

Summary
A 12-year-old girl presented with an acute confusional state and a 2-year history of weight loss, anxiety, agitation and recurrent fever. Thyroid function tests confirmed severe hyperthyroidism, and a diagnosis of thyroid storm was made (Burch and Wartofsky score=75). ECG showed a prolonged QTc interval of 506 ms. Acute treatment for thyroid storm consisted of Lugol's iodine, prednisolone, carbimazole and propranolol. She made a steady recovery and by 3 months her thyroid function had normalised; a repeat ECG showed a QTc within the normal range (430 ms). There was no relevant family history. This is a case of QTc prolongation with hyperthyroidism and normalisation with euthyroidism. It is not commonly recognised that hyperthyroidism in children may be associated with QTc prolongation. QTc measurement should be incorporated into management protocols for hyperthyroidism.
Background
Prolongation of the QT interval is associated with a risk of sudden cardiac death, whether it is acquired or inherited.1–3 Acquired causes include medications, toxins, electrolyte imbalance, subarachnoid haemorrhage, myocardial ischaemia, autonomic neuropathy and HIV infection.4 5 The association of hyperthyroidism and prolonged QTc has not been previously reported in children. Hyperthyroidism in children is not uncommon, and children are commonly treated with medications that prolong the QT interval such as antihistamines. Assessment of QTc in hyperthyroid children may be important so that medications that could further prolong QT and increase cardiac risk may be avoided, and protective medication be considered.
Case presentation
A 12-year-old girl presented with a 2 year history of weight loss, jitteriness and anxiety, and a 2 month history of episodic confusion, vomiting and fever. She was tachycardic, febrile (40°C), confused and agitated. She had a fine tremor, hyper-reflexia, marked proximal muscle weakness and a goitre with bruit and a flow murmur at the left lower sternal edge. Investigations showed free T4 87 pmol/L (normal: 10–20), FT3 18.2 pmol/L (3.7–7.7), thyroid-stimulating hormone (TSH) <0.01 mU/L (0.3–4.0) and thyroid-stimulating immunoglobulin 14 U/L (normal <1). ECG taken while afebrile showed sinus tachycardia 120 bpm, PR 150 ms, QT 358 ms, RR 500 ms, QTc 506 ms (Bazett's formula), T wave morphology was abnormally broad with slow upstroke (figure 1). Potassium (3.7 mmol/L), magnesium (0.74 mmol/L) and calcium (2.18 mmol/L) were within normal range. Echocardiography demonstrated a structurally normal heart with normal function. Her Burch and Wartofsky score was 75, highly suggestive of thyroid storm.6 She was treated with Lugol's iodine, carbimazole and propranolol but the episodes of fever did not cease until prednisolone was started on day 3. On day 3 QTc remained prolonged at 491 ms with a heart rate of 70 bpm (figure 2). There was no family history of sudden unexplained death and both parents had normal ECGs including QTc. A decision was made to remain on propranolol and to avoid QTc prolonging drugs and grapefruit juice, with serial ECGs for QT assessment over time.
Figure 1.

ECGs at presentation and at 6 and 12 weeks of follow-up. QTc was calculated using Bazett's formula.
Figure 2.
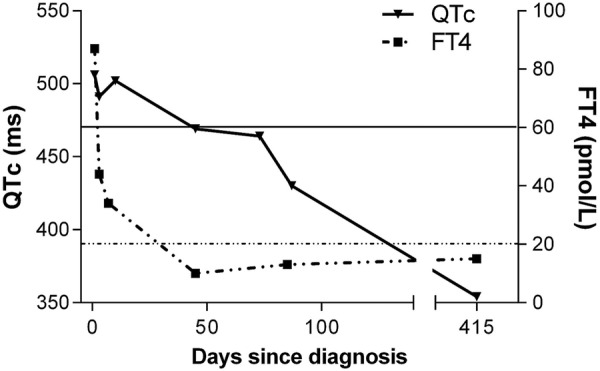
Corrected QT interval and serum-free T4 at diagnosis and following treatment of severe hyperthyroidism. Horizontal lines represent upper limits of normal for QTc (470 ms) and FT4 (20 pmol/L).
Investigations
ECG traces are provided at presentation, 6-week follow-up and 3-month follow-up, and a graph of free T4 versus QTc.
Differential diagnosis
▸ QTc prolongation secondary to hyperthyroidism.
▸ Primary channelopathy/long QT syndrome.
Outcome and follow-up
At 6 weeks postdischarge, the patient had normal levels of free T4 (10 pmol/L) and T3 (4.2 pmol/L); QTc was 469 ms. By 3 months postdischarge, she had been euthyroid for 8 weeks; QTc was 430 ms and there was normalisation of T wave morphology (figures 1 and 2). Propranolol was ceased. Twelve months after the event, she was euthyroid (FT4 15 pmol/L, T3 5.1 pmol/L, TSH 3.6 mU/L) and was assessed by exercise ECG. QTc was 354 ms at rest (figure 2), 377 ms at peak heart rate and 444 ms after 7 min of recovery. Thus there was no evidence of a persisting underlying long QT syndrome.
Discussion
This case is of a young girl with severe hyperthyroidism due to Grave's disease, and associated prolongation of the QT interval. Importantly, the QTc normalised with resolution of hyperthyroidism (figure 2). While this association has not been reported in children, there is evidence of an association in adults.
In addition to the well-known effects of T3 on cardiac rate and contractility, thyroid hormone is also known to effect ventricular repolarisation.7 Hypothyroidism is classically associated with prolonged QTc,8 but paradoxically, hyperthyroidism can also lead to QT prolongation. In adults with hyperthyroidism, QTc is prolonged compared with controls and normalises with treatment of hyperthyroidism, furthermore QTc is positively correlated with both serum FT3 and FT4.9 Those with subclinical hyperthyroidism have longer QTc than controls10 and within the normal male population QTc is correlated with FT4.11 The clinical importance of this effect is suggested by a population-based study in adults which found that the use of antithyroid drugs was associated with sudden cardiac death; the authors proposed that this was due to undertreated hyperthyroidism.12 Further, in a recent report of a 13-year-old girl with severe hyperthyroidism, severe QTc prolongation was documented immediately prior to the development of torsade de pointes and cardiac arrest.13
The mechanism by which hyperthyroidism causes prolongation of ventricular repolarisation remains unclear. Thyroid hormone excess may cause hyperpolarisation and prolongation of QTc by increasing the activity of Na+/K+ATPase.14 Alternatively ventricular repolarisation could be effected by modulation of cardiac mitochondrial function by thyroid hormone.15 16
Our unit has considerable experience with the diagnosis and management of long QT syndrome in children.17 With physiological or drug-induced QT prolongation, it is important to consider whether an underlying genetic predisposition is present. We can be confident this is not the case because of the normalisation of QTc with disease resolution, normal QT response post exercise, absence of family history and normal ECGs in the parents. Genetic testing in these circumstances is not appropriate.
A relationship between hyperthyroidism and QTc prolongation is clinically important. Hyperthyroidism in children is not uncommon, and patients are commonly treated with medications that prolong the QT interval, such as antihistamines. Assessment of QTc in children with hyperthyroidism is important so that QT prolonging medications may be avoided, and protective medication considered. The relationship between hyperthyroidism and QTc should be assessed prospectively to allow better estimation of the strength of association and frequency of significant prolongation.
Learning points.
Children with hyperthyroidism are at risk of QT prolongation.
Serial ECGs should be performed and QT prolonging medication avoided until the QT interval has normalised.
Conversely, in children with QT prolongation, hyperthyroidism should be considered.
Acknowledgments
The authors thank Miss SN and her family who kindly gave permission for this case report.
Footnotes
Contributors: BBA and LGE contributed equally as first authors of this case report. All authors were involved in the clinical care of this patient and in writing the manuscript.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Goldenberg I, Moss AJ. Long QT syndrome. J Am Coll Cardiol 2008;51:2291–300 [DOI] [PubMed] [Google Scholar]
- 2.Khan IA. Clinical and therapeutic aspects of congenital and acquired long QT syndrome. Am J Med 2002;112:58–66 [DOI] [PubMed] [Google Scholar]
- 3.Yap YG, Camm AJ. Drug induced QT prolongation and torsades de pointes. Heart 2003;89:1363–72 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Roden DM. Drug-induced prolongation of the QT Interval. N Engl J Med 2004;350:1013–22 [DOI] [PubMed] [Google Scholar]
- 5.Al-Khatib SM, LaPointe NMA, Kramer JM, et al. What clinicians should know about the QT interval. JAMA 2003;289:2120–7 [DOI] [PubMed] [Google Scholar]
- 6.Burch HB, Wartofsky L. Life-threatening thyrotoxicosis. Thyroid storm. Endocrinol Metab Clin North Am 1993;22:263. [PubMed] [Google Scholar]
- 7.Polikar R, Burger AG, Scherrer U, et al. The thyroid and the heart. Circulation 1993;87:1435–41 [DOI] [PubMed] [Google Scholar]
- 8.Fazio S, Biondi B, Lupoli G, et al. Evaluation, by noninvasive methods, of the effects of acute loss of thyroid hormones on the heart. Angiology 1992;43:287–93 [DOI] [PubMed] [Google Scholar]
- 9. doi: 10.1046/j.1365-2265.2001.01295.x. Colzani RM, Emdin M, Conforti F, et al. Hyperthyroidism is associated with lengthening of ventricular repolarization. Clin Endocrinol 2001;55:27–32. [DOI] [PubMed] [Google Scholar]
- 10.Galetta F, Franzoni F, Fallahi P, et al. Changes in autonomic regulation and ventricular repolarization induced by subclinical hyperthyroidism. Biomed Pharmacother 2010;64:546–9 [DOI] [PubMed] [Google Scholar]
- 11.van Noord C, van der Deure WM, Sturkenboom MC, et al. High free thyroxine levels are associated with QTc prolongation in males. J Endocrinol 2008;198:253–60 [DOI] [PubMed] [Google Scholar]
- 12.Van Noord C, Sturkenboom MC, Straus SM, et al. Population-based studies of antithyroid drugs and sudden cardiac death. Br J Clin Pharmacol 2009;68:447–54 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kara O, Demirel F, Tepe D, et al. A case with Graves disease who developed agranulocytosis and vasculitis during metimazole treatment. Poster presented at 9th Joint Meeting of Paediatric Endocrinology Milan, 2013 [Google Scholar]
- 14.Awais D, Shao Y, Ismail-Beigi F. Thyroid hormone regulation of myocardial Na/K-ATPase gene expression. J Mol Cell Cardiol 2000;32:1969–80 [DOI] [PubMed] [Google Scholar]
- 15.Owecki M, Michalak A, Nikisch E, et al. Prolonged ventricular repolarization measured by corrected QT interval (QTc) in subclinical hyperthyroidism. Horm Metab Res 2006;38:44–7 [DOI] [PubMed] [Google Scholar]
- 16.Venditti P, Puca A, Di Meo S. Effects of thyroid state on H2O2 production by rat heart mitochondria: sites of production with complex I- and complex II-linked substrates. Horm Metab Res 2003;35:55–61 [DOI] [PubMed] [Google Scholar]
- 17.Earle N, Crawford J, Smith W, et al. Community detection of long QT syndrome with a clinical registry: an alternative to ECG screening programs? Heart Rhythm 2013;10:233–8 [DOI] [PubMed] [Google Scholar]