

Abstract
Prosthetic tricuspid valve is an obstacle to implant cardiac devise. Cardiac Resynchronization therapy is one of the most popular therapies for heart failure patients these days. We present this case of prosthetic tricuspid valve and left ventricular dysfunction which we overcome the problem by implanting two leads to coronary sinus branches. Patient improved in few months of follow up.
Keywords: CRT, Tricuspid Valve, Heart Failure
1. Introduction
Heart failure is prevalent and its prevalence rate is following an increasing trend (1). Cardiac Resynchronization Therapy (CRT) is beneficial for about 25% of those with left bundle branch in ECG, lower than 35% ejection fraction, and moderate to severe dyspnea on full medical therapy without correctable cause (2).
Implanting CRT includes one lead to the right ventricle, one lead to the left ventricle, and the 3rd to the right atrial appendage. We implant LV lead routinely via the coronary sinus. LV access in open-heart surgery is another option. Few implants from septostomy have also been reported (3). Metallic tricuspid valve is an obstacle to enter the right ventricle causing the researchers to have dilemma when implanting CRT through open-heart surgery. In this study, we present one of these patients and report our attempt to avoid open-heart surgery by implanting two LV leads from the coronary sinus (4).
2. Case Presentation
A 52 year old man with severe dyspnea on exertion came to our attention. He was unable to do his job and had difficulty in doing his grooming. The patient’s past medical history showed aortic valve replacement 20 years ago. Another valve surgery had also occurred 7 years ago during which, aortic, mitral, and tricuspid valves were replaced by metallic valves.
Echocardiography showed normal functioning prosthetic valves, but EF = 30%, EDD = 87, and ESD = 65.
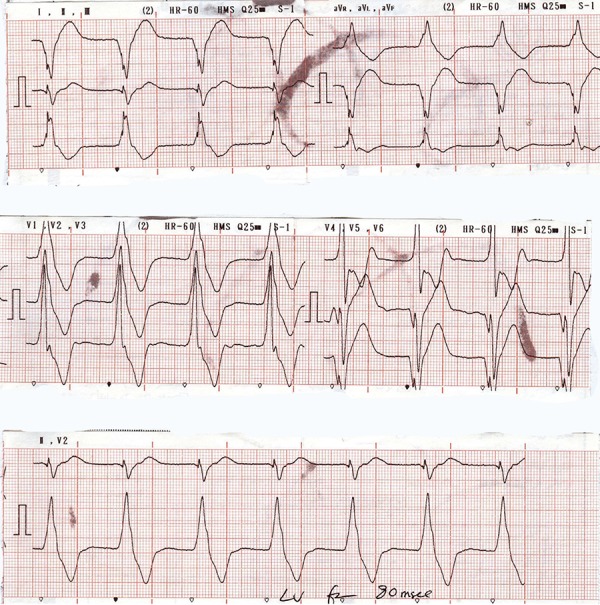
In addition, ECG revealed wide QRS and prolonged PR.
During ambulatory ECG monitoring, some brief episodes of atrial tachycardia were also noted. However, coronary angiography revealed normal findings.
The two previous valve surgeries would make the 3rd one a difficult operation due to severe adhesions; therefore, we decide to implant two LV leads from CS. After the implantation, the patient’s dyspnea improved. Then, we started Amiodarone to prevent atrial tachycardia and also increased carvediolol.
ECG and the fluoroscopic image are presented in Figures 1, 2, and 3.
Figure 1. LAO Projection Showed 3 Prosthetic Valves and Position of 2 LV Leads in the Lateral Veins.
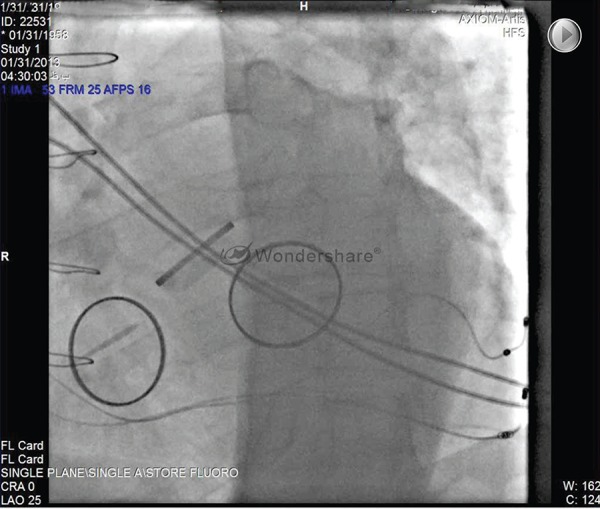
Figure 2. RAO Projection Showed Final 3 Prosthetic Valves and 3 Leads of CRT.

Figure 3. ECG after CRT Implantation.
3. Discussion
Although CRT implantation alleviate symptom and improve outcome in heart failure patients, there are some challenging cases sometimes. Implanting any device in patients with prosthetic tricuspid valve is challenging because RV. is out of reach.
Implanting leads to left ventricle epicardium from coronary sinus route is possible and promising in this group (4).
Coronary Sinus is a way to reach ventricles in patients with prosthetic Tricuspid Valve. This way permits CRT implantation in this group without hazard of open-heart surgery.
Acknowledgments
There is no acknowledgement.
Footnotes
Implication for health policy/practice/research/medical education:Endocardial lead implantation is not advised when tricuspid valve is metallic but it is possible via coronary sinus cardiac veins. This case is a patient with three metallic valvesin aortic, mitral and tricuspid positions, that due to left ventricular systolic dysfunction, two endocardial leads were implanted via coronary sinus for him.
Authors’ Contribution: Doing the case and providing the clips: Mohammad Vahid Jorat, preparing the first draft:Amir Aslani, final draft and edition: Mohammad Hossein Nikoo.
Financial Disclosure: We have no conflict of interest.
Funding/Support: There is no funding and support.
References
- 1.Schocken DD, Benjamin EJ, Fonarow GC, Krumholz HM, Levy D, Mensah GA, et al. Prevention of heart failure: a scientific statement from the American Heart Association Councils on Epidemiology and Prevention, Clinical Cardiology, Cardiovascular Nursing, and High Blood Pressure Research; Quality of Care and Outcomes Research Interdisciplinary Working Group; and Functional Genomics and Translational Biology Interdisciplinary Working Group. Circulation. 2008;117(19):2544–65. doi: 10.1161/CIRCULATIONAHA.107.188965. [DOI] [PubMed] [Google Scholar]
- 2.Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS, Ganiats TG, et al. 2009 focused update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119(14):1977–2016. doi: 10.1161/CIRCULATIONAHA.109.192064. [DOI] [PubMed] [Google Scholar]
- 3.Leclercq F, Hager FX, Macia JC, Mariottini CJ, Pasquie JL, Grolleau R. Left ventricular lead insertion using a modified transseptal catheterization technique: A totally endocardial approach for permanent biventricular pacing in end-stage heart failure. Pacing Clin Electrophysiol. 1999;22(11):1570–5. doi: 10.1111/j.1540-8159.1999.tb00374.x. [DOI] [PubMed] [Google Scholar]
- 4.Bai Y, Strathmore N, Mond H, Grigg L, Hunt D. Permanent ventricular pacing via the great cardiac vein. Pacing Clin Electrophysiol. 1994;17(4 Pt 1):678–83. doi: 10.1111/j.1540-8159.1994.tb02403.x. [DOI] [PubMed] [Google Scholar]