

Abstract
Femoral retroversion is an uncommon cause of cam femoroacetabular impingement that may require surgical treatment beyond arthroscopic or open femoroplasty. We present the case of a young adult with bilateral severe femoral retroversion in whom such treatment failed. We discuss the rationale, surgical technique, and outcome of this patient, who underwent bilateral closed intramedullary derotational proximal femoral osteotomies and interlocked nailing with adjunctive pre- and post-osteotomy hip arthroscopies. Clinical improvement with normal foot progression angles, radiographic union, and resolution of bilateral cam femoroacetabular impingement from femoral retroversion was achieved. This surgery permits rapid institution of weight-bearing ambulation and an early rehabilitative program. Femoral retroversion may be an underappreciated and insufficiently treated cause of cam femoroacetabular impingement that may be readily detected and successfully remedied with this less invasive procedure.
When the concept of femoroacetabular impingement (FAI) was introduced more than a decade ago, cam impingement from femoral retroversion was listed among several more common causes.1 On average, femoral anteversion ranges from 30° to 40° at birth and decreases progressively throughout growth, but the range of published normal values for adult femoral anteversion ranges from 8° to 20°,2-9 likely because of differences in imaging techniques and/or reference landmarks. One commonly used definition of femoral version is the angular difference between the axis of the femoral neck and the transepicondylar axis of the knee.8,10 A recent study found a mean femoral anteversion of 9° in patients who underwent hip arthroscopy for symptomatic FAI.9 Although the efficacy of surgery for FAI and the arthroscopic method in particular have gained support,11-14 there exists a paucity of information regarding the treatment of cam FAI from femoral retroversion. Femoral retroversion amplifies the effect of a cam lesion by engaging the cam lesion into the socket before the initiation of hip flexion.15 A cam lesion in a patient with normal or increased femoral anteversion may not be symptomatic until terminal hip flexion and internal rotation, with no significant restriction in range of motion, whereas a retroverted femur may engage the rim much sooner, resulting in significant pain and loss of internal rotation with daily activities. One large series showed femoral retroversion in 16.6% of patients with FAI and a significant correlation with osteoarthrosis in this patient population.16 Another study showed that although internal rotation improves after arthroscopic femoroplasty independent of femoral neck version, patients with abnormal version had altered internal rotation with increased values associated with increased anteversion and decreased values with relative retroversion.17
We present a technical note on closed intramedullary derotational osteotomy with adjuvant hip arthroscopy for eradication of secondary cam impingement arising from severe bilateral femoral retroversion.
Case
A 26-year-old man was referred to the primary author (D.K.M.) for consideration of revision hip arthroscopy versus possible intertrochanteric osteotomy for severe bilateral femoral retroversion with unabated bilateral deep groin pain despite right and sequential left arthroscopic hip surgeries. He had undergone arthroscopic acetabuloplasty with labral refixation and femoroplasty on each hip approximately 2 years earlier by the coauthor (H.D.M.). He stated that he still walked “like Charlie Chaplin” with noticeable out-toeing and had “never been able to in-toe.” His hip examinations showed marked limitation of internal rotation in both extension (internal rotation to 5°) and flexion (internal rotation to 5° with anterior impingement test). Radiographs showed postoperative recontouring of both hips with normal anterior offset ratios (0.21 on the right and 0.22 on the left) and alpha angles (45° bilaterally). Magnetic resonance imaging showed a transepicondylar femoral neck axis of −19° (right) and −9° (left) (Fig 1).
Fig 1.
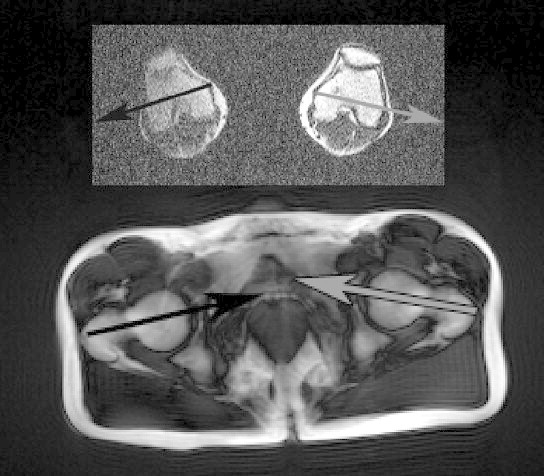
Preoperative magnetic resonance image showing femoral retroversion of both lower extremities. Distal femoral transepiphyseal axis and femoral neck axis of left (black arrows) and right (grey arrows) lower extremities.
The patient underwent closed right derotational osteotomy with interlocked nailing and adjuvant hip arthroscopy. He subsequently had the same procedure performed on the left lower extremity 3 months later. Both surgeries were performed with overnight hospitalization with immediate weight bearing to tolerance on 2 crutches. The patient had uneventful postoperative courses with full weight bearing without upper extremity aids at 3 weeks and clinical and radiographic union by 3 months. At 15 months and 12 months after the right and left surgeries, respectively, he is able to walk and jog with improved foot progression angles and wants to return to military duty after removal of all metal implants.
Surgical Technique
This procedure is a modification of an osteotomy technique originated by Dr. Robert Buly with adjunctive arthroscopic assistance. The patient was placed on a fracture table in the supine position. Hip arthroscopy under general anesthesia was performed through the anterolateral viewing portal with a 70° arthroscope and a modified mid-anterior working portal. Under hip distraction, diagnostic and therapeutic hip arthroscopy was initiated. In this case the anterosuperior labrum was frayed without gross detachment (after previous acetabuloplasty and labral refixation), and the previous anterior femoroplasty site appeared sufficiently recontoured without gross under- or over-resection (Fig 2). Conservative arthroscopic selective labral debridement with a mechanical shaver was performed, with preservation of the labral fluid seal. Blocked internal rotation to 10° on intraoperative anterior impingement testing was confirmed on dynamic arthroscopic visualization with premature abutment of the anteromedial femoral head-neck junction against the anterosuperior acetabular rim. After hip arthroscopy, a seamless progression to derotational osteotomy was performed without a change in setup or re-draping.
Fig 2.
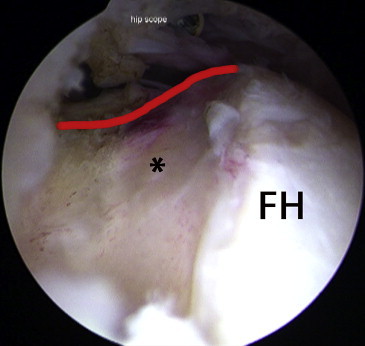
Pre-osteotomy supine arthroscopic image of left hip, as viewed from anterolateral portal, showing sufficient previous femoroplasty (asterisk). The red line depicts sufficient anterior offset. (FH, femoral head.)
By use of a fluoroscopic C-arm device positioned between the legs so as to enable anteroposterior and lateral projections of the entire left femur, parallel lateral-based Steinmann pins were placed on each side of the proposed osteotomy. The proximal pin was placed through the anterolateral portal into the anterior aspect of the greater trochanter (to avoid intramedullary obstruction) and the distal pin in the transcondylar region. The anteroposterior location of the latter was not critical because the rod did not extend to this level.
A 3-cm vertical incision was made proximal to the greater trochanter with subsequent dissection to its apex. Apical trochanteric pin placement and proximal femoral entry were established under bi-plane fluoroscopic guidance. An intramedullary saw (Winquist saw; Biomet, Warsaw, IN) was selected to match the anticipated maximal external diameter of cortical bone at a level 5 to 6 cm distal to the lesser trochanter. With the saw blade retracted behind the protective cam-shaped tip, antegrade intramedullary insertion was achieved (Fig 3). Once confirmed in the desired intramedullary position, the saw blade was progressively protracted by clockwise rotation of a proximal-based external dial and axial saw rotation performed in incremental fashion until the closed transverse osteotomy was completed (Fig 4). The saw blade was then fully retracted behind the protective cam by continuing to dial in the same clockwise direction (until the dial read “0”) and carefully extracted from the femoral canal.
Fig 3.
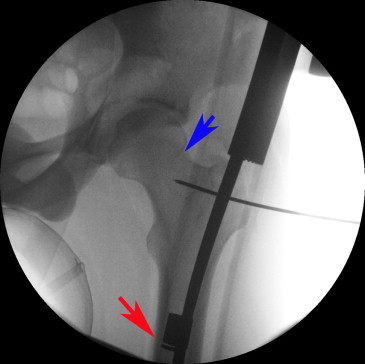
Intraoperative fluoroscopic image after insertion of intramedullary saw to level of desired osteotomy. One should note that the saw blade is protected behind the distal cam (red arrow), enabling insertion and removal from the femoral intramedullary canal. The area of previous arthroscopic femoroplasty (blue arrow) should also be noted.
Fig 4.
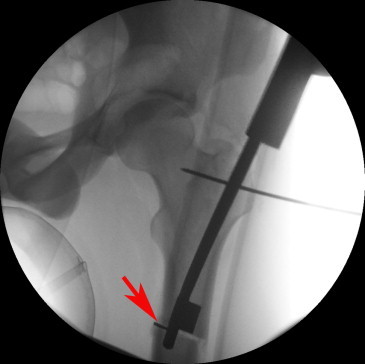
Intraoperative fluoroscopic image showing intramedullary transverse osteotomy at subtrochanteric level of left femur. One should note the deployed saw blade from “under” the protective metallic cam (arrow).
A reamed intramedullary rod (titanium trochanteric fixation nail system [TFN]; Synthes, West Chester, PA) was then partially seated across the osteotomy site, and controlled internal rotation of the distal segment was performed. To assess sufficient derotation, we viewed the divergence of the parallel-placed pins from a distal-based axial perspective.18 An angular guide (Blade plate guide; Synthes) was used to measure the relative angular degree of rotation. We chose to overcorrect slightly by using a 30° correction for this left femur. Once achieved, the intramedullary rod was fully inserted and proximal screw placement was performed under fluoroscopic guidance. Before placement of a distal interlocking screw, axial alignment and the absence of inadvertent osteotomy site distraction were confirmed.
Repeat hip arthroscopy confirmed impingement-free internal rotation to 30° with flexion–adduction–internal rotation testing. Once we were satisfied with the rotational correction of the femoral deformity, foot alignment in both hip and knee extension, as well as hip and knee flexion, was checked to ensure the absence of any significant compensatory tibial rotational deformity. The supplemental video demonstrates the aforementioned surgery and highlights key procedural steps (Video 1).
Discussion
The primary significance of this technical report is 2-fold. By bringing femoral retroversion into the differential diagnostic algorithm of FAI, perhaps some patients who have eluded diagnosis and/or sufficient treatment may benefit. Moreover, we describe a less invasive option that may have applicability in correcting more severe deformities.
The classic description of cam FAI includes an abnormal thickness of the femoral neck and/or asphericity at the femoral head-neck junction. The former condition may be reflected by a decreased anterior offset ratio19; the latter, by an increased alpha angle.20 However, we submit that cam FAI may occur in the absence of these findings with femoral retroversion. Though defined as less than 5° of anteversion, femoral retroversion in a clinical sense may be better defined as less than 0° of anteversion (i.e., some degree of true retroversion). The detection of this deformity on physical examination may include an out-toeing gait and significantly less internal than external rotation tested in hip extension and in flexion (with anterior impingement testing). Among various imaging modalities measuring femoral version, magnetic resonance imaging and computed tomography are arguably the most used, with either the distal femoral transepicondylar axis or posterior condylar line being used as a reference.21-23 We suggest that symptomatic patients with suspected cam FAI from femoral retroversion on physical examination undergo magnetic resonance imaging or computed tomography.
If relatively minor retroversion is confirmed, we would consider arthroscopic treatment in the form of femoroplasty. Hip internal rotation can improve to some degree after arthroscopic femoroplasty even in the setting of femoral retroversion.17 Although, conceptually, femoroplasty can eradicate even severe cam FAI, volumetric resection of large amounts of bone at the femoral head-neck junction may predispose to iatrogenic femoral neck fracture.24 Moreover, in patients with a pincer component of FAI, anterosuperior rim reduction may help gain hip internal rotation. Traditional open corrective osteotomy at the intertrochanteric or subtrochanteric level may be quite invasive. Hip arthroscopy before derotational osteotomy permits arthroscopic diagnosis and treatment of chondrolabral dysfunction and acetabular and/or femoral bony protrusions. Moreover, it enables precise assessment of the severity and location of residual femoroacetabular abutment from femoral retroversion after cam decompression with femoral osteochondroplasty. The Winquist intramedullary saw enables a less invasive uniplanar derotational osteotomy through small incisions. Controlled rotational correction by internal rotation of the distal femoral shaft is confirmed with an axial change in initial parallel pin placement, improved foot position, and increased internal rotation with the anterior impingement test. Though uncommon, significant compensatory tibial external torsion may affect the desired amount of derotation and, in fact, may merit tibial derotation osteotomy25 (distal segment rotated externally), yielding a 2-level procedure (R. Buly, oral communication, September 2012). Secure interlocked intramedullary fixation permits early postoperative weight bearing through a stable transverse osteotomy. Post-osteotomy hip arthroscopy confirms eradication of ongoing FAI with dynamic testing. Although this can be performed without traction, we have not had any complications with the brief reapplication of traction through the osteotomized and stabilized femur.
Our patient had rapid radiographic union of both proximal femurs by 3 months postoperatively. The right osteotomy site healed without noticeable deformity (Fig 5). The left osteotomy site had 6° of varus deformity (Fig 6) with the mechanical axis into the medial compartment of the knee. Selecting an undersized intramedullary saw may not complete the osteotomy, but an oversized saw may require excessive reaming that may decrease tight control of valgus-varus/flexion-extension.
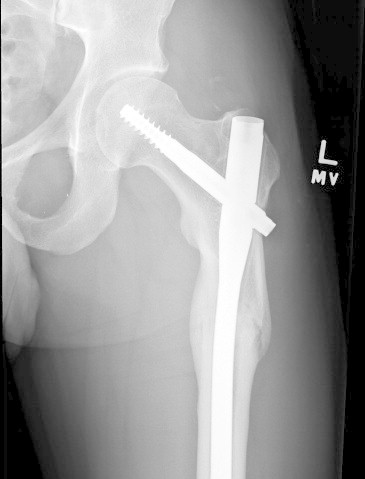
Fig 5.

Postoperative anteroposterior radiograph of right femur showing healed derotational osteotomy.
Fig 6.
Postoperative anteroposterior radiograph of left femur showing healed derotational osteotomy.
Closed derotational osteotomy may have expanded applications. Excessive femoral anteversion, especially when combined with excessive acetabular anteversion, may cause symptomatic anterior instability. With the exception of external rather than internal rotation of the distal femoral segment, select patients with excessive femoral anteversion may benefit from the described procedure. Moreover, patients with acquired rotational deformities due to malunited femur fractures may be candidates for this procedure.26,27
The ideal technique for femoral derotational osteotomy has been described as simple, involving little or no immobilization and reliably maintaining operative correction, with a high level of cosmesis and a low risk of complications.28 Closed derotational femoral osteotomy achieves these goals. In addition, early weight bearing with load-sharing intramedullary rod fixation is allowed and in fact encouraged, making possible single staged bilateral derotational osteotomies. The infection risk may be lessened because the osteotomy site is not formally opened. Moreover, arthroscopic assistance enables assessment and treatment of intra-articular pathology before derotational osteotomy and confirmation of improved dynamic femoroacetabular interaction afterward.
Femoral retroversion is a potential treatable cause of secondary cam FAI, even despite previous arthroscopic femoroplasties. Closed intramedullary derotational osteotomy with adjunctive hip arthroscopy is feasible, offering a less invasive option than open derotational osteotomy plus the benefits of load-sharing fixation. Concurrent hip arthroscopy enables dynamic assessment of the often critical femoroacetabular interaction and treatment of coexistent intra-articular pathology. This procedure may have an application in the treatment of severe femoral retroversion and anteversion deformities.
Acknowledgment
The authors acknowledge Robert Buly, M.D., from the Hospital for Special Surgery, New York, New York.
Footnotes
The authors report the following potential conflict of interest or source of funding: D.K.M. receives support from Board of Orthopedics Overseas and Editorial Board Arthroscopy and Orthopedics Today. He receives no monies from any of these board positions. ArthroCare and Smith & Nephew. Intellectual property unrelated to this manuscript. H.D.M. receives support from Smith & Nephew and Pivot Medical.
Supplementary Data
Arthroscopic-assisted closed derotational osteotomy for cam femoroacetabular impingement from femoral retroversion.
References
- 1.Ganz R., Parvizi J., Beck M., Leunig M., Nötzli H., Siebenrock K.A. Femoroacetabular impingement: A cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;(417):112–120. doi: 10.1097/01.blo.0000096804.78689.c2. [DOI] [PubMed] [Google Scholar]
- 2.Bråten M., Terjesen T., Rossvoll I. Femoral anteversion in normal adults. Ultrasound measurements in 50 men and 50 women. Acta Orthop Scand. 1992;63:29–32. doi: 10.3109/17453679209154844. [DOI] [PubMed] [Google Scholar]
- 3.Reikerås O., Bjerkreim I., Kolbenstvedt A. Anteversion of the acetabulum and femoral neck in normals and in patients with osteoarthritis of the hip. Acta Orthop Scand. 1983;54:18–23. doi: 10.3109/17453678308992864. [DOI] [PubMed] [Google Scholar]
- 4.Kim J.S., Park T.S., Park S.B., Kim J.S., Kim I.Y., Kim S.I. Measurement of femoral neck anteversion in 3D. Part 1: 3D imaging method. Med Biol Eng Comput. 2000;38:603–609. doi: 10.1007/BF02344864. [DOI] [PubMed] [Google Scholar]
- 5.Sugano N., Noble P.C., Kamaric E. A comparison of alternative methods of measuring femoral anteversion. J Comput Assist Tomogr. 1998;22:610–614. doi: 10.1097/00004728-199807000-00019. [DOI] [PubMed] [Google Scholar]
- 6.Kingsley P.C., Olmsted K.L. A study to determine the angle of anteversion of the neck of the femur. J Bone Joint Surg Am. 1948;30:745–751. [PubMed] [Google Scholar]
- 7.Ito K., Minka M.A., Leunig M., Werlen S., Ganz R. Femoroacetabular impingement and the cam-effect. A MRI-based quantitative anatomical study of the femoral head-neck offset. J Bone Joint Surg Br. 2001;83:171–176. doi: 10.1302/0301-620x.83b2.11092. [DOI] [PubMed] [Google Scholar]
- 8.Tomczak R.J., Guenther K.P., Rieber A., Mergo P., Ros P.R., Brambs H.J. MR imaging measurement of the femoral antetorsional angle as a new technique: Comparison with CT in children and adults. AJR Am J Roentgenol. 1997;168:791–794. doi: 10.2214/ajr.168.3.9057536. [DOI] [PubMed] [Google Scholar]
- 9.Ejnisman L., Philippon M.J., Lertwanich P. Relationship between femoral anteversion and findings in hips with femoroacetabular impingement. Orthopedics. 2013;36:e293–e300. doi: 10.3928/01477447-20130222-17. [DOI] [PubMed] [Google Scholar]
- 10.Hernandez R.J., Tachdjian M.O., Poznanski A.K., Dias L.S. CT determination of femoral torsion. AJR Am J Roentgenol. 1981;137:97–101. doi: 10.2214/ajr.137.1.97. [DOI] [PubMed] [Google Scholar]
- 11.Philippon M.J., Briggs K.K., Yen Y.M., Kuppersmith D.A. Outcomes following hip arthroscopy for femoroacetabular impingement with associated chondrolabral dysfunction: Minimum two-year follow-up. J Bone Joint Surg Br. 2009;91:16–23. doi: 10.1302/0301-620X.91B1.21329. [DOI] [PubMed] [Google Scholar]
- 12.Byrd J.W., Jones K.S. Arthroscopic femoroplasty in the management of cam-type femoroacetabular impingement. Clin Orthop Relat Res. 2009;467:739–746. doi: 10.1007/s11999-008-0659-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Matsuda D.K., Carlisle J.C., Arthurs S.C., Wierks C.H., Philippon M.J. Comparative systematic review of the open dislocation, mini-open, and arthroscopic surgeries for femoroacetabular impingement. Arthroscopy. 2011;27:252–269. doi: 10.1016/j.arthro.2010.09.011. [DOI] [PubMed] [Google Scholar]
- 14.Botser I.B., Smith T.W., Jr., Nasser R., Domb B.G. Open surgical dislocation versus arthroscopy for femoroacetabular impingement: A comparison of clinical outcomes. Arthroscopy. 2011;27:270–278. doi: 10.1016/j.arthro.2010.11.008. [DOI] [PubMed] [Google Scholar]
- 15.Bedi A., Dolan M., Hetsroni I. Surgical treatment of femoroacetabular impingement improves hip kinematics: A computer-assisted model. Am J Sports Med. 2011;39(suppl):43S–49S. doi: 10.1177/0363546511414635. [DOI] [PubMed] [Google Scholar]
- 16.Moya L., Buly R., Henn F., Kelly B., Ma Y., Molisani D. Femoral retroversion in patients with femoroacetabular impingement: A cofactor in the development of hip osteoarthritis. J Bone Joint Surg Br. 2010;92(suppl IV):526. [Google Scholar]
- 17.Kelly B.T., Bedi A., Robertson C.M., Dela Torre K., Giveans M.R., Larson C.M. Alterations in internal rotation and alpha angles are associated with arthroscopic cam decompression in the hip. Am J Sports Med. 2012;40:1107–1112. doi: 10.1177/0363546512437731. [DOI] [PubMed] [Google Scholar]
- 18.Türker M., Cirpar M., Cetik O., Senyücel C., Tekdemir I., Yalçinozan M. Comparison of two techniques in achieving planned correction angles in femoral subtrochanteric derotation osteotomy. J Pediatr Orthop B. 2012;21:215–219. doi: 10.1097/BPB.0b013e32834d4d01. [DOI] [PubMed] [Google Scholar]
- 19.Eijer H., Leunig M., Mahomed M.N., Ganz R. Crosstable lateral radiograph for screening of anterior femoral head–neck offset in patients with femoro-acetabular impingement. Hip Int. 2001;11:37–41. [Google Scholar]
- 20.Nötzli H.P., Wyss T.F., Stoecklin C.H., Schmid M.R., Treiber K., Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002;84:556–560. doi: 10.1302/0301-620x.84b4.12014. [DOI] [PubMed] [Google Scholar]
- 21.Ruwe P.A., Gage J.R., Ozonoff M.B., DeLuca P.A. Clinical determination of femoral anteversion. A comparison with established techniques. J Bone Joint Surg Am. 1992;74:820–830. [PubMed] [Google Scholar]
- 22.Hoiseth A., Reikeras O., Fonstelien E. Evaluation of three methods for measurement of femoral neck anteversion. Femoral neck anteversion, definition, measuring methods and errors. Acta Radiol. 1989;30:69–73. [PubMed] [Google Scholar]
- 23.Botser I.B., Ozoude G.C., Martin D.E., Siddiqi A.J., Kuppuswami S., Domb B.G. Femoral anteversion in the hip: Comparison of measurement by computed tomography, magnetic resonance imaging, and physical examination. Arthroscopy. 2012;28:619–627. doi: 10.1016/j.arthro.2011.10.021. [DOI] [PubMed] [Google Scholar]
- 24.Mardones R.M., Gonzalez C., Chen Q., Zobitz M., Kaufman K.R., Trousdale R.T. Surgical treatment of femoroacetabular impingement: Evaluation of the effect of the size of the resection. J Bone Joint Surg Am. 2005;87:273–279. doi: 10.2106/JBJS.D.01793. [DOI] [PubMed] [Google Scholar]
- 25.Walton D.M., Liu R.W., Farrow L.D., Thompson G.H. Proximal tibial derotation osteotomy for torsion of the tibia: A review of 43 cases. J Child Orthop. 2012;6:81–85. doi: 10.1007/s11832-012-0384-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Farquharson-Roberts M.A. Corrective osteotomy for combined shortening and rotational malunion of the femur. J Bone Joint Surg Br. 1995;77:979–980. [PubMed] [Google Scholar]
- 27.Jagernauth S., Tindall A.J., Kohli S., Allen P. New technique: A novel femoral derotation osteotomy for malrotation following intramedullary nailing. Case Rep Orthop. 2012;2012:837325. doi: 10.1155/2012/837325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Gordon J.E., Pappademos P.C., Schoenecker P.L., Dobbs M.B., Luhmann S. Diaphyseal derotational osteotomy with intramedullary fixation for correction of excessive femoral anteversion in children. J Pediatr Orthop. 2005;25:548–553. doi: 10.1097/01.bpo.0000158783.37602.cb. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Arthroscopic-assisted closed derotational osteotomy for cam femoroacetabular impingement from femoral retroversion.