

Abstract
Femoral neck osteoplasty is an integral component for successful treatment of femoroacetabular impingement. Current techniques allow this to be performed arthroscopically, and results are equivalent to those of open procedures when typical anterior and anterosuperior lesions are considered. The arthroscopic procedure is dependent on obtaining adequate visualization through capsular management and proper leg positioning, and it requires fluoroscopy to guide and verify an adequate resection. We present our preferred technique for arthroscopic femoral neck osteoplasty.
Femoroacetabular impingement (FAI) is a well-recognized cause of hip pain in young adults and is associated with early-onset osteoarthritis.1 Two subtypes of impingement (pincer and cam) exist, and although they can occur independently, they most commonly coexist in an impinging hip.2 Cam impingement occurs as a result of an aspherical femoral head or a decreased femoral head-neck offset; this abnormal bony morphology is also sometimes referred to as a pistol-grip or tilt deformity. With hip motion, the abnormal bony prominence is repetitively forced into a generally spherical acetabulum, generating shear forces that can potentially result in tearing of the labrum and delamination of articular cartilage in the anterosuperior aspect of the acetabulum.
Cam lesions are common. Recent studies in healthy volunteers have found that up to 35% of men and 10% of women have evidence of cam morphology on imaging studies (radiographs or magnetic resonance imaging).3,4 The prevalence is even higher among young, active male subjects, with studies of asymptomatic football and hockey players showing evidence of cam morphology in up to 75% of imaged hips.5,6 Given the commonality of this lesion, the young population affected, and the potential for adverse long-term hip outcomes, the ability to effectively treat this lesion is paramount.
The goal of treatment of symptomatic impinging cam lesions is to restore a spherical femoral head and a normal head-neck offset, thereby eliminating the impinging bone. Originally, this required an open approach as popularized by Ganz et al.7; however, with recent technique advancements, this can now be performed arthroscopically. In the accompanying video presentation (Video 1), we demonstrate our technique for arthroscopic femoral neck osteoplasty for impinging cam lesions.
Surgical Technique
Hip arthroscopy is performed in the usual fashion. It is our preference to perform this with the patient in the supine position using an anterolateral portal for viewing and a mid-anterior portal for working for the majority of the procedure. Additional working portals can be created as needed to facilitate cam resection in different locations on the femoral head and neck. Pathology in the central compartment is addressed first. This includes a pincer resection and/or labral repair, as appropriate. It also includes addressing areas of acetabular chondral delamination, which may require resection of unstable cartilage and possibly microfracture of the subchondral bone.
Once work in the central compartment is completed, the traction on the lower extremities is released, and the femoral neck is visualized in the peripheral compartment. Though not shown in the accompanying video, our first step is to position the operative extremity in a slightly flexed, externally rotated, and abducted position. This relaxes the capsule so that we are able to visualize the superior retinacular vessels located posterosuperiorly along the femoral neck. We remain cognizant of this location throughout the case to prevent damage to these vessels, which could lead to avascular necrosis of the femoral head.
Leaving the hip in this position, we next inspect the medial extent of the cam lesion. If the lesion extends quite medially, we begin the resection with the hip in this position; however, for many lesions, this is not required. Next, we reposition the hip into a slightly flexed, abducted, and internally rotated position to optimize our arthroscopic view of the lesion. The fluoroscopy unit is also repositioned so that it is approximately 20° or 30° off of horizontal, as shown in Fig 1A. This re-creates the patient's preoperative cross-table lateral radiograph (Figs 1B and 1C) and allows us to monitor the amount of bony resection and to compare it with our preoperatively planned resection.
Fig 1.
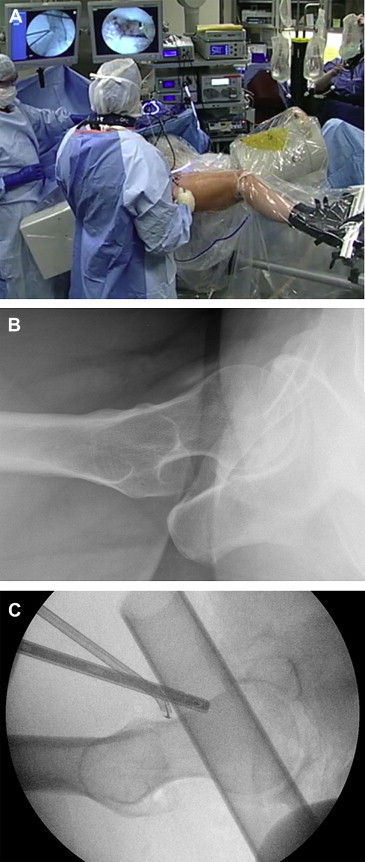
(A) Operative setup for the arthroscopic resection of a cam lesion of the right femoral neck. The majority of the resection is performed with the hip in a slightly flexed, abducted, and internally rotated position. The fluoroscopy unit is positioned approximately 20° or 30° off of horizontal because this re-creates the patient's preoperative cross-table lateral radiograph. (B) Preoperative cross-table lateral radiograph of right hip. (C) Intraoperative fluoroscopic view of right hip.
Once the leg is repositioned, we proceed with establishing adequate visualization of the cam lesion. If the cam lesion extends quite distally, this may necessitate creation of a descending capsulotomy limb along the femoral neck, producing a T-capsulotomy. This is performed with a sharp surgical blade (Banana Knife; Arthrex, Naples, FL) or by judicious use of a hip-specific shaver (Stryker, San Jose, CA) and/or an ArthroCare 50° radiofrequency wand (Austin, TX). We attempt to resect as little capsule as possible to facilitate capsular repair of at least the descending limb of the capsulotomy at the conclusion of the case.
Once we have established visualization, we use a hip-specific, 5.5-mm round burr (Stryker) in reverse mode to clear soft tissue and cartilage off of the cam lesion. The shaver and ArthroCare wand can also be used. We then proceed with bony resection in a systematic manner. We use the burr in reverse mode in areas where little resection is required and in forward mode, which is more aggressive, in areas where large amounts of resection are required or if the underlying bone is sclerotic. We start medially and distally and then work proximally and laterally. Often, we find that it is easiest to define the edges of the lesion first with the burr and then smooth away the remaining prominence in the middle. If the lesion extends quite proximally, the hip may need to be extended to ensure complete resection.
Once the majority of the lesion has been resected by working through the mid-anterior portal, we switch portals so that we can work through the anterolateral portal (Fig 2). This allows us to resect and shape the more lateral aspect of the lesion. This working configuration, however, does place the retinacular vessels at greater risk for iatrogenic damage, so we remain vigilant of their position.
Fig 2.
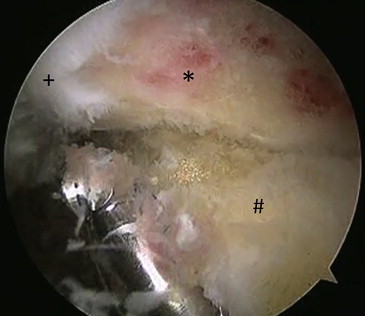
Arthroscopic view of the right femoral neck as viewed through the mid-anterior portal. The burr is introduced through the anterolateral portal to complete the resection of the lateral aspect of the cam lesion. (Asterisk, femoral neck; plus sign, femoral head; pound sign, capsule.)
Lastly, we switch portals again and perform a final shaping of the femoral neck, including a careful beveling of the cartilage-bone junction, to create a smooth concavity from what was initially a convexity (Fig 3). We then fluoroscopically verify a complete resection (Fig 4). We begin with a cross-table lateral projection and then image at various degree intervals while rotating the fluoroscopy unit into an anteroposterior projection. All images are scrutinized to ensure that we have created a spherical femoral head and an adequate head-neck offset. This completes the femoral neck osteoplasty. If a T-capsulotomy has been performed, the descending limb, at a minimum, is repaired; closure of the transverse component remains controversial. Table 1 reviews the key points in arthroscopic femoral neck osteoplasty.
Fig 3.
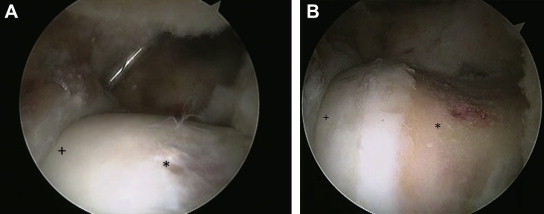
Arthroscopic view of the right femoral neck as viewed through the anterolateral portal (A) before and (B) after femoral neck osteoplasty. (Asterisk, femoral neck; plus sign, femoral head.)
Fig 4.
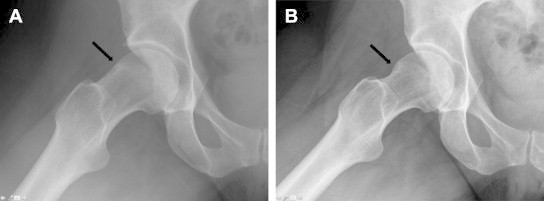
Frog-leg lateral radiographic images of the right hip (A) before and (B) after femoral neck osteoplasty. The arrow points to the cam lesion before resection and to the area of bony resection thereafter.
Table 1.
Key Points for Arthroscopic Femoral Neck Osteoplasty
| Remain cognizant of the position of the superior retinacular vessels throughout the case to prevent iatrogenic avascular necrosis of the femoral head. |
| Use a T-capsulotomy to increase visualization, especially if the cam lesion extends distally. |
| The majority of the resection is performed with the hip in a slightly flexed, abducted, and internally rotated position. |
| The medial extent of the cam lesion can be accessed by slight external rotation of the hip. |
| The lateral extent can be accessed by working through the anterolateral portal. |
| The proximal extent can be accessed by placing the hip in full extension. |
| Use fluoroscopy to guide the resection and to verify a complete resection. |
| Repair the descending limb of the T-capsulotomy to avoid iatrogenic instability of the hip. |
Discussion
Surgical treatment of FAI is effective. Recent systematic reviews have shown overall improvements in hip function scores and reductions in the severity of symptoms at short-term and midterm follow-up.8-11 These outcomes have not been shown to differ significantly based on technique (arthroscopic, mini-open, or open).8-11 When the treatment of typical anterior and anterosuperior cam lesions is specifically considered, the arthroscopic and open techniques are similar in that clinical studies have shown equivalent decreases in the extended-neck lateral alpha angle and improvement in the head-neck offset12; cadaveric studies have shown equivalent bony resections in terms of volume, depth, width, and overall arc of resection.13,14 However, Bedi et al.12 did find a significantly greater reduction in the anteroposterior alpha angle when an open approach was used in comparison to an arthroscopic approach. They suggested, therefore, that posterosuperior lesions might be more adequately addressed through an open approach with surgical dislocation.
Arthroscopic surgery has many advantages in comparison to open surgery, including reduced hospital admissions, decreased surgical morbidity, and a lower major complication rate.10 Systematic reviews have shown a major complication rate of up to 20% for open surgery and up to 5% for arthroscopic surgery.10,15 Unique to open surgery are trochanteric osteotomy–related complications, including nonunion and prominent hardware; there is also a higher risk of osteonecrosis.12 Inherent to arthroscopy, however, are the risks of abdominal compartment syndrome and traction-related concerns, including neurapraxia of the sciatic, femoral, perineal, pudendal, and lateral femoral cutaneous nerves; pressure necrosis of the perineum; and anal and vaginal tears.15,16 Overall, hip arthroscopy is regarded as “relatively safe, with minimal risk for major perioperative complications.”10
The success of surgery for FAI is dependent on adequate bony resection. On the femoral side, we reason that re-creating a spherical femoral head and restoring a normal femoral head-neck offset will achieve this goal; however, there is little evidence to support this approach. Studies have shown that neither the magnitude of correction of the alpha angle nor correction of the alpha angle to less than 50° is correlated with postoperative outcomes of pain, function, or increases in range of motion.17,18 Although inadequate resection risks continued impingement, resection of greater than 30% of the femoral neck width risks fracture,19 and overzealous proximal resection or poor contouring of the head-neck junction risks disruption of the labral seal.16 Therefore the ideal amount of bony resection is a compromise and is dependent on surgeon judgment.20 This contributes to the learning curve associated with hip arthroscopy and femoral neck osteoplasty.
Femoral neck osteoplasty is an important component of the surgical management of FAI. This article and the accompanying video have described our preferred technique for the arthroscopic resection of femoral cam lesions. Arthroscopic techniques, in comparison to open techniques, have a lower major complication rate, decreased morbidity, and equivalent patient outcomes at short-term and midterm follow-up.
Footnotes
The authors report the following potential conflict of interest or source of funding: B.A.L. receives support from Arthrex, National Institutes of Health, and VOT Solutions.
Supplementary Data
Arthroscopic technique for femoral neck osteoplasty in right hip.
References
- 1.Ganz R., Parvizi J., Beck M., Leunig M., Notzli H., Siebenrock K.A. Femoroacetabular impingement: A cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;417:112–120. doi: 10.1097/01.blo.0000096804.78689.c2. [DOI] [PubMed] [Google Scholar]
- 2.Beck M., Kahlhor M., Leunig M., Ganz R. Hip morphology influences the pattern of acetabular cartilage damage. J Bone Joint Surg Br. 2005;87:1012–1018. doi: 10.1302/0301-620X.87B7.15203. [DOI] [PubMed] [Google Scholar]
- 3.Laborie L.B., Lehmann T.G., Engesæter I.Ø., Eastwood D.M., Engesæter L.B., Rosendahl K. Prevalence of radiographic findings thought to be associated with femoroacetabular impingement in a population-based cohort of 2081 healthy young adults. Radiology. 2011;260:494–502. doi: 10.1148/radiol.11102354. [DOI] [PubMed] [Google Scholar]
- 4.Hack K., Di Primio G., Rakhra K., Beaulé P.E. Prevalence of cam-type femoroacetabular impingement morphology in asymptomatic volunteers. J Bone Joint Surg Am. 2010;92:2436–2444. doi: 10.2106/JBJS.J.01280. [DOI] [PubMed] [Google Scholar]
- 5.Kapron A.L., Anderson A.E., Aoki S.K. Radiographic prevalence of femoroacetabular impingement in collegiate football players: AAOS exhibit selection. J Bone Joint Surg Am. 2011;93 doi: 10.2106/JBJS.K.00544. e111(1-10) [DOI] [PubMed] [Google Scholar]
- 6.Philippon M.J., Ho C.P., Briggs K.K., Stull J., Laprade R.F. Prevalence of increased alpha angles as a measure of cam-type femoroacetabular impingement in youth ice hockey players. Am J Sports Med. 2013;41:1357–1362. doi: 10.1177/0363546513483448. [DOI] [PubMed] [Google Scholar]
- 7.Ganz R., Gill T.J., Gautier E., Ganz K., Krugel N., Berlemann U. Surgical dislocation of the adult hip: A technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001;83:1119–1124. doi: 10.1302/0301-620x.83b8.11964. [DOI] [PubMed] [Google Scholar]
- 8.Bedi A., Chen N., Robertson W., Kelly B.T. The management of labral tears and femoroacetabular impingement of the hip in the young, active patient. Arthroscopy. 2008;24:1135–1145. doi: 10.1016/j.arthro.2008.06.001. [DOI] [PubMed] [Google Scholar]
- 9.Clohisy J.C., St John L.C., Schutz A.L. Surgical treatment of femoroacetabular impingement: A systematic review of the literature. Clin Orthop Relat Res. 2010;468:555–564. doi: 10.1007/s11999-009-1138-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Matsuda D.K., Carlisle J.C., Arthurs S.C., Wierks C.H., Philippon M.J. Comparative systematic review of the open dislocation, mini-open, and arthroscopic surgeries for femoroacetabular impingement. Arthroscopy. 2011;27:252–269. doi: 10.1016/j.arthro.2010.09.011. [DOI] [PubMed] [Google Scholar]
- 11.Ng V.Y., Arora N., Best T.M., Pan X., Ellis T.J. Efficacy of surgery for femoroacetabular impingement: A systematic review. Am J Sports Med. 2010;38:2337–2345. doi: 10.1177/0363546510365530. [DOI] [PubMed] [Google Scholar]
- 12.Bedi A., Zaltz I., De La Torre K., Kelly B.T. Radiographic comparison of surgical hip dislocation and hip arthroscopy for treatment of cam deformity in femoroacetabular impingement. Am J Sports Med. 2011;39(suppl):20S–28S. doi: 10.1177/0363546511412734. [DOI] [PubMed] [Google Scholar]
- 13.Mardones R., Lara J., Donndorff A. Surgical correction of “cam-type” femoroacetabular impingement: A cadaveric comparison of open versus arthroscopic debridement. Arthroscopy. 2009;25:175–182. doi: 10.1016/j.arthro.2008.09.011. [DOI] [PubMed] [Google Scholar]
- 14.Sussmann P.S., Ranawat A.S., Lipman J., Lorich D.G., Padgett D.E., Kelly B.T. Arthroscopic versus open osteoplasty of the head-neck junction: A cadaveric investigation. Arthroscopy. 2007;23:1257–1264. doi: 10.1016/j.arthro.2007.07.012. [DOI] [PubMed] [Google Scholar]
- 15.Bedi A., Kelly B.T., Khanduja V. Arthroscopic hip preservation surgery: Current concepts and perspective. Bone Joint J. 2013;95-B:10–19. doi: 10.1302/0301-620X.95B1.29608. [DOI] [PubMed] [Google Scholar]
- 16.Vaughn Z.D., Safran M.R. Arthroscopic femoral osteoplasty/chielectomy for cam-type femoroacetabular impingement in the athlete. Sports Med Arthrosc. 2010;18:90–99. doi: 10.1097/JSA.0b013e3181dfce63. [DOI] [PubMed] [Google Scholar]
- 17.Bedi A., Dolan M., Hetsroni I., Magennis E. Surgical treatment of femoroacetabular impingement improves hip kinematics: A computer-assisted model. Am J Sports Med. 2011;39(suppl):43S–49S. doi: 10.1177/0363546511414635. [DOI] [PubMed] [Google Scholar]
- 18.Stähelin L., Stähelin T., Jolles B.M., Herzog R.F. Arthroscopic offset restoration in femoroacetabular cam impingement: Accuracy and early clinical outcome. Arthroscopy. 2008;24:51–57. doi: 10.1016/j.arthro.2007.08.010. [DOI] [PubMed] [Google Scholar]
- 19.Mardones R.M., Gonzalez C., Chen Q., Zobitz M., Kaufman K.R., Trousdale R.T. Surgical treatment of femoroacetabular impingement: Evaluation of the effect of the size of the resection. J Bone Joint Surg Am. 2005;87:273–279. doi: 10.2106/JBJS.D.01793. [DOI] [PubMed] [Google Scholar]
- 20.Bedi A., Dolan M., Magennis E., Lipman J., Buly R., Kelly B.T. Computer-assisted modeling of osseous impingement and resection in femoroacetabular impingement. Arthroscopy. 2012;28:204–210. doi: 10.1016/j.arthro.2011.11.005. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Arthroscopic technique for femoral neck osteoplasty in right hip.