32 (68.09) | 47 (8.41) |
| Total | 285 (50.98) | 274 (49.02) | 559 (100.00) |
Of the 47 teeth diagnosed by radiographic examination as having enamel-dentin caries, 9 were opened for treatment and all of them presented dentin caries lesions. These teeth were restored with composite resin and one of them required endodontic treatment due to pulp infection caused by an extensive caries lesion. The remaining teeth diagnosed as having enamel-dentin caries were treated with non-invasive procedures (fluoride therapy and/or sealant placement) and monitoring, based on a multidisciplinary decision.
The teeth classified according to the criteria of Weerheijm, Gruythuysen and Van Amerongen19 (1992) as score 6 on radiographic images (Figure 3) had the clinical option of monitoring the lesion.
DISCUSSION
The total number of teeth evaluated by radiographic examination (559) did not correspond to the total number of teeth evaluated clinically (607), so there was a difference of 48 teeth, due to incomplete imaging of some teeth in the radiographs.
Based on tooth eruption chronology, 1st molars erupt earlier than 2nd molars and then 1st and 2nd premolars. As their contact with the oral cavity is longer than the other posterior teeth, they are more susceptible to dental caries and cavitated lesions, and are also frequently restored2. That can explain the occurrence of more sealed surfaces on 1st molars (11 1st molars of 13 sealed teeth) and the occurrence of restorations in this same group of teeth (27 1st molars of 47 restored teeth); premolars presented completely sound occlusal surfaces (score 0) in a high number of teeth compared with molars (155 premolars and 69 molars).
In the present study, 32 teeth presented cavities during clinical examination, and 47 teeth presented enamel-dentin occlusal caries, demonstrating a higher occurrence of non-cavitated lesions than cavitated lesions.
The dentin lesions detected on the radiographs with no clinical signs of disease, did not present a different pattern regarding age and gender (Table 2), which is agreement with the findings of Weerheijm, Gruythuysen and Van Amerongen19 (1992).
In the patients aged between 10 and 12 years, there was a higher prevalence of enamel-dentin caries (26 teeth), when compared to those aged between 13 and 15 years (9 teeth) and between 16 and 18 years (12 teeth), though this was not statistically significant. This result may be due to the fact that in the older teenagers, most of the lesions were cavitated or restored. In those aged between 10 and 12 years, 13 and 15 years and 16 and 18 years, 6, 8 and 16 teeth were found to have dentin caries and 9, 17 and 21 teeth were restored, respectively.
When considering the prevalence of enamel-dentin caries in maxillary and mandibular molars, Weerheijm, Gruythuysen and Van Amerongen19 (1992) affirmed that there is no significant difference between maxillary and mandibular arches. Our study found a higher occurrence of enamel-dentin caries in mandibular molars than in maxillary molars, but this difference was not statistically significant (Table 4).
Comparing the presence and distribution of enamel-dentin caries lesions in the various tooth types, the first erupted posterior teeth in the oral cavity had the highest number of enamel-dentin lesions on dentin. The mandibular first molars were affected in 15 of the 47 cases of enamel-dentin caries, maxillary first molars in 11 cases, second mandibular molars in 13 cases and second maxillary molars in only 4 cases. Of all teeth with enamel-dentin caries detected, only four premolars were affected.
For the second molars, even with the same caries lesion, the clinical condition led to a difficult diagnosis, with criterion 0 (Figure 1) scored incorrectly for more units with enamel-dentin caries (Table 3).
Routine clinical examinations without complementary radiographic examinations do not detect the occurrence of caries lesions in some teeth. In many examinations, radiographic images are carried out only when there is a suspicion of a caries lesion on proximal surfaces9,11. This situation is more complex when considering epidemiologic studies involving a larger number of individuals. In these cases, no radiographic images are taken and caries lesions are under-reported3.
According to the guidelines of the American Dental Association1 (2006), radiographic diagnosis should only be used after clinical examination, considering the dental and general health needs of the patient. Because each patient is different, radiographic examination should be individualized1. In the present study, we observed that enamel-dentin caries could not be detected in clinical examination: 8.41% of the teeth clinically diagnosed as sound presented dentin caries (Figure 7). Thus, bitewing radiographic images should be considered part of the initial routine dental examination in children. Newman, et al.9 (2009) support the recommendations of pediatric dentistry worldwide that bitewing radiography be considered part of the initial routine dental examination of children because the prevalence of hidden occlusal caries detectable only radiographically is approximately 12%.
Civera, et al.5 (2007) also concluded that the use of radiographic techniques, conventional or digital, increases the number of caries lesions diagnosed compared to clinical examination alone; 3.23 times more caries lesions were diagnosed using digital images and 2.88 more lesions were diagnosed using conventional radiography, when compared to clinical examination.
Digital radiography is a reality, and its reduced dose of radiation provides real benefits to the patient. Besides having similar accuracy for the detection of caries lesions as conventional radiography4,6,11,15, it also has the advantage of not requiring film and chemical processing21. More studies on the application of density measurement tools and histograms are necessary.
Early diagnosis of enamel-dentin caries provides the opportunity for non-invasive treatment through remineralization of small lesions, resulting in inactive lesions and preservation of the dental structure, function and esthetics12,16. Non-invasive treatments were chosen (fluoride therapy and/or sealant placement), by consensual multidisciplinary decision, for 38 of the 47 teeth diagnosed as having enamel-dentin caries.
CONCLUSIONS
It is important to note that radiographic examination, even using digital systems, presents considerable limitations; for example, one cannot determine if the lesion is active or not, or the presence or absence of cavities. Research on detection of enamel-dentin caries is still ongoing and this study permits the implementation of future studies in this area. It is important to have a precise diagnostic method, with an established protocol for bitewing radiographic images as a reference for all patients that present clinically sound dental units.
ACKNOWLEDGMENTS
We are grateful to Fapesb (Edital Temático 2004) and CNPq for their contributions for this study.
REFERENCES
- 1.American Dental Association Council on Scientific Affairs The use of dental radiographs: update and recommendations. J Am Dent Assoc. 2006;137:1304–1312. doi: 10.14219/jada.archive.2006.0393. [DOI] [PubMed] [Google Scholar]
- 2.Alvarez JO, Navia JM. Nutritional status, tooth eruption, and dental caries: a review. Am J Clin Nutr. 1989;49:417–426. doi: 10.1093/ajcn/49.3.417. [DOI] [PubMed] [Google Scholar]
- 3.Assaf AV, Meneghim MC, Zanin L, Mialhe FL, Pereira AC, Ambrosano GMB. Assessment of different methods for diagnosing dental caries in epidemiological surveys. Commun Dent Oral Epidemiol. 2004;32:418–425. doi: 10.1111/j.1600-0528.2004.00180.x. [DOI] [PubMed] [Google Scholar]
- 4.Castro VM, Katz JO, Hardman PK, Glaros AG, Spencer P. In vitro comparison of conventional film and direct digital imaging in the detection of approximal caries. Dentomaxillofac Radiol. 2007;36:138–142. doi: 10.1259/dmfr/15558921. [DOI] [PubMed] [Google Scholar]
- 5.Civera VG, Silla JMA, Company JMM, Navarro LF. Clinical and radiographic diagnosis of approximal and occlusal dental caries in a low risk population. Med Oral Patol Oral Cir Bucal. 2007;12:E252–E257. [PubMed] [Google Scholar]
- 6.Ferreira RI, Haiter-Neto F, Tabchoury CPM, Paiva GAN, Bóscolo FN. Assessment of enamel demineralization using conventional, digital, and digitized radiography. Braz Oral Res. 2006;20:114–119. doi: 10.1590/s1806-83242006000200005. [DOI] [PubMed] [Google Scholar]
- 7.Lynch RJM, Ten Cate JM. The effects of adjacent dentine blocks on the demineralization and remineralization of enamel in vitro. Caries Res. 2006;40:38–42. doi: 10.1159/000088904. [DOI] [PubMed] [Google Scholar]
- 8.Meneghim MC, Assaf AV, Zanin L, Kozlowski FC, Pereira AC, Ambrosano GM. Comparison of diagnostic methods for dental caries. J Dent Child (Chic) 2003;70:115–119. [PubMed] [Google Scholar]
- 9.Newman B, Seow WK, Kazoullis S, Ford D, Holcombe T. Clinical detection of caries in the primary dentition with and without bitewing radiography. Aust Dent J. 2009;54:23–30. doi: 10.1111/j.1834-7819.2008.01084.x. [DOI] [PubMed] [Google Scholar]
- 10.Parks ET, Williamson GF. Digital radiography: an overview. J Contemp Dent Pract. 2002;3:23–39. [PubMed] [Google Scholar]
- 11.Peker I, Toraman Alkurt M, Altunkaynak B. Film tomography compared with film and digital bitewing radiography for proximal caries detection. Dentomaxillofac Radiol. 2007;36:495–499. doi: 10.1259/dmfr/13319800. [DOI] [PubMed] [Google Scholar]
- 12.Pretty IA. Caries detection and diagnosis: novel technologies. J Dent. 2006;34:727–739. doi: 10.1016/j.jdent.2006.06.001. [DOI] [PubMed] [Google Scholar]
- 13.Ricketts DNJ, Ekstrand KR, Martignon S, Ellwood R, Alatsaris M, Nugent Z. Accuracy and reproducibility of conventional radiographic assessment and subtraction radiography in detecting demineralization in occlusal surfaces. Caries Res. 2007;41:121–128. doi: 10.1159/000098045. [DOI] [PubMed] [Google Scholar]
- 14.Souza-Zaroni WC, Ciccone JC, Souza-Gabriel AE, Ramos RP, Corona SAM, Palma-Dibb RG. Validity and reproducibility of different combinations of methods for occlusal caries detection: an in vitro comparison. Caries Res. 2006;40:194–201. doi: 10.1159/000092225. [DOI] [PubMed] [Google Scholar]
- 15.Syriopoulos K, Sanderink GCH, Velder XL, Van Der Stelt PF. Radiographic detection of approximal caries: a comparison of dental films and digital imaging systems. Dentomaxillofac Radiol. 2000;29:312–318. doi: 10.1038/sj/dmfr/4600553. [DOI] [PubMed] [Google Scholar]
- 16.Thompson VP, Kaim JM. Nonsurgical treatment of incipient and hidden caries. Dent Clin North Am. 2005;49:905–921. doi: 10.1016/j.cden.2005.05.003. [DOI] [PubMed] [Google Scholar]
- 17.Weerheijm KL. Occlusal "hidden caries". Dent Update. 1997;24:182–184. [PubMed] [Google Scholar]
- 18.Weerheijm KL, Groen HJ, Bast AJ, Kieft JA, Eijkman MA, Van Amerongen WE. Clinically undetected occlusal dentine caries: a radiographic comparison. Caries Res. 1992;26:305–309. doi: 10.1159/000261457. [DOI] [PubMed] [Google Scholar]
- 19.Weerheijm KL, Gruythuysen RJ, Van Amerongen WE. Prevalence of hidden caries. ASDC J Dent Child. 1992;59:408–412. [PubMed] [Google Scholar]
- 20.Wenzel A. Bitewing and digital bitewing radiography for detection of caries lesions. J Dent Res. 2004;83:C72–C75. doi: 10.1177/154405910408301s14. [DOI] [PubMed] [Google Scholar]
- 21.Wenzel A. A review of dentists´ use of digital radiography and caries diagnosis with digital systems. Dentomaxillofac Radiol. 2006;35:307–314. doi: 10.1259/dmfr/64693712. [DOI] [PubMed] [Google Scholar]
- 22.Wenzel A, Haiter-Neto F, Gotfredsen E. Influence of spatial resolution and bit depth on detection of small caries lesions with digital receptors. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:418–422. doi: 10.1016/j.tripleo.2006.05.016. [DOI] [PubMed] [Google Scholar]