

Abstract
We evaluate Spectral OCT (SOCT) with a speckle contrast reduction technique using resonant scanner for assessment of corneal surface changes after excimer laser photorefractive keratectomy (PRK) and we compare healing process between conventional PRK and transepithelial PRK. The measurements were performed before and after the surgery. Obtained results show that SOCT with a resonant scanner speckle contrast reduction is capable of providing information regarding the healing process after PRK. The main difference between the healing processes of PRK and TransPRK, assessed by SOCT, was the time to cover the stroma with epithelium, which was shorter in the TransPRK group.
OCIS codes: (110.4500) Optical coherence tomography, (030.6140) Speckle, (330.1070) Vision - acuity
1. Introduction
Photorefractive keratectomy (PRK) is a laser eye surgery procedure intended to correct refractive error of the human eye reducing dependency on glasses or contact lenses. The technique permanently change the shape of the anterior central cornea using an excimer laser to ablate (remove by vaporization) a small amount of tissue from the corneal stroma at the front of the eye. In conventional PRK, before the ablation of the stroma, the corneal epithelium has to be removed. The original method to remove the epithelium before photorefractive keratectomy (PRK) was manual, mechanical scraping, which was later enhanced by the use of alcohol solution or brush [1, 2]. In 2003, Camellin proposed a new alcohol-assisted technique called laser-assisted sub-epithelial keratectomy (LASEK), which enabled preservation of the epithelium as a flap and reapplying it to the ocular surface after treatment [3]. Another method that uses an epithelial flap, separated with a microkeratome with a blunt oscillating blade, is called epithelial laser in situ keratomileusis (Epi-LASIK) and was introduced almost simultaneously [4]. Another alternative is transepithelial PRK, where epithelial removal is carried out with laser phototherapeutic (PTK) ablation, followed by a laser refractive ablation of the stroma. This technique has been used since the 1990s but due to the prolonged surgery time with old generation lasers, increased pain, and a lack of adjusted nomograms, this technique was not widely used [5–7]. Recently, a new variation of transepithelial PRK, called TransPRK, was introduced by Schwind eye-tech-solutions. In TransPRK, both epithelium and stroma are removed in a single step, in one ablation profile, which takes into account literature data estimating the central epithelial thickness of a normal cornea to be 55 µm and 65 µm at 4 mm from the center [8]. The procedure has several advantages, but the main disadvantage is higher total energy load delivered by the excimer laser; although, its influence on the healing process of the cornea is unclear.
Therefore, the aim of this paper was to reveal differences in the healing process between conventional PRK and transepithelial. For in vivo examination of the healing process of the cornea, we used a non-invasive and non-contact SOCT technique with a novel speckle contrast reduction method, recently proposed by Szkulmowski et al. [9]. In the mentioned paper it has been shown that the technique increases effective image resolution and improves visualization of corneal structures, such as Bowman’s layer and the basal epithelium layer.
2. Materials and methods
2.1. Prototype of Spectral OCT system with resonant scanner
The SOCT system used for the study, see Fig. 1 was based on a standard fiber-optic Michelson interferometer, in which the object arm was modified by the introduction of a resonant scanner (CRS 4kHz, Cambridge Technology) just after beam collimator. This technique was described in detail by Szkulmowski et al. and applied for the real-time reduction of speckle contrast in the imaging of human eyes and skin [9]. In principle, the presented configuration can be applied to any OCT modality.
Fig. 1.
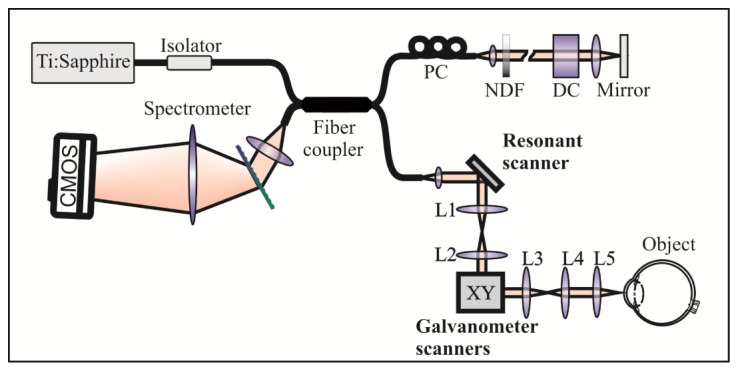
Schematic of the SOCT setup used in this study. Ti:Sapphire – light source; PC – polarization controller; NDF – neutral density filter; DC – dispersion compensator; CMOS – camera; L1-5 – lenses.
The light emitted by a Ti: Sapphire laser (λ0 = 795 nm, Δλ = 150 nm, Femtosecond laser, Austria) provided the measured axial resolution of the instrument 5.7 µm in the air (~4.2 µm in tissue). In the objective arm, the light, after being dithered by the resonant scanner is directed to galvanometric scanners by a non-magnifying telescope (L1-L2). Such a configuration allows an additional sinusoidal trajectory from the resonant scanner to be superimposed on the standard raster scanning pattern introduced by galvanometric scanners, Fig. 2(a) . In our configuration, we acquired SOCT signals when the sampling beam was on the linear slope of the sinusoidal pattern. The scanners are independent of each other; thus, it is possible to configure the trajectory in such a way that, during one period of resonant scanner oscillation Tresonant, the beam travels a much larger distance in the direction perpendicular to the direction of the imaged cross-section than in the lateral direction. In such a configuration, the resulting scanning pattern can be regarded as a set of parallel cross-sectional images, Fig. 2(b). To create a final OCT image, the parallel cross-sectional images are averaged. Since the cross-sectional images are acquired in slightly different positions on the sample, separated by distance y, the speckle pattern differs in each one and averaging leads to the reduction of the speckle contrast.
Fig. 2.
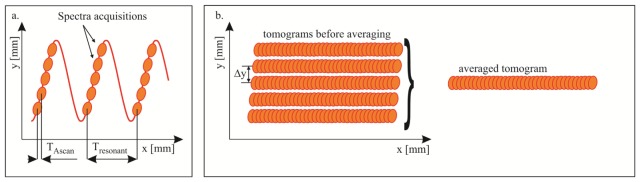
Schematic of the beam trajectory for one tomogram with reduced speckle pattern. a. Beam trajectory with marked positions of spectra acquisitions; TAscan – time span between spectra acquisitions, Tresonant – resonant scanner period and time span between spectra acquisitions with the same lateral y position. b. Schematic view of the spectra acquisition positions in a case with denser sampling in the x direction. Acquired spectra with the same lateral y position can be regarded as one of a set of parallel tomograms separated by the distance Δy in y direction. The distance Δy can be easily controlled by the operator. This set of tomograms is averaged to create one tomogram with a reduced speckle pattern.
The SOCT signal was acquired using a spectrometer equipped with a CMOS linescan camera (Sprint, Basler), to enable imaging with speeds up to 100,000 lines/s (10 μs repetition time and 8.6 μs exposure time). The CMOS detector was set to acquire 2048 pixels. As a result, the maximum number of SOCT signals acquired at the linear part of the slope of the sinusoidal trajectory was 8. Reduction of the speckle contrast can be controlled by setting the amplitude of the resonant scanner vibrations (the orthogonal beam dither amplitude). In our experiments, we set the optimal value of the beam deflection by maximizing the value of the contrast to noise ratio (CNR) of the averaged tomogram, as described previously [9]. Taking into account the exposure time of the camera and number of the averaged A-scans, the optimal value of the orthogonal beam dither amplitude was determined to be 75 μm.
2.2 Patients and surgical procedure
Studies presented in this article were approved by Ethic Committee on Clinical Investigation of Nicolaus Copernicus University, in accordance to the tenets of the Helsinki. Informed written consent was obtained from all patients, before the SOCT measurement.
A total of 40 eyes of 20 patients (mean age 31 ± 5.67 years) with myopia or myopic compound astigmatism (mean SE −3.88 ± 1.89 D) were enrolled into this prospective study. Patients who met the following criteria were excluded: (1) patients with any general health problems, (2) patients with a history of previous eye surgeries, (3), eyes with ocular pathologies (4) traumas and (5) scars. In 20 eyes, conventional PRK with alcohol-assisted epithelial removal was performed (PRK group) and 20 eyes were treated with transepithelial PRK (TransPRK group). Both eyes of the same patient were treated with the same technique. Groups were matched with respect to age, gender and preoperative refractive error. Before the surgery proparacaine hydrochloride 0.5% drops (Alcaine, Alcon, USA) were instilled 3 times within a 5 minute interval. The eyes were exposed using a wire lid speculum. In the PRK group, the cornea was exposed to 20% ethylic alcohol solution for 30 seconds with the aid of a well. Superficial cut of the epithelium was subsequently done with either 8.5 or 9.5 mm diameter trephine. Mean diameter of the epithelial removal was 9.2 ± 0.5 mm. In TransPRK group the epithelium was removed during laser ablation only from the area of total ablation zone, which diameter was within the range of 7.52 mm to 9.7 mm, mean 8.29 ± 0.47 mm. There was a statistically significant difference in mean diameter of the epithelial removal between groups (P<0.001). All surgeries were performed with the Amaris 750 S (Schwind eye-tech-solutions, Germany). In all cases, 0.02% mitomycin C (MMC) was applied for 2 min. Intraoperative complications were not noted. After the surgery, a bandage contact lens was applied (Acuvue Oasis, J&J, USA) for 6 to 7 days. The postoperative regimen included 0.3% tobramycin drops (Tobrexan, Alcon, USA) for one month, 0.1% diclofenac drops (Dicloabak, Laboratoires THEA, France) for one month, 0.15% hyaluronic acid (Biolan, Penta Arzneimittel, Germany) for 3 months, and 0.1% dexamethasone drops (Dexafree, Laboratoires THEA, France) 3 times a day in the first month, 2 times a day in the second month, and once a day in the third month. Ophthalmic examination and SOCT measurements were performed as follow: one day before the surgery, once a day in the first week after surgery, once per week during the next 4 weeks, as well as 2 and 3 months after surgery. The postoperative course was uneventful in all eyes.
2.3 Data analysis
The applicability of Spectral OCT (SOCT) with a novel speckle contrast reduction technique for assessment of the corneal surface changes after excimer laser photorefractive keratectomy was evaluated qualitatively and representative tomograms are presented on Fig. 3 and Fig. 4 . Statistical analysis was done to compare healing process between conventional PRK and TransPRK with the use of Wilcoxon Signed Rank test (diameter of the epithelial removal before the surgery, time to cover the stroma with epithelium, changes of central thickness of the epithelium), Fisher's exact test (increased reflectivity in the region close to the limbus in first 14 postoperative days) or Student's test (preoperative and postoperative manifest refraction spherical equivalent, evolution of uncorrected distant visual acuity). For all tests P<0.05 was considered statistically significant.
Fig. 3.

SOCT tomograms of the central cornea and peripheral cornea with limbus, acquired before the surgery and in the first postoperative day after PRK and TransPRK. Legend: CEP – corneal epithelium, BECL – basal epithelial cell layer, BL – Bowman’s layer, ST – stroma, DM – Descemet’s membrane, LEP – limbal epithelium, CJ – conjunctiva, SC – sclera, CL – contact lens, OP – opaque epithelium, RE – regrown epithelium, EC – cut of the epithelium, IR – inflammatory response, HEP – hyperreflective epithelium, SSI – stromal surface irregularities, (stars) – artifacts caused by specular reflection. The preoperative refractive error of the eye after PRK was: −2.5Dsph −2.0Dcyl ax 172°, after TransPRK: −4.75Dsph −0.5Dcyl ax 80°. Scale bars in both direction represent 500 µm.
Fig. 4.

SOCT tomograms of the central cornea and peripheral cornea with limbus, acquired in the first postoperative weeks and 3 months after the surgery for PRK and TransPRK. Legend: HEP – hyperreflective epithelium, IR- inflammatory response, BECL – basal epithelial cell layer, HRD – hyperreflective dots, SSI – stromal surface irregularities, (stars) – artifacts caused by specular reflection. The preoperative refractive error of the eye after PRK was: −2.5Dsph −2.0Dcyl ax 172°, after TransPRK: −4.75Dsph −0.5Dcyl ax 80°. Scale bars in both direction represent 500 µm.
3. Results
Figure 3 shows SOCT tomograms of the central cornea and peripheral cornea with limbus, acquired before the surgery and in the first postoperative days. The left panel presents the results obtained from an example eye after PRK and the right after TransPRK. On the tomograms acquired immediately after surgery, part of the epithelium has highly increased reflectivity in the PRK case, which might have been caused by the use of alcohol solution (Fig. 3, OP). Part of Bowman’s layer, central to the removed epithelium, remains intact. The TransPRK procedure results in cuts of Bowman’s layer and epithelium almost in the same location (Fig. 3, EC), the epithelium is removed with the excimer laser only within the diameter of the total ablation zone. In both groups, the epithelium started to regrow from the periphery (Fig. 3, RE) during the first day after surgery. Tomograms from day 2 and later confirm that regrown epithelium has much higher reflectivity. By day 3, the stroma was completely covered with epithelium in the majority of eyes in TransPRK group. By day 4, the same process was finished in the corneas in the PRK group. The mean time to cover the stroma with epithelium was 3.6 ± 0.9 days in the PRK group and 2.4 ± 0.8 days in the TransPRK group (P<0.001). On days 4 and 5, the thickness of the epithelium reaches the maximal value and it has the highest reflectivity (Fig. 3, HEP). The evolution of the central epithelial thickness is shown in Table 1 .
Table 1. Mean preoperative and postoperative central thickness of the epithelium (CET) in subgroups.
| CET ± SD [μm] | PRK group | TransPRK group | P | |||
|---|---|---|---|---|---|---|
| Pre op | 52.60 ± 4.21 | 52.40 ± 3.96 | >0.05 | |||
| Day 4 | 61.20 ± 6.15 | 61.70 ± 6.14 | >0.05 | |||
| Day 7 | 59.12 ± 5.14 | 58.91 ± 5.05 | >0.05 | |||
| Week 2 | 55.06 ± 5.09 | 54.85 ± 4.93 | >0.05 | |||
| Week 3 | 53.02 ± 5.08 | 53.06 ± 5.09 | >0.05 | |||
| Month 3 | 53.05 ± 4.57 | 53.08 ± 4.44 | >0.05 |
Evolution of uncorrected distant visual acuity (UDVA) in subgroups is presented in Table 2 . Statistically significant differences were observed only in first and third postoperative day. Preoperative and postoperative mean manifest refraction spherical equivalent (MRSE) was similar in both groups.
Table 2. Mean preoperative and postoperative manifest refraction spherical equivalent (MRSE) and evolution of uncorrected distant visual acuity (UDVA) in subgroups.
| MRSE ± SD [D] | PRK group | TransPRK group | P | |||
|---|---|---|---|---|---|---|
| Pre op | −3.85 ± 1.89 | −3.91 ± 1.96 | >0.05 | |||
| Post op | −0.11 ± 0.21 | −0.12 ± 0.25 | >0.05 |
| UDVA ± SD [LogMAR] | PRK group | TransPRK group | P | |||
|---|---|---|---|---|---|---|
| Pre op | 0.85 ± 0.35 | 0.88 ± 0.36 | >0.05 | |||
| Day 1 | 0.29 ± 0.25 | 0.41 ± 0.29 | 0.026 | |||
| Day 2 | 0.38 ± 0.29 | 0.42 ± 0.31 | >0.05 | |||
| Day 3 | 0.32 ± 0.21 | 0.21 ± 0.22 | 0.023 | |||
| Day 4 | 0.22 ± 0.15 | 0.19 ± 0.14 | >0.05 | |||
| Day 5 | 0.12 ± 0.14 | 0.10 ± 0.15 | >0.05 | |||
| Week 2 | 0.06 ± 0.09 | 0.05 ± 0.09 | >0.05 | |||
| Week 3 | 0.02 ± 0.08 | −0.01 ± 0.09 | >0.05 | |||
| Month 3 | −0.08 ± 0.07 | −0.10 ± 0.07 | >0.05 |
Figure 4 presents further evolution of the postoperative changes of the same eyes. On day 14, the basal epithelial cell layer is detectable again at the periphery (Fig. 4, BCEL). On the tomograms presented for the PRK group between days 1 and 14, changes in the reflectivity of the superficial stroma are visible in the region close to the limbus (Fig. 3 and Fig. 4, IR). The area of very superficial stroma which has a lenticular shape and normal reflectivity is posteriorly bordered by the stroma of increased reflectivity due to an accumulation of hyperreflective dots We observed similar changes in 30% of eyes in the PRK group and 10% of eyes in the TransPRK group (P<0.05). Slightly increased reflectivity of the epithelium and the stroma, with small hyperreflective dots within the stroma, were observed until the 3rd month after surgery, regardless of the surgical technique (Fig. 4, HRD). The SOCT examination also revealed some irregularities of the stromal surface (Fig. 3 and Fig. 4, SSI). Those changes are very subtle just after the surgery, mostly pronounced on postoperative days 4 and 5, and still visible 3 months after the surgery. The magnitude of the irregularities, which is difficult to measure objectively, is not dependent on the technique.
4. Discussion
SOCT was first used for examination of the cornea in 2006 and has since become a widely accepted diagnostic technique [10]. Currently, a number of commercially available instruments based on SOCT technology are able to provide tomograms of the anterior segment; however, the effective image resolution, defined as the smallest detectable detail, has not improved much since 2006. The clinical performance of OCT systems is dependent on several factors including resolution, system sensitivity, light penetration, and scanning speed. Among all of these, axial resolution is a key factor contributing to the performance of imaging. Prototype systems have reached axial resolutions of 2 µm in tissue, but when using expensive components. Another way to improve the performance of OCT is to reduce speckle pattern [11]. In our study, we implemented the novel technique of averaging 8 A-scans deflected orthogonally to the fast scanning axis. This allowed us to obtain tomograms with highly reduced contrast of speckle noise. This technique compromises lateral resolution in the direction perpendicular to the tomogram surface without affecting the lateral resolution along the tomogram. As a result, images with outstanding quality are obtained. The proposed technique is easy to implement in an OCT system, as it requires one additional resonant scanner deflecting the beam in the direction perpendicular to the fast scanning axis. A disadvantage of this technique is the reduced imaging speed, as the effective line-rate of the OCT device is equal to the frequency of the dithering device, what in our case was equal to 4 kHz.
The idea to use OCT for evaluation of epithelial healing is not new. In 2011, Pang et. al. published a paper on the applicability of a standard, commercial SOCT instrument for evaluation of corneal epithelial healing under a therapeutic contact lens after lamellar keratoplasty and Epi-LASIK procedures [12]. They concluded that SOCT is a valuable imaging tool for monitoring the progression of epithelial healing in situ in patients following corneal surgical procedures. Examination of the corneas after laser refractive surgery with SOCT and the novel speckle reduction technique demonstrated that this new technology further improves the diagnostic possibilities. Detailed tomograms provided new information of clinical value regarding the healing process after laser PRK.
The second aim of this paper was to reveal differences, detectable by SOCT, in the healing process between conventional alcohol-assisted PRK and transepithelial PRK. Both procedures were performed with a Schwind Amaris 750 S and a recently introduced TransPRK algorithm was used for transepithelial PRK. In TransPRK, both epithelium and stroma are removed in a single ablation profile, taking into account the epithelial thickness. Calculation is based on two different ablation values per pulse, one for the epithelium, where the laser ablates more tissue per pulse, and the other for the stroma. This makes the procedure more precise and initial clinical results are very encouraging [13–15]. TransPRK has several advantages, including reduced surgery time, less dehydration, no alcohol use, reduced inconvenience for the patient, and that the epithelium removed is the same diameter as the total ablation zone. A major disadvantage of transepithelial PRK is the higher total energy load delivered to the cornea by the excimer laser. However, in our study, we did not detect any differences between surgical techniques that may be caused by different energy.
The main difference between PRK and TransPRK in the healing process was the time to cover the stroma with epithelium, which was shorter in the TransPRK group, probably due to the difference in mean diameter of the epithelial removal between groups. It might be the reason for statistically significant differences in UDVA in postoperative day 1 and 3, because the highest decrease of visual acuity is observed when regrowing epithelium reaches the center of the cornea. On the tomograms presented in Fig. 3 for the PRK group between days 1 and 14, changes are visible in the reflectivity of the superficial stroma in the region close to the limbus. We observed similar changes statistically more often in the PRK group and we speculate that this is a sign of more intensive inflammatory response, which might have been caused by the use of alcohol solution. In an animal study, Panagiotopoulos et al. observed numerous fibroblast-like cells, granulocytes, and monocytes adjacent to the stromal surface after excimer laser ablation, mainly during the 1st and 2nd week after surgery [16].
Another very interesting observation is that SOCT enabled the detection of irregularities of the stromal surface, which were very subtle just after the surgery, mostly pronounced on postoperative days 4 and 5, and still visible 3 months after surgery (Fig. 3 and Fig. 4, SSI). They were not dependent on the technique and did not prevent form achieving a good UDVA 3 months after the surgery. The laser used in the study (Schwind Amaris 750 S) was a very small spot, high repetition rate laser with two fluence levels. About 80% of the ablation was performed with a high fluence value and for the remaining 20%, it automatically switches to a lower fluence to obtain optimal smoothing of the cornea. Nevertheless, stromal surface irregularities were still detectable 3 months after the surgery. Fortunately, histological studies of the wound healing response, in the presence of stromal irregularities, after excimer laser treatment in animal models demonstrated there are two mechanisms responsible for regaining corneal surface regularity [16]. First, the regrowing epithelium covers the irregular surface and has the ability to mask minor defects of the curvature. Second, wound healing reactivity creates an even surface by absorption of irregularities of stromal wound bed and by producing new stromal tissue. However, this process may take several months. Higher post-ablation irregularities induce more pronounced healing reactions when compared to a smoother ablation surface [17]. The presence of small hyperreflective dots within the stroma 3 month after the surgery confirms that the final healing process is not finished. During the first weeks after the surgery increased reflectivity of the stroma with hyper-reflective dots, is mainly caused by progressive repopulation from the subjacent activated keratocytes that migrate into the ablated stroma. In course of healing process these cells transform into myofibroblasts and are associated with an increase in extracellular matrix, being responsible for new collagen creation. The later process may be responsible for increased reflectivity of the anterior stroma many months after the ablation [18,19].
Our study has several limitations. One of the inherent disadvantages of OCT technology is inability to measure the reflectivity of the structures quantitatively. Moreover, the brightness of cornea in the presented images is a combination of three factors. Firstly, the sensitivity of the SOCT setup changed slightly during the months of the study. Secondly, the reflectivity of the cornea changes between subjects and the third reason is that due to the lack of precise positioning system, the images are acquired at different angle of incidence of the probing OCT beam. Another important limitation of the study is that tomograms were evaluated subjectively. However, even this stage of the work show applicability of the imaging technique to resolve anatomical structures like Bowman’s or basal epithelial cell layers during postoperative healing. In our SOCT study we found out that healing process is still not finished 3 months after the surgery and it would be beneficial to continue the observations up to 6 or 12 months.
In conclusion, SOCT with a novel speckle contrast reduction technique improves the effective image resolution of tomograms and provides information of clinical value regarding the healing process after excimer laser PRK. The main difference between the healing processes of PRK and TransPRK, assessed by SOCT, was the time to cover the stroma with epithelium, which was shorter in TransPRK group.
Acknowledgments
This work was supported by the TEAM/2012 project financed by European Union within the frames of Innovative Economy coordinated by Foundation for Polish Science and the National Laboratory of Quantum Technology. Danuta Bukowska and Maciej Szkulmowski acknowledge the National Center for Research and Development Grant No. PBS1/A9/20/2013. Maciej Szkulmowski additionally acknowledges Polish Ministry of Science and Higher Education grants for years 2011-2014.
References and links
- 1.Abad J. C., An B., Power W. J., Foster C. S., Azar D. T., Talamo J. H., “A prospective evaluation of alcohol-assisted versus mechanical epithelial removal before photorefractive keratectomy,” Ophthalmology 104(10), 1566–1575 (1997). 10.1016/S0161-6420(97)30095-5 [DOI] [PubMed] [Google Scholar]
- 2.Seiler T., Bende T., Wollensak J., ““[Laser surgery of the cornea],” Fortschritte der Ophthalmologie,” Zeitschrift der Deutschen Ophthalmologischen Gesellschaft 84, 513–518 (1987). [PubMed] [Google Scholar]
- 3.Camellin M., “Laser epithelial keratomileusis for myopia,” J. Refract. Surg. 19(6), 666–670 (2003). [DOI] [PubMed] [Google Scholar]
- 4.Pallikaris I. G., Katsanevaki V. J., Kalyvianaki M. I., Naoumidi I. I., “Advances in subepithelial excimer refractive surgery techniques: Epi-LASIK,” Curr. Opin. Ophthalmol. 14(4), 207–212 (2003). 10.1097/00055735-200308000-00007 [DOI] [PubMed] [Google Scholar]
- 5.Carr J. D., Patel R., Hersh P. S., “Management of late corneal haze following photorefractive keratectomy,” J. Refract. Surg. 11(3Suppl), S309–S313 (1995). [DOI] [PubMed] [Google Scholar]
- 6.Kanitkar K. D., Camp J., Humble H., Shen D. J., Wang M. X., “Pain after epithelial removal by ethanol-assisted mechanical versus transepithelial excimer laser debridement,” J. Refract. Surg. 16(5), 519–522 (2000). [DOI] [PubMed] [Google Scholar]
- 7.Lee H. K., Lee K. S., Kim J. K., Kim H. C., Seo K. R., Kim E. K., “Epithelial healing and clinical outcomes in excimer laser photorefractive surgery following three epithelial removal techniques: mechanical, alcohol, and excimer laser,” Am. J. Ophthalmol. 139(1), 56–63 (2005). 10.1016/j.ajo.2004.08.049 [DOI] [PubMed] [Google Scholar]
- 8.Reinstein D. Z., Archer T. J., Gobbe M., Silverman R. H., Coleman D. J., “Epithelial thickness in the normal cornea: three-dimensional display with Artemis very high-frequency digital ultrasound,” J. Refract. Surg. 24(6), 571–581 (2008). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Szkulmowski M., Gorczynska I., Szlag D., Sylwestrzak M., Kowalczyk A., Wojtkowski M., “Efficient reduction of speckle noise in Optical Coherence Tomography,” Opt. Express 20(2), 1337–1359 (2012). 10.1364/OE.20.001337 [DOI] [PubMed] [Google Scholar]
- 10.Kaluzny B. J., Kałuzny J. J., Szkulmowska A., Gorczyńska I., Szkulmowski M., Bajraszewski T., Wojtkowski M., Targowski P., “Spectral optical coherence tomography: a novel technique for cornea imaging,” Cornea 25(8), 960–965 (2006). 10.1097/01.ico.0000224644.81719.59 [DOI] [PubMed] [Google Scholar]
- 11.Wojtkowski M., Kaluzny B., Zawadzki R. J., “New directions in ophthalmic optical coherence tomography,” Optom. Vis. Sci. 89(5), 524–542 (2012). 10.1097/OPX.0b013e31824eecb2 [DOI] [PubMed] [Google Scholar]
- 12.Pang C. E., M V., Tan D. T., Mehta J. S., “Evaluation of Corneal Epithelial Healing Under Contact Lens with Spectral-Domain Anterior Segment Optical Coherence Tomography (SD-OCT),” Open Ophthalmol. J. 5(1), 51–54 (2011). 10.2174/1874364101105010051 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Aslanides I. M., Padroni S., Arba Mosquera S., Ioannides A., Mukherjee A., “Comparison of single-step reverse transepithelial all-surface laser ablation (ASLA) to alcohol-assisted photorefractive keratectomy,” Clin. Ophthalmol. 6, 973–980 (2012). 10.2147/OPTH.S32374 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fadlallah A., Fahed D., Khalil K., Dunia I., Menassa J., El Rami H., Chlela E., Fahed S., “Transepithelial photorefractive keratectomy: clinical results,” J. Cataract Refract. Surg. 37(10), 1852–1857 (2011). 10.1016/j.jcrs.2011.04.029 [DOI] [PubMed] [Google Scholar]
- 15.Luger M. H., Ewering T., Arba-Mosquera S., “Consecutive myopia correction with transepithelial versus alcohol-assisted photorefractive keratectomy in contralateral eyes: one-year results,” J. Cataract Refract. Surg. 38(8), 1414–1423 (2012). 10.1016/j.jcrs.2012.03.028 [DOI] [PubMed] [Google Scholar]
- 16.Panagiotopoulos M., Gan L., Fagerholm P., “Stroma remodelling during healing of corneal surface irregularities induced by PTK,” Acta Ophthalmol. Scand. 85(4), 387–394 (2007). 10.1111/j.1600-0420.2006.00852.x [DOI] [PubMed] [Google Scholar]
- 17.Weber B. A., Gan L., Fagerholm P., “Wound healing response in the presence of stromal irregularities after excimer laser treatment,” Acta Ophthalmol. Scand. 79(4), 381–388 (2001). 10.1034/j.1600-0420.2001.079004381.x [DOI] [PubMed] [Google Scholar]
- 18.Linna T., Tervo T., “Real-time confocal microscopic observations on human corneal nerves and wound healing after excimer laser photorefractive keratectomy,” Curr. Eye Res. 16(7), 640–649 (1997). 10.1076/ceyr.16.7.640.5058 [DOI] [PubMed] [Google Scholar]
- 19.Møller-Pedersen T., Li H. F., Petroll W. M., Cavanagh H. D., Jester J. V., “Confocal microscopic characterization of wound repair after photorefractive keratectomy,” Invest. Ophthalmol. Vis. Sci. 39(3), 487–501 (1998). [PubMed] [Google Scholar]