

Abstract
The role of capsular repair in the arthroscopic treatment of femoroacetabular impingement remains poorly defined. Some surgeons rarely repair the capsule, whereas others perform repairs routinely. There is little direct clinical evidence to guide surgeon decision making. When capsular repairs are performed, the procedure requires adequate visualization and careful suture placement either to re-establish the patient's normal capsular volume or to plicate a redundant capsule in a hip with hyperlaxity preoperatively. We present our preferred technique for arthroscopic capsular repair.
Over the past decade, significant advances have been made in the recognition and treatment of femoroacetabular impingement (FAI). Acetabular rim resection, labral debridement and repair, and femoral neck osteoplasty are now commonly performed arthroscopically for well-accepted surgical indications. The role of capsular repair in arthroscopic procedures, however, is less well defined.
Hip arthroscopy, unlike arthroscopy of other joints, requires a capsulotomy to allow visualization and to increase maneuverability of instruments within the central compartment. Commonly, an interportal capsulotomy is performed. Surgeons may also create a descending capsulotomy limb along the femoral neck (creating a T-capsulotomy) to increase visualization in the peripheral compartment for the treatment of distal cam lesions. Because the descending limb of the capsulotomy may disrupt the zona orbicularis, a structure important to hip stability, it is commonly repaired. Debate exists, however, about whether the interportal segment of a T-capsulotomy or an isolated interportal capsulotomy requires repair.
The proposed advantage of capsular repair is increased hip stability, which may decrease the risk of postoperative hip dislocation or painful microinstability. The disadvantages, however, include the risk of constraining the hip by over-tightening the capsule,1 increased operating room time,1 and increased cost. There is little evidence available to guide surgeons' decisions regarding capsular repair. Our preference is to perform repair in patients who we believe are at risk for postoperative instability, including young and/or female patients, patients who have generalized or hip-specific hyperlaxity, patients who have radiographic features of dysplasia, or patients whose hips distract easily intraoperatively. In patients with osteoarthritis, we prefer not to perform repairs because release of a contracted capsule may have a therapeutic benefit. The accompanying video presentation (Video 1) shows our preferred technique for arthroscopic capsular repair in the hip.
Surgical Technique
Hip arthroscopy for FAI is performed in the usual fashion. Our preference is to use supine positioning and anterolateral and mid-anterior portals as our viewing and working portals, respectively, for the majority of the procedure. We initially perform a transverse interportal capsulotomy to allow us to work within the central compartment; we convert this into a T-capsulotomy when the cam lesion extends distally. Extensive capsulectomies are not performed, particularly when a capsular repair is planned.
Once the acetabular rim resection, labral debridement and/or repair, and femoral neck osteoplasty have been completed, a capsular repair can be performed. If a T-capsulotomy has been used, the descending limb of the capsulotomy is repaired first, proceeding from distal to proximal, and then the transverse component is repaired, proceeding from medial to lateral. We find that usually between 2 and 4 sutures in each of the descending and transverse components of the capsulotomy are necessary to obtain adequate apposition of the capsular edges and to lend sufficient strength to the repair.
Capsular repair is performed with the hip in an extended position with neutral rotation. This brings the capsular edges into a nearly apposed position but lessens the risk of over-tightening the capsule, which may occur if the repair is performed in an internally rotated position. We then begin by establishing visualization superficial to the capsular layer using both a hip-specific shaver (Stryker, San Jose, CA) and an ArthroCare 50° radiofrequency wand (Austin, TX) (Fig 1). This will permit visualization during suture placement and knot tying. Next, a partially threaded, 8.25 × 11–cm cannula (Arthrex, Naples, FL) is inserted over a switching stick through the mid-anterior portal to allow for easier exchange of instruments and to eliminate the potential for formation of a soft-tissue bridge between the limbs of the suture.
Fig 1.
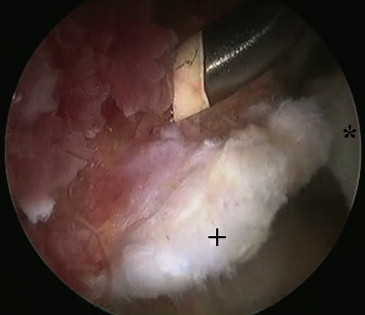
(A) Arthroscopic view of right hip through anterolateral portal. The ArthroCare wand is being used superficial to the capsule to increase visualization. (Asterisk, distal capsule; plus sign, proximal capsule.)
Creating a stitch in the capsule begins by first passing a Crescent SutureLasso (Arthrex) loaded with a No. 2 FiberStick (Arthrex) through the cannula and through the medial capsular tissue (for repair of the descending capsulotomy) or through the distal capsular tissue (for repair of the transverse capsulotomy) (Fig 2A). The stitch is placed approximately 2 to 3 mm back from the capsular edge, although this distance can be increased based on a preoperative assessment of the patient's capsular laxity and a need to tighten the capsule by plication. The camera is used to pinch the FiberStick against the femoral neck to secure the suture and prevent accidental pullout while the Crescent is removed. A KingFisher suture grasper (Arthrex) is then used through the cannula to retrieve the suture end. This completes half of the capsular stitch.
Fig 2.
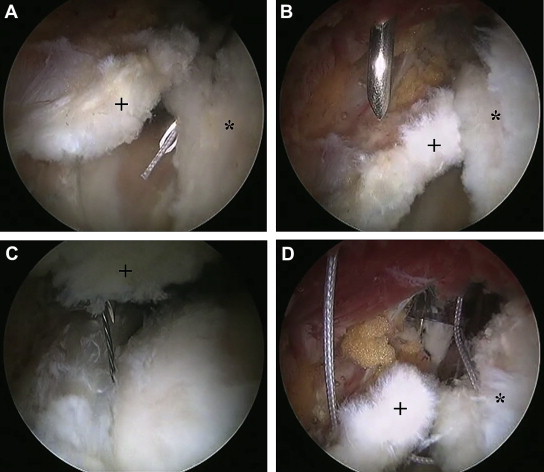
Arthroscopic view of right hip through anterolateral portal. (A) A Crescent SutureLasso loaded with No. 2 FiberStick is being passed through the distal capsular tissue for repair of the interportal capsulotomy. (B) A large-bore spinal needle has been passed percutaneously into the hip and will pierce the proximal capsule directly across from the FiberStick suture already placed in the distal capsule. (C) A nitinol wire loop is advanced through the spinal needle. (D) The wire loop is used to shuttle the FiberStick suture through the proximal capsule. (Asterisk, distal capsule; plus sign, proximal capsule.)
The second half of the capsular stitch is created by passing a large-bore spinal needle (14 gauge × 7 inches; Arthrex), loaded with a nitinol wire loop (Arthrex), through the skin and through either the lateral or the proximal capsule by means of a direct anterior approach to the hip. The spinal needle should pass through the capsule directly across from the previously placed FiberStick suture and, again, should be approximately 2 to 3 mm back from the capsular edge (Fig 2B). The wire loop is advanced (Fig 2C) and the needle is removed. A suture retriever (Arthrex) is used to retrieve the wire loop out through the cannula, and the FiberStick suture is then shuttled through the capsule and out through the skin (Fig 2D). Lastly, the suture retriever is again used through the cannula to retrieve the working end of the FiberStick. At this point, the FiberStick suture has been passed through both edges of the capsule, and both ends of the FiberStick exit the hip joint through the cannula. The suture is then tied with alternating half-hitches or an arthroscopic sliding knot (Fig 3). Additional capsular stitches are placed by the same technique. Although we used No. 2 FiberStick in the accompanying video presentation and the previous description, we have recently switched to No. 1 Vicryl (Ethicon, Cincinnati, OH), in favor of a dissolvable suture. The key points of arthroscopic capsular repair are reviewed in Table 1.
Fig 3.

Arthroscopic view of right hip through anterolateral portal. One stitch has been completed in the capsule. A total of 2 to 4 stitches are placed in the interportal portion of the capsulotomy. (Asterisk, distal capsule; plus sign, proximal capsule.)
Table 1.
Key Points of Arthroscopic Capsular Repair
| Capsular repair is performed with the leg in an extended position with neutral rotation. The descending limb of the T-capsulotomy is repaired first, followed by the interportal portion. Visualization is created above the capsular layer using a shaver and/or an ArthroCare wand. A Crescent SutureLasso is used to pass a suture through the medial or distal limb of the capsulotomy. A spinal needle is used to percutaneously pass a nitinol wire loop through the lateral or proximal limb of the capsulotomy. This is used to shuttle the suture through the capsule. Both ends of the suture are brought out of the hip joint through a cannula to prevent possible formation of a soft-tissue bridge. Alternating half-hitches or an arthroscopic knot can be used to tie the suture. Two to 4 stitches are placed in the descending limb of the capsulotomy and another 2 to 4 stitches in the interportal portion. |
Discussion
The role of capsular repair in the arthroscopic treatment of FAI is poorly defined, and there is little clinical evidence to directly guide surgeon decision making. Advocates of capsular repair emphasize the importance of the hip capsule in joint stability, and their viewpoint is supported by biomechanical studies that confirm increased external rotation and anterior translation of the femoral head after capsular sectioning2 and by clinical studies in arthroplasty that show the importance of capsular repair in reducing the postoperative dislocation rate when a posterior approach is used.3 Although hip subluxation and dislocation are infrequent after hip arthroscopy, case reports do exist describing this complication.4-6 There are also growing concerns that postoperative microinstability due to capsular laxity or deficiency may detrimentally affect patient outcomes.7 To avoid these complications, some surgeons choose to perform capsular repairs.
Capsular repair, however, does have inherent risks and disadvantages, as previously mentioned, including the risk of constraining the hip by over-tightening the capsule1 and the disadvantages of increased operating room time1 and increased cost. We also have considered that capsular repair may increase the risk of heterotopic ossification as a result of the increased dissection we perform to improve visibility and facilitate the repair. With routine prophylaxis for heterotopic ossification in all of our arthroscopy patients, however, we have not noted this as a problem. Given the rarity of postoperative dislocations and the paucity of clinical evidence supporting capsular repair, some surgeons choose not to perform capsular repairs.
Surgeons are beginning to investigate the role of capsular repair in hip arthroscopy. Domb et al.8 recently performed a matched-pair study with 2 years' follow-up. They showed no significant differences in hip range of motion, visual analog pain scores, improvement in hip-specific scores (modified Harris Hip Score, Non-Arthritic Hip Score, and Hip Outcome Score—Activities–of–Daily Living subscale), or complications between patients who received capsular repairs and those who did not. They did find, however, that the absolute Non-Arthritic Hip Score and Hip Outcome Score—Activities–of–Daily Living subscale at final follow-up were significantly higher in the capsular repair group than in the non-repair group. Overall, this study shows that capsular repair is a safe and potentially beneficial procedure; however, the results are subject to inherent bias given that the non–capsular repair surgeries were all performed early in the study period whereas the capsular repair surgeries were performed later.
Various techniques have been described for arthroscopic capsular repair. The most frequently described technique is similar to our technique in that it uses an arthroscopic suture-passing device to pass a nitinol wire loop through the first capsular limb. In contrast, however, a penetrating suture retriever is used to retrieve the wire through the opposite capsular limb. The wire is used to shuttle a suture through both capsular limbs, and then the suture is tied.1,3,9 We previously used this technique; however, we often found that the penetrating suture retriever was difficult to pass through the thick, tough capsule and that it could leave a relatively large hole in the capsule after passage. In addition, we find that using a spinal needle through a separate insertion site allows us to approach the capsule at a more favorable working angle. Other techniques describe using a hip-specific capsular closure device (InJector II Capsule Restoration System; Pivot Medical, Sunnyvale, CA)1 or a device originally designed for use in shoulder rotator cuff repair (SpeedStitch; ArthroCare)10 to facilitate suture passage. We do not have any experience with the use of these devices in the hip and are unable to comment on their advantages or disadvantages.
In conclusion, we believe that capsular repair does have a role in the arthroscopic treatment of FAI. Currently, we perform repairs in selective patients who we believe are at risk for postoperative instability, but we acknowledge that there is little available evidence to support this approach. This article and the accompanying video have described our preferred technique for capsular repair.
Footnotes
The authors report the following potential conflict of interest or source of funding: B.A.L. receives support from Arthrex, National Institutes of Health, and VOT Solutions.
Supplementary Data
Arthroscopic technique for capsular repair after procedures to address FAI in a right hip have been completed.
References
- 1.Harris J.D., Slikker W., Gupta A.K., McCormick F.M., Nho S.J. Routine complete capsular closure during hip arthroscopy. Arthrosc Tech. 2013;2:e89–e94. doi: 10.1016/j.eats.2012.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Myers C.A., Register B.C., Lertwanich P. Role of the acetabular labrum and the iliofemoral ligament in hip stability: An in vitro biplane fluoroscopy study. Am J Sports Med. 2011;39(suppl):85S–91S. doi: 10.1177/0363546511412161. [DOI] [PubMed] [Google Scholar]
- 3.Domb B.G., Philippon M.J., Giordano B.D. Arthroscopic capsulotomy, capsular repair, and capsular plication of the hip: Relation to atraumatic instability. Arthroscopy. 2013;29:162–173. doi: 10.1016/j.arthro.2012.04.057. [DOI] [PubMed] [Google Scholar]
- 4.Ranawat A.S., McClincy M., Sekiya J.K. Anterior dislocation of the hip after arthroscopy in a patient with capsular laxity of the hip: A case report. J Bone Joint Surg Am. 2009;91:192–197. doi: 10.2106/JBJS.G.01367. [DOI] [PubMed] [Google Scholar]
- 5.Matsuda D.K. Acute iatrogenic dislocation following hip impingement arthroscopic surgery. Arthroscopy. 2009;25:400–405. doi: 10.1016/j.arthro.2008.12.011. [DOI] [PubMed] [Google Scholar]
- 6.Benali Y., Katthagen B.D. Hip subluxation as a complication of arthroscopic debridement. Arthroscopy. 2009;25:405–407. doi: 10.1016/j.arthro.2009.01.012. [DOI] [PubMed] [Google Scholar]
- 7.Shu B., Safran M.R. Hip instability: Anatomic and clinical considerations of traumatic and atraumatic instability. Clin Sports Med. 2011;30:349–367. doi: 10.1016/j.csm.2010.12.008. [DOI] [PubMed] [Google Scholar]
- 8.Domb B., Finley Z., Baise R., Botser I. Two-year outcome of arthroscopic capsular repair of the hip: A matched-pair controlled study (SS-33) Arthroscopy. 2013;29 e16 (abstr, suppl) [Google Scholar]
- 9.Mauro C.S., Voos J.E., Kelly B.T. Femoroacetabular impingement surgical techniques. Oper Tech Orthop. 2010;20:223–230. [Google Scholar]
- 10.Mei-Dan O., Young D.A. A novel technique for capsular repair and labrum refixation in hip arthroscopy using the SpeedStitch. Arthrosc Tech. 2012;1:e107–e112. doi: 10.1016/j.eats.2012.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Arthroscopic technique for capsular repair after procedures to address FAI in a right hip have been completed.