

Abstract
Purpose
Forkhead box P3 (Foxp3) is known as the most specific marker for regulatory T lymphocytes, which play an important role in immune tolerance to disturb antitumor immunity. The present study aimed to investigate the prognostic significance of Foxp3 regulatory T lymphocyte (Foxp3 Treg) infiltration in breast cancer.
Methods
Immunohistochemical studies with Foxp3, CD4, and CD8 were performed on representative full tissue sections from 143 patients with invasive ductal carcinoma, not otherwise specified. Foxp3 Treg infiltration and the ratios between Foxp3 Treg and CD4 or CD8 T cells were separately analyzed for the tumor bed and tumor periphery to evaluate their association with different clinicopathological parameters and patients' outcome.
Results
The tumor periphery was considerably more densely infiltrated by Foxp3 Treg, CD4, and CD8 T cells than the tumor bed. Unfavorable clinicopathological parameters (a Ki-67 labeling index of ≥14%, a worse histologic grade, a worse nuclear grade, hormone receptor negativity, human epidermal growth factor receptor 2 positivity, and tumor recurrence) were associated with increased Foxp3 Treg infiltration and a high ratio between Foxp3 Treg and CD4/CD8 T cells. In the tumor periphery, as Foxp3 Treg infiltration and the Foxp3 Treg/CD8 ratio increased, patients' 5-year disease-free survival rate decreased.
Conclusion
The infiltration densities of Foxp3 Treg, CD4, and CD8 T cells were markedly different between the tumor bed and periphery. Besides the absolute count of Foxp3 Treg, the ratio between Foxp3 Treg and effector T cells was a significant prognostic factor in breast cancer.
Keywords: Breast neoplasms, Foxp3 protein, Humans, T-lymphocyte, Regulatory
INTRODUCTION
Regulatory T lymphocytes (Treg), comprising a subpopulation of CD4 T lymphocytes, mediate peripheral tolerance by suppressing self-antigen reactive T cells [1,2]. Since most tumor antigens are self-antigens [2], the suppression of tumor antigen reactive T lymphocytes by Treg is an important obstacle in antitumor immunity [3]. The transcription factor forkhead box P3 (Foxp3) which plays an important role in the development and function of CD4/CD25 Treg, is known as the most specific marker of Treg and has been previously utilized for Treg quantification [4,5,6].
Foxp3 regulatory T lymphocytes (Foxp3 Treg) suppress various immune cells, including CD4 and CD8 T lymphocytes, dendritic cells, B cells, and macrophages [7], via multiple mechanisms. First, Foxp3 Treg can inhibit effector T cells via the secretion of inhibitory cytokines, such as interleukin (IL)-10 or tumor growth factor 1β (TGF-1β). Second, a high level of CD25 (IL-2 receptor α chain) expression in Foxp3 Treg can result in the competitive consumption of IL-2 by Foxp3-negative T cells, which subsequently inhibits the proliferation of effector T cells. Finally, Foxp3 Treg can directly eliminate effector T cells through the perforin- and granzyme-dependent pathways [7,8,9,10,11]. Furthermore, increased Foxp3 Treg infiltration has been known to be associated with unfavorable outcomes and various poor prognostic factors in many cancers [12,13,14,15,16,17].
Previous studies have shown that the infiltration pattern of tumor-infiltrating lymphocytes (TIL) differs between the tumor bed and its surrounding tissues. Additionally, both the infiltration pattern and the TIL population have been shown to influence tumor prognosis [13,18,19]. However, to date, few studies have investigated the zonal difference of Foxp3 Treg infiltration in breast cancer. Since Foxp3 Treg interacts with various target cells, an assessment of the relative proportion between Foxp3 Treg and its target cells is considered more reliable than that of Foxp3 Treg alone. This study therefore aimed to investigate Foxp3 Treg infiltration and the relative ratio between Foxp3 Treg and CD4 or CD8 T lymphocytes in the tumor bed and tumor periphery, respectively, and to assess the association of these factors with clinicopathological parameters, biologic subtypes, and prognosis in breast cancer.
METHODS
Patient selection
The present study included 143 patients who had been diagnosed with invasive ductal carcinoma, not otherwise specified, and undergone surgical excision at Ewha Womans University Mokdong Hospital between January 2003 and December 2007. Patients who received preoperative hormonal therapy or neoadjuvant chemotherapy were excluded. Cases in which the tumor size was less than 0.5 cm or the proportion of ductal carcinoma in situ was more than 50% were also excluded. All hematoxylin-and-eosin-stained slides for each case were retrospectively reviewed, and the most representative tumor block was selected. Histological grade was assessed using the Nottingham grading system [20]. Clinicopathological parameters evaluated for each breast cancer patient included the patient's age at his/her initial diagnosis, tumor size, lymph node metastasis, histologic grade, nuclear grade, estrogen receptor (ER) and progesterone receptor (PR) status, human epidermal growth factor receptor 2 (HER2) status, tumor recurrence, distant metastasis, and survival. The median follow-up duration after surgery was 69 months. This study was approved by the Institutional Review Board of Ewha Womans University Mokdong Hospital (IRB approval number, 14-05-06).
Immunohistochemistry
Immunohistochemistry (IHC) was performed on representative full tissue sections of formalin-fixed paraffin-embedded tumor blocks using monoclonal antibodies against Foxp3 (clone 236A/E7, dilution 1:200; Abcam, Cambridge, UK), CD4 (clone 4B12, dilution 1:60; Novocastra, Newcastle, UK), and CD8 (clone 4B11, dilution 1:80; Novocastra). Staining procedure was conducted using a Leica-BOND III automated IHC system (Leica Microsystems, Wetzlar, Germany) according to a modified manufacturer protocol. The Bond Polymer Refine Detection Kit (Leica Microsystems) was used following antigen retrieval with Solution 1 (Leica Microsystems). Briefly, tissue sections on adhesive glass slides were deparaffinized, hydrated in serially diluted alcohol, and immersed in 3% hydrogen peroxide to remove endogenous peroxidase activity. Sections were subsequently processed in EDTA buffer (pH 9.0) for CD4 or CD8, and citrate buffer (pH 6.0) for Foxp3 for 15 minutes in the microwave for antigen retrieval. After incubation with the primary antibodies, immuno-detection was performed according to the manufacturer's guidelines. We used 3'-diaminobenzidine chromogen as the substrate. The primary antibody incubation step was omitted in the negative control. Slides were counterstained with Mayer's hematoxylin.
Quantification of Foxp3 Treg, CD4 T cells, and CD8 T cells
Foxp3 Treg, CD4, and CD8 T lymphocyte infiltration were separately quantified for the tumor bed and tumor periphery. The tumor periphery was defined as the area within a 400× high power field (HPF) from the outline of the tumor. Tumor bed was defined as the area at least one 400× HPF apart from the tumor outline toward center of the tumor. Treg, CD4, and CD8 T cells were manually counted in 5 HPFs with the densest infiltration within the tumor bed and tumor periphery, respectively. The average number of cells was then calculated from such counts. The ratios of Foxp3 Treg to CD4 or CD8 T cells in the tumor bed and tumor periphery were also separately calculated. Nuclear or cytoplasmic staining for Foxp3 by tumor cells was neglected.
Biologic subtype classification
In this study, breast cancer was classified into four biologic subtypes based on IHC profiles of ER/PR and HER2. A cutoff value of >1% positively stained nuclei was used to define ER and PR positivity [21]. IHC staining for HER2 was evaluated according to the American Society of Clinical Oncology/College of American Pathologists guidelines, using the following categories: 0, no staining; 1+, weak, incomplete membranous staining (<10% of tumor cells); 2+, complete membranous staining, either uniform or weak (≥10% of tumor cells); and 3+, uniform intense membranous staining (≥30% of tumor cells) [22]. A sample was considered HER2-positive when intense membranous staining (3+) was observed. IHC result for Ki-67 was determined by the percentage of tumor cells with positively stained nuclei. According to the above criteria, all breast cancers were classified as follows [23]: luminal A type: ER and/or PR positive, HER2 negative, and Ki-67 labeling index (LI) <14%; HER2-negative luminal B type: ER and/or PR positive, HER2 negative, and Ki-67 LI ≥14%; HER2-positive luminal B type: ER and/or PR positive and HER2 positive; HER2 type: ER and PR negative and HER2 positive; triple negative breast cancer (TNBC): ER, PR, and HER2 negative.
Statistical analysis
Data were processed using the SPSS for Windows version 20.0 (IBM, Armonk, USA). The Mann-Whitney U test and Kruskal-Wallis test were used to examine differences between Foxp3 Treg, Foxp3 Treg/CD4 T cells, and Foxp3 Treg/CD8 T cells according to the included clinicopathological parameters. If the Kruskal-Wallis test resulted in a p-value of <0.05, a post hoc Conover multiple comparison test was performed for pairwise comparison of subgroups. Kaplan-Meier survival curves and log-rank statistics were used to evaluate time to tumor recurrence and time to death. Multivariate regression analysis was performed using the Cox proportional hazards model. In all analyses, a p-value of <0.05 indicated statistical significance.
RESULTS
Patients' clinicopathological characteristics
The clinicopathological characteristics of the study group are shown in Table 1. The age at initial diagnosis was over 35 years in 136 patients (95.1%). The tumor size was ≤5 cm (T1 and T2) in 137 patients (95.8%), and lymph node metastasis was observed in 33 patients (23.1%). Breast cancer cases in all enrolled patients were classified into biologic subtypes, including 89 luminal A (62.2%), 21 HER2-positive luminal B (14.7%), 5 HER2-negative luminal B (3.5%), 14 HER2 type (9.8%), and 14 TNBC (9.8%).
Table 1.
Clinicopathological characteristics of the patients (n=143)
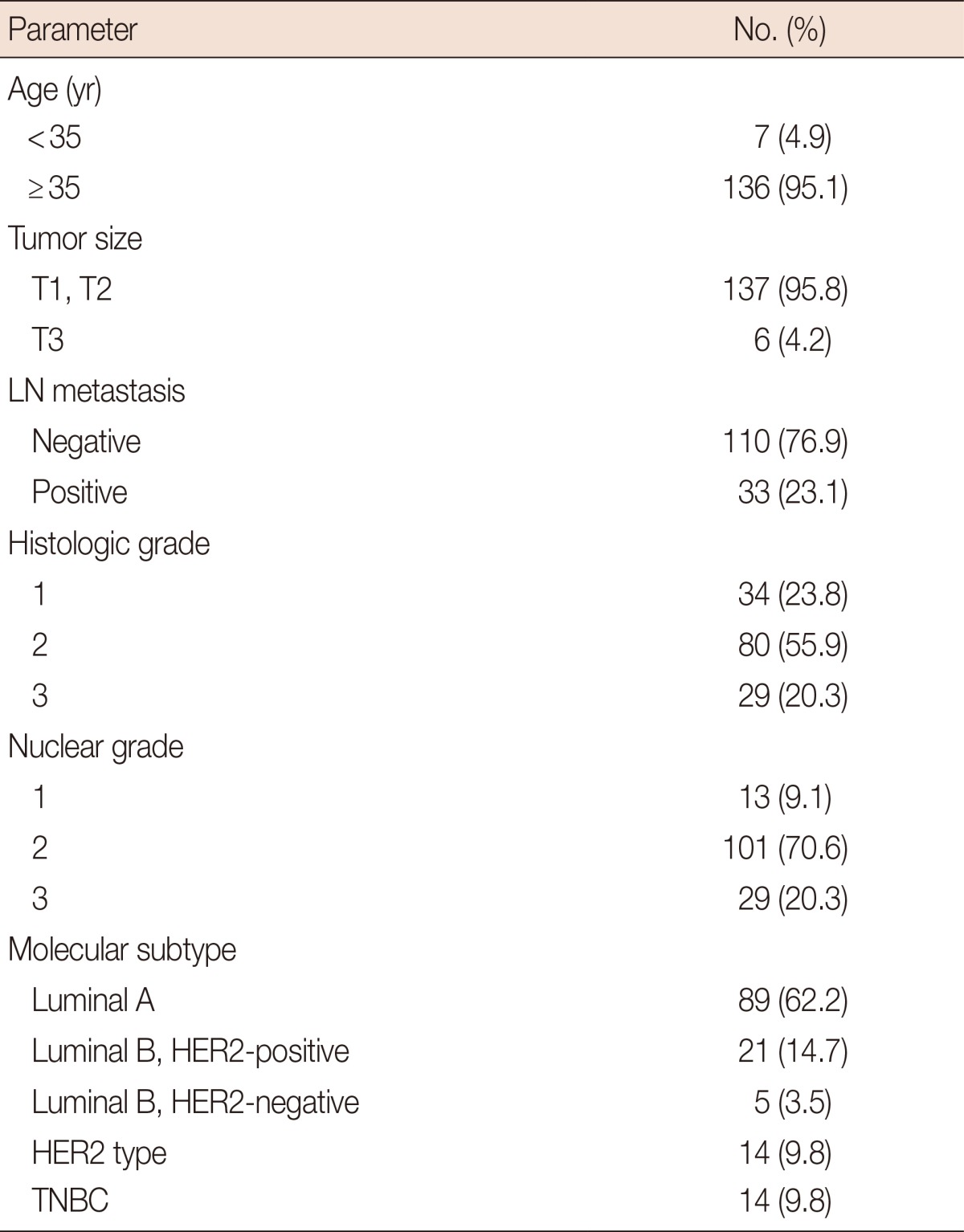
LN=lymph node; HER2=human epidermal growth factor receptor 2; TNBC=triple negative breast cancer.
Difference in Foxp3 Treg, CD4 T cell, and CD8 T cell infiltration between the tumor periphery and tumor bed
The density of Foxp3 Treg in the tumor periphery was remarkably higher than that in the tumor bed (p<0.001) (Table 2, Figure 1), with mean values of 32.0 and 19.2, respectively. CD4 and CD8 T cells, which are under the suppression of Foxp3 Treg, also showed denser infiltration in the tumor periphery than in the tumor bed (p<0.001) (Table 2, Figure 1). The ratios between Foxp3 Treg and CD4 or CD8 T cells were higher in the tumor bed than in the tumor periphery; however, the difference was not statistically significant.
Table 2.
Zonal difference of Foxp3 Treg, CD4, and CD8 T cells infiltration
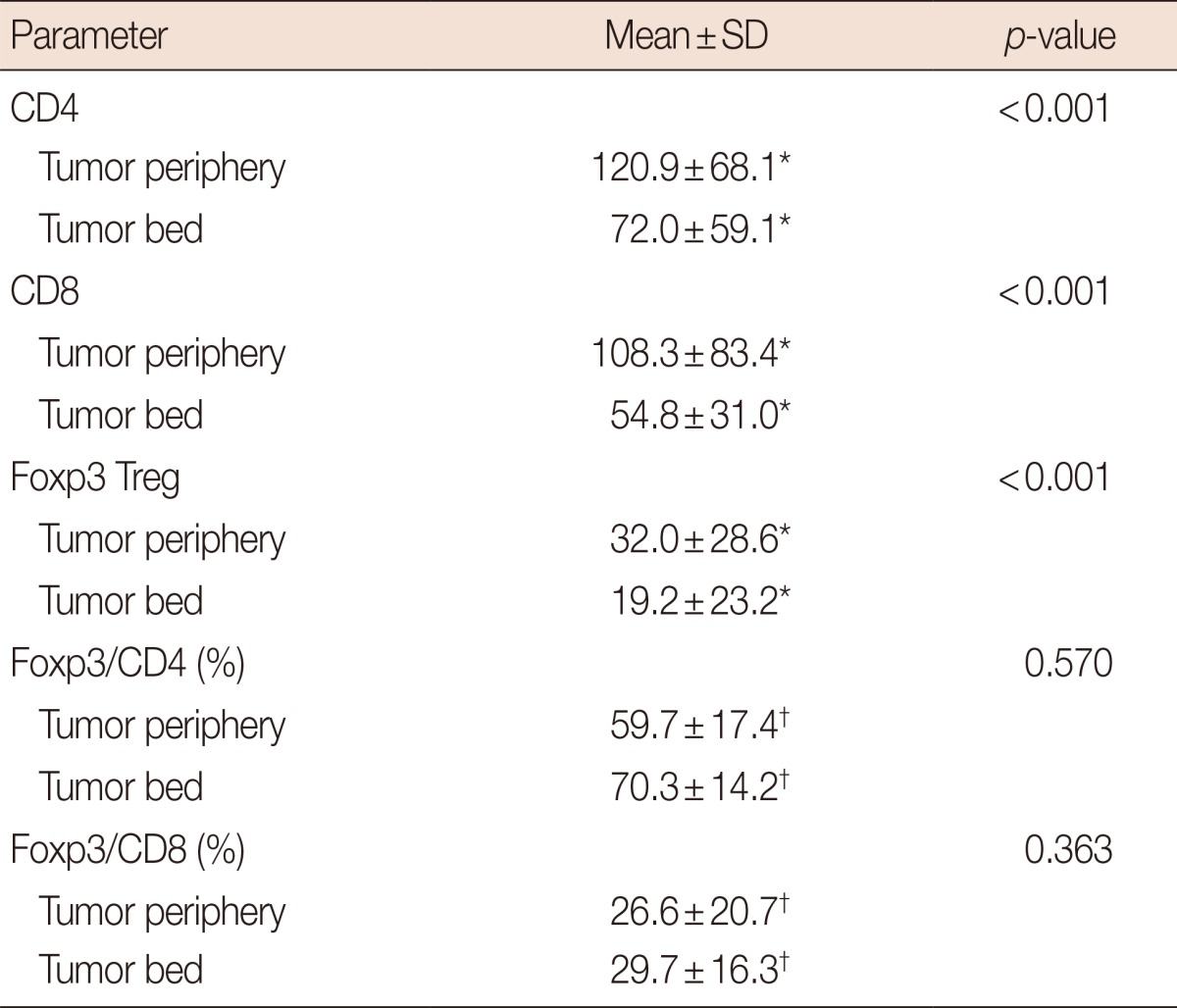
Foxp3=forkhead box P3; SD=standard deviation.
*Absolute number; †Relative ratio of Foxp3 Treg to effector T cell.
Figure 1.

immunohistochemical (IHC) staining of CD4 in tumor periphery (IHC stain for CD4, ×200) (A), CD4 in tumor bed (IHC stain for CD4, ×200) (B), CD8 in tumor periphery (IHC stain for CD8, ×200) (C), CD8 in tuomr bed (IHC stain for CD8, ×200) (D), Foxp3 in tumor periphery (IHC stain for Foxp3, ×200) (E), and Foxp3 in tumor bed (IHC stain for Foxp3, ×200) (F). Tumor periphery shows denser infiltration of CD4, and CD8 T cells, and Foxp3 Tregs than tumor bed.
Correlations between Foxp3 treg infiltration and clinicopathological parameters
Differences in the infiltration of Foxp3 Treg in the tumor periphery and tumor bed were analyzed separately according to clinicopathological parameters (Table 3). In the tumor periphery, an increased absolute count of Foxp3 Treg had a significant association with various poor prognostic factors of breast cancer, including a Ki-67 LI of ≥14% (p=0.001), a worse histologic grade (p=0.001), a worse nuclear grade (p=0.035), ER negativity (p=0.010), and PR negativity (p=0.019). Of four biologic subtypes, the densest infiltration of Foxp3 Treg was observed in the aggressive TNBC subtype. In the tumor bed, a Ki-67 LI of ≥14% (p=0.004) and a worse histologic grade (p=0.017) were significantly associated with the increased infiltration of Foxp3 Treg.
Table 3.
Correlation of clinicopathological characteristics with Foxp3 Treg infiltration
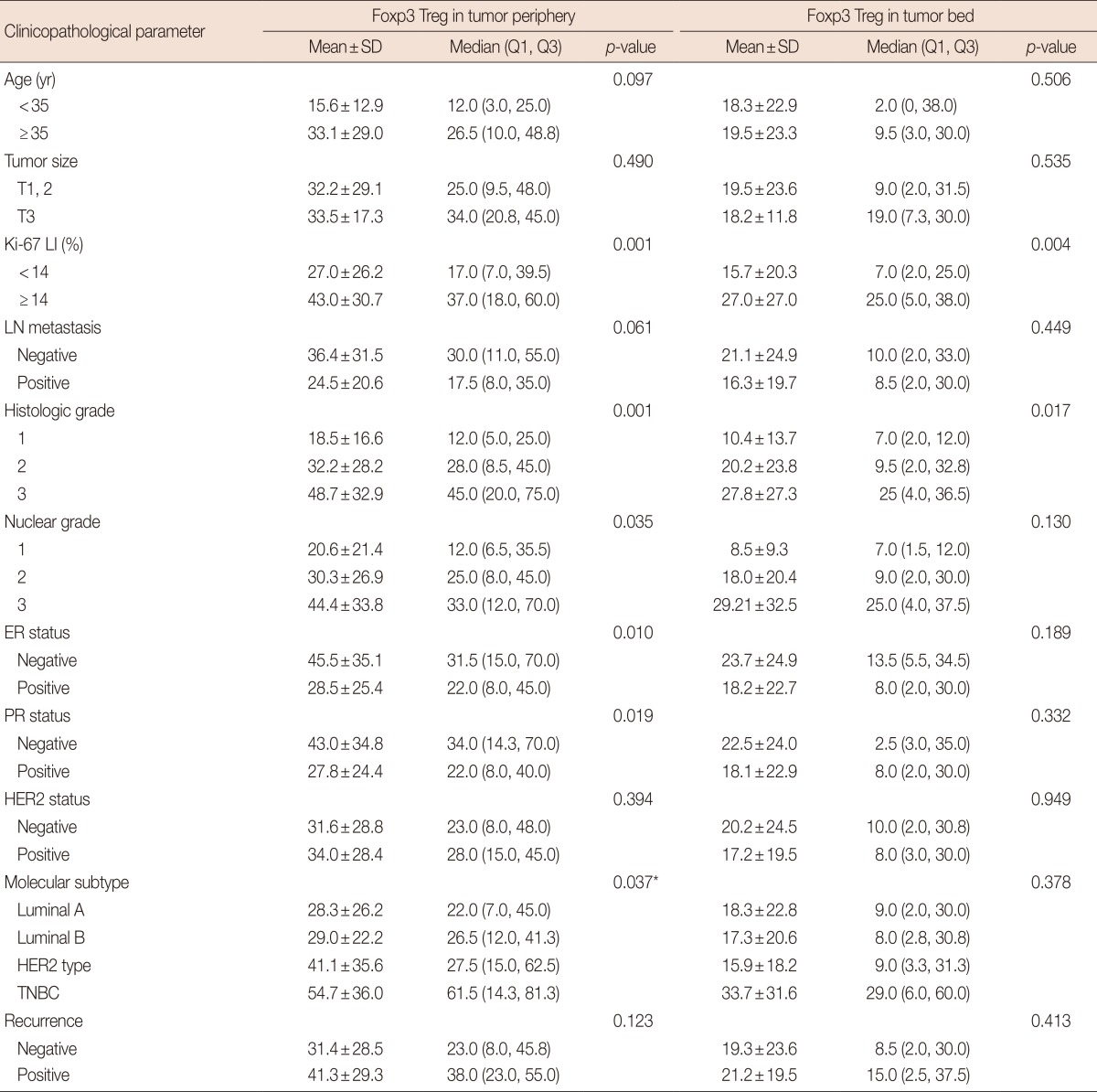
Foxp3=forkhead box P3; SD=standard deviation; Q1=25% quantile; Q3=75% quantile; Ki-67 LI=Ki-67 labeling index; LN=lymph node; ER=estrogen receptor; PR=progesterone receptor; HER2=human epidermal growth factor receptor 2; TNBC=triple negative breast cancer.
*p-value <0.05 was confirmed between luminal A-TNBC and luminal B-TNBC by the post hoc Conover test.
Correlations between the ratios of Foxp3 Treg to CD4/CD8 T cells and clinicopathological parameters
Because Foxp3 Treg disturbs antitumor immunity by suppressing the activity of effector T cells, the relative ratio between Foxp3 Treg and effector T cells was expected to be important, in addition to the absolute count of Foxp3 Treg. Table 4 shows the association between the clinicopathological parameters and the ratio of Foxp3 Treg to CD4 T cells. In the tumor periphery, poor prognostic factors, such as a Ki-67 LI of ≥14% (p=0.004), a worse histologic grade (p=0.014), HER2 positivity (p=0.006), and recurrence (p=0.014), were associated with high Foxp3 Treg/CD4 T cell ratios. Additionally, a significant difference was observed among the biologic subtypes (p=0.014). In the tumor bed, a large tumor size (p=0.021), a worse histologic grade (p=0.022), and tumor recurrence (p=0.017) were also associated with high Foxp3 Treg/CD4 T cell ratios. Differences in the ratio between Foxp3 Treg and CD8 T cells, according the included clinicopathological parameters, are shown in Table 5. Our results indicated that some poor prognostic factors were associated with high Foxp3 Treg/CD8 T cell ratios. In the tumor periphery, breast cancers with a Ki-67 LI of ≥14% (p=0.002), a worse histologic grade (p=0.001), PR negativity (p=0.023), and tumor recurrence (p=0.035) also had high Foxp3 Treg/CD8 T cell ratios. In the tumor bed, tumors with a Ki-67 LI of ≥14% (p=0.008), a worse histologic grade (p=0.002), ER negativity (p=0.044), and recurrence (p=0.048) were found to possess high Foxp3 Treg/CD8 T cell ratios. Interestingly, while the absolute count of Foxp3 Treg had no significant association with tumor recurrence, the relative ratio between Foxp3 Treg and effector T cells did.
Table 4.
Correlation of clinicopathological characteristics with Foxp3 Treg/CD4 T cell
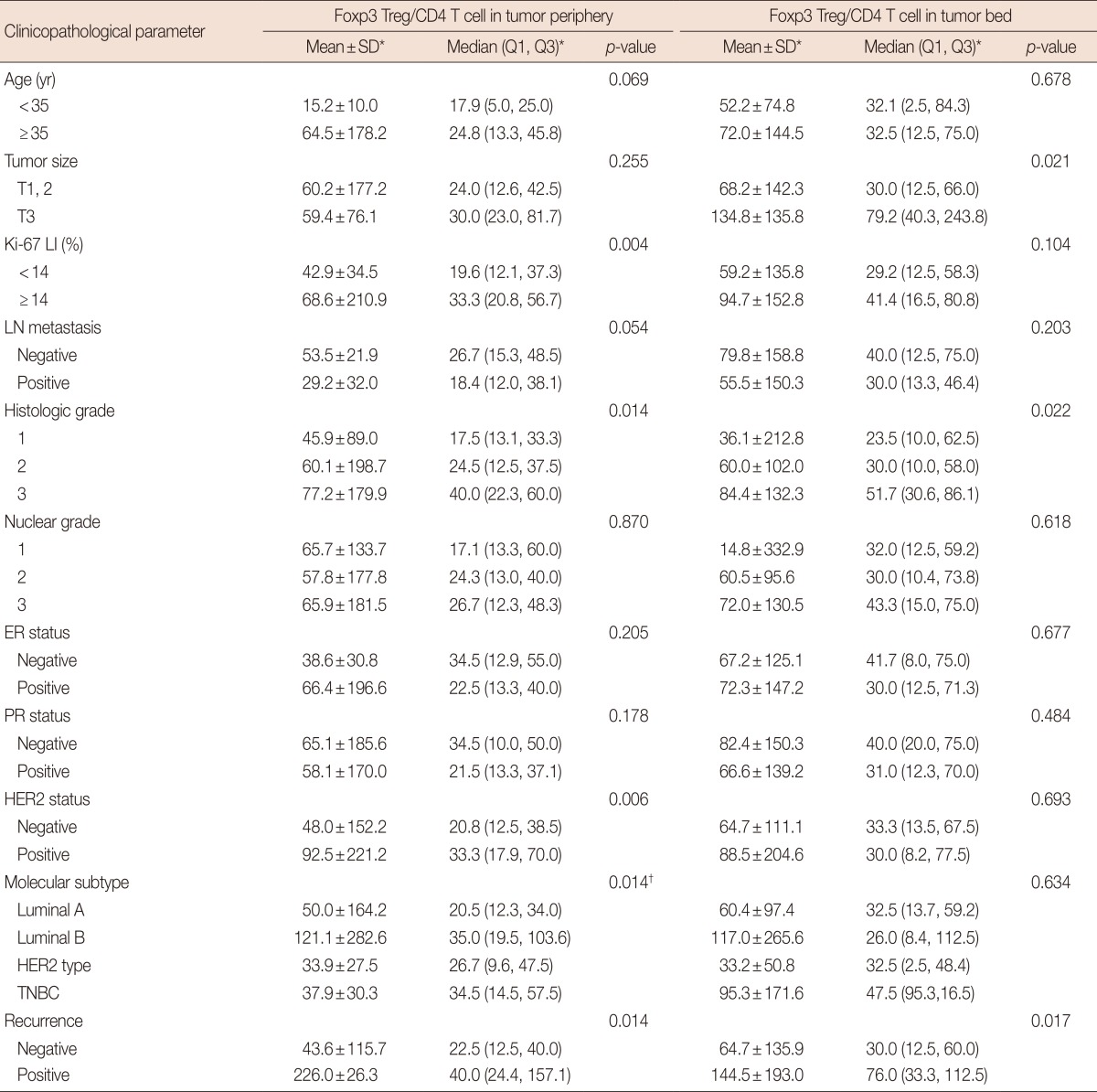
Foxp3=forkhead box P3; SD=standard deviation; Q1=25% quantile; Q3=75% quantile; Ki-67 LI=Ki-67 labeling index; LN=lymph node; ER=estrogen receptor; PR=progesterone receptor; HER2=human epidermal growth factor receptor 2; TNBC=triple negative breast cancer.
*Ratio of Foxp3 Treg to CD4 T cell; †p-value <0.05 was confirmed between luminal A-luminal B by the post hoc Conover test.
Table 5.
Correlation of clinicopathological characteristics with Foxp3 Treg/CD8 T cells
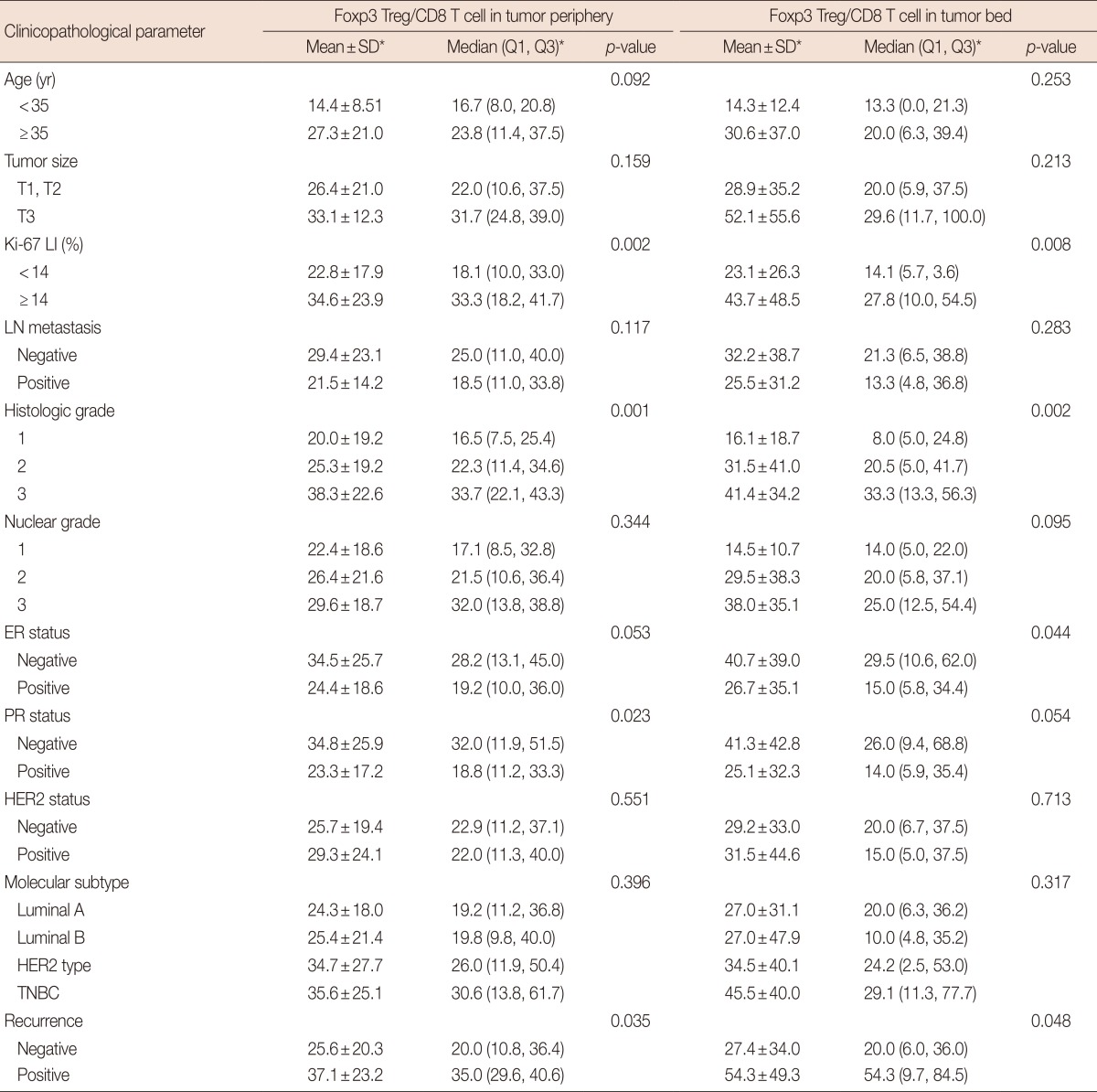
Foxp3=forkhead box P3; SD=standard deviation; Q1=25% quantile; Q3=75% quantile; Ki-67 LI=Ki-67 labeling index; LN=lymph node; ER=estrogen receptor; PR=progesterone receptor; HER2=human epidermal growth factor receptor 2; TNBC=triple negative breast cancer.
*Ratio of Foxp3 Treg to CD8 T cell.
Impact of Foxp3 Treg infiltration on patients' outcome
The absolute Foxp3 Treg count, the Foxp3 Treg/CD4 T cell ratio, and the Foxp3 Treg/CD8 T cell ratio were subclassified into high or low groups in reference to their respective median values. In the tumor periphery, univariate analysis confirmed a significant difference in the 5-year disease-free survival (DFS) rate in two of those parameters. The 5-year DFS rate was 98.5% in the low Foxp3 Treg group versus 85.7% in the high Foxp3 Treg group (p=0.042). Similarly, it was 98.5% in the low Foxp3 Treg/CD8 T cell group versus 86.2% in the high Foxp3 Treg/CD8 T cell group (p=0.012) (Table 6, Figure 2). For the tumor bed, no parameter was found to significantly influence DFS and overall survival (OS).
Table 6.
Univariate analysis of Foxp3, CD4, and CD8 T cell infiltration and disease-free survival and overall survival
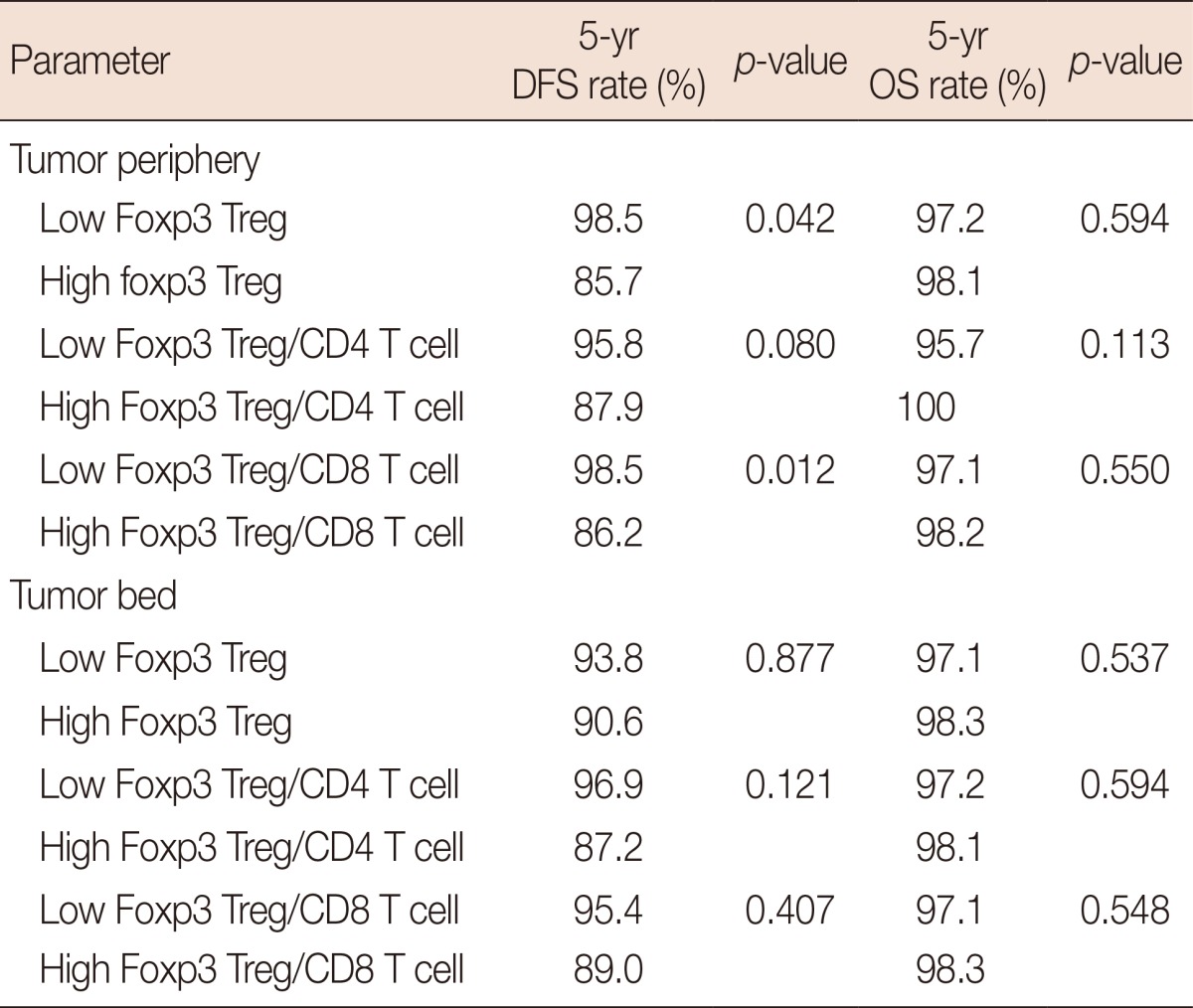
Foxp3 Treg, Foxp3 Treg/CD4 T cells, and Foxp3 Treg/CD8 T cells were subclassified as high or low groups in reference to the respective median values. Foxp3=forkhead box P3; DFS=disease-free survival; OS=overall survival.
Figure 2.

(A) Kaplan-Meier survival curve comparing the high and the low forkhead box P3 (Foxp3) T reg infiltration group in tumor periphery. The 5-year disease-free survival (DFS) rate was higher in low Foxp3 Treg group than in the high Foxp3 Treg group (p=0.042). (B) Kaplan-Meier survival curve comparing the high Foxp3 Treg/CD8 group and the low Foxp3 Treg/CD8 group in tumor periphery. The 5-year DFS rate was higher in the low Foxp3 Treg/CD8 T cell group than in the high Foxp3 Treg/CD8 T cell group (p=0.012).
Multivariate Cox analysis revealed that an advanced T stage (T1, T2 vs. T3; p=0.001; hazard ratio [HR], 8.568; 95% confidence interval [CI], 2.344-31.316), an advanced N stage (N0, N1 vs. N2, N3; p=0.013; HR, 3.981; 95% CI, 1.336-11.860), and a high Foxp3 Treg/CD8 T cell ratio (low vs. high; p=0.025; HR, 5.572; 95% CI, 1.235-25.144) were predictive factors for decreased DFS. An advanced T stage (T1, T2 vs. T3; p=0.047; HR, 11.406; 95% CI, 1.032-126.050) was the only predictive factor for shorter OS (Table 7).
Table 7.
Multivariate analysis for patient prognosis
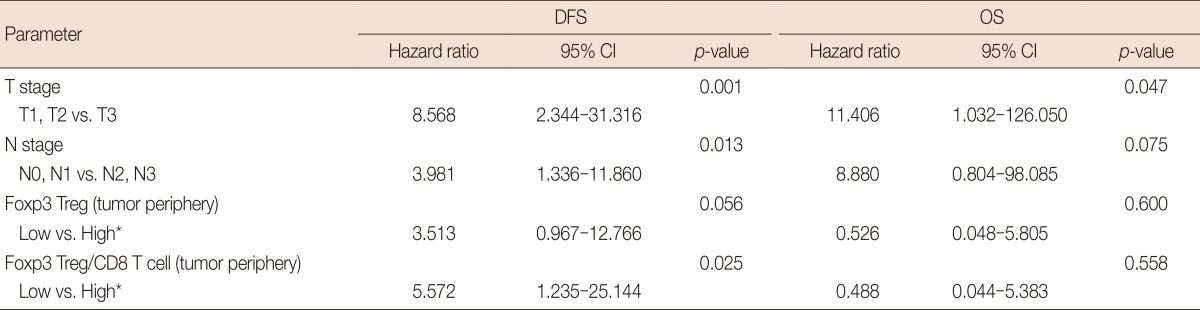
DFS=disease-free survival; OS=overall survival; CI=confidence interval; Foxp3=forkhead box P3.
*Foxp3 Treg and Foxp3 Treg/CD8 T cells were subclassified as high or low groups in reference to the respective median value.
DISCUSSION
In the present study, we investigated the infiltration of Foxp3 Treg, CD4, and CD8 T cells separately in the tumor periphery and tumor bed, and assessed its association with pathologic prognostic factors, biologic subtypes, and patients' outcome in breast cancer. Immunohistochemical studies were performed using representative full tissue sections instead of tissue microarrays, and each type of lymphocyte was manually counted on the immunostained slides. Therefore, selection bias was significantly reduced, and the difference in zonal lymphocyte infiltration could be identified with better accuracy than in studies using tissue microarrays.
The results of the current study revealed that the tumor periphery was remarkably more densely infiltrated by Foxp3 Treg, CD4, and CD8 T cells than the tumor bed. This was in accordance with previously published results reporting that infiltration by Foxp3 Treg and CD8 T cells was more abundant in the tumor's surrounding tissue than in the tumor bed [13]. Such a distinct difference in TIL density among different tumor areas highlights the importance of zonal quantification when investigating TIL.
Furthermore, Foxp3 Treg infiltration was more closely related to the unfavorable parameters and had a greater influence on DFS in the tumor periphery than in the tumor bed. These results suggest that the suppression of antitumor immunity by Foxp3 Treg in the tumor periphery (the invasive front of tumor) is very important to its biologic behaviors.
In both the tumor periphery and tumor bed, unfavorable pathological parameters (a Ki-67 LI of ≥14%, a worse histologic grade and nuclear grade, tumor recurrence, and aggressive biologic subtype [TNBC]) were associated with more Foxp3 Treg infiltration. These results are in agreement with those of previous studies reporting the correlation between increased Foxp3 Treg infiltration and unfavorable pathologic phenotypes in breast cancer [12,13,14].
Besides the absolute count of Foxp3 Treg, its relative ratios to CD4 and CD8 T cells were also investigated. An increased ratio between Foxp3 Treg and effector T cells was correlated with various unfavorable parameters (a Ki-67 LI of ≥14%, a worse histologic grade, hormone receptor negativity, HER2 positivity, and tumor recurrence). Few studies have examined Foxp3 Treg infiltration together with effector T cells. CD8 T lymphocytes, a major target of Foxp3 Treg, are a crucial component of tumor-specific cellular-adaptive immunity. Additionally, Foxp3 Treg constitutes a subgroup of CD4 T cells while paradoxically suppressing Foxp3-negative CD4 T cells. Therefore, the relative ratio between Foxp3 Treg and the T effector cell population is presumed to be important for the efficiency of antitumor immunity [24]. Our results provide evidence supporting such a presumption and suggest that both the absolute count of Foxp3 Treg and its relative ratio to effector T cells influence prognostic parameters.
Hormonal receptor negativity and HER2 amplification have been demonstrated to be closely related to increased Foxp3 Treg infiltration in breast cancer [12,13,14]. This study also identifies that these two factors tend to correlate with more Foxp3 Treg infiltration although statistical significance was only confirmed for some variables. Furthermore, TNBC had a tendency to show higher Foxp3 Treg infiltration than the other subtypes, suggesting that Foxp3 Treg might contribute to the immune evasion in TNBC, the most aggressive biologic subtype. Accordingly, Foxp3 Treg can be considered as an important therapeutic target for TNBC, for which no effective targeted therapies are known to date. The modulation of suppressive activity of Treg is expected to potentiate antitumor immunity. Thus, some strategies can be considered for using Treg as a cancer therapeutic modality: some chemotherapy agents are known to reduce the number of Treg and to depress its suppressive activity [25]; systemic elimination of Treg by means of monoclonal antibodies to surface molecules enhances the natural and vaccine-induced antitumor responses of T cells [26]; the differentiation and expansion of Treg can be blocked by the inhibition of factors (such as IL-10 or TGF-β) involved in Treg conversion [27].
Furthermore, univariate analysis revealed that as Foxp3 Treg infiltration and Foxp3 Treg/CD8 T cell ratio in the tumor periphery increased, DFS decreased. Conversely, these two factors had no influence on DFS in the tumor bed. These results are consistent with those published by Gobert et al. [28].
However, in a previous project [29], we investigated Foxp3 Treg infiltration in TNBC, but found no significant correlation between DFS/OS and Foxp3 Treg. The discrepancy in these results probably stemmed from the intrinsic prognostic difference between the study groups.
Nonetheless, the present study failed to demonstrate the difference in OS according to Foxp3 Treg infiltration. Such a result is likely owing to the very few number of patients (3 patients, 2.1%) who died from breast cancer in the study group. This is thought to be a limitation of our study.
In conclusion, the infiltration densities of Foxp3 Treg, CD4, and CD8 T cells were markedly different between the tumor bed and its periphery. In addition to a high absolute count of Foxp3 Treg, a high ratio between Foxp3 Treg and effector T cells was also a significant prognostic factor.
Footnotes
This study was supported by a grant of the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (HI12C0050).
The authors declare that they have no competing interests.
References
- 1.DiPaolo RJ, Glass DD, Bijwaard KE, Shevach EM. CD4+CD25+ T cells prevent the development of organ-specific autoimmune disease by inhibiting the differentiation of autoreactive effector T cells. J Immunol. 2005;175:7135–7142. doi: 10.4049/jimmunol.175.11.7135. [DOI] [PubMed] [Google Scholar]
- 2.Khong HT, Restifo NP. Natural selection of tumor variants in the generation of "tumor escape" phenotypes. Nat Immunol. 2002;3:999–1005. doi: 10.1038/ni1102-999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sakaguchi S. Naturally arising Foxp3-expressing CD25+CD4+ regulatory T cells in immunological tolerance to self and non-self. Nat Immunol. 2005;6:345–352. doi: 10.1038/ni1178. [DOI] [PubMed] [Google Scholar]
- 4.Hori S, Nomura T, Sakaguchi S. Control of regulatory T cell development by the transcription factor Foxp3. Science. 2003;299:1057–1061. [PubMed] [Google Scholar]
- 5.Fontenot JD, Gavin MA, Rudensky AY. Foxp3 programs the development and function of CD4+CD25+ regulatory T cells. Nat Immunol. 2003;4:330–336. doi: 10.1038/ni904. [DOI] [PubMed] [Google Scholar]
- 6.Beyer M, Schultze JL. Regulatory T cells in cancer. Blood. 2006;108:804–811. doi: 10.1182/blood-2006-02-002774. [DOI] [PubMed] [Google Scholar]
- 7.Shevach EM. Mechanisms of foxp3+ T regulatory cell-mediated suppression. Immunity. 2009;30:636–645. doi: 10.1016/j.immuni.2009.04.010. [DOI] [PubMed] [Google Scholar]
- 8.Pandiyan P, Zheng L, Ishihara S, Reed J, Lenardo MJ. CD4+CD25+Foxp3+regulatory T cells induce cytokine deprivation-mediated apoptosis of effector CD4+ T cells. Nat Immunol. 2007;8:1353–1362. doi: 10.1038/ni1536. [DOI] [PubMed] [Google Scholar]
- 9.Zou W. Regulatory T cells, tumour immunity and immunotherapy. Nat Rev Immunol. 2006;6:295–307. doi: 10.1038/nri1806. [DOI] [PubMed] [Google Scholar]
- 10.Garín MI, Chu CC, Golshayan D, Cernuda-Morollón E, Wait R, Lechler RI. Galectin-1: a key effector of regulation mediated by CD4+CD25+ T cells. Blood. 2007;109:2058–2065. doi: 10.1182/blood-2006-04-016451. [DOI] [PubMed] [Google Scholar]
- 11.Sakaguchi S, Miyara M, Costantino CM, Hafler DA. FOXP3+ regulatory T cells in the human immune system. Nat Rev Immunol. 2010;10:490–500. doi: 10.1038/nri2785. [DOI] [PubMed] [Google Scholar]
- 12.Bohling SD, Allison KH. Immunosuppressive regulatory T cells are associated with aggressive breast cancer phenotypes: a potential therapeutic target. Mod Pathol. 2008;21:1527–1532. doi: 10.1038/modpathol.2008.160. [DOI] [PubMed] [Google Scholar]
- 13.Liu F, Lang R, Zhao J, Zhang X, Pringle GA, Fan Y, et al. CD8+ cytotoxic T cell and FOXP3+ regulatory T cell infiltration in relation to breast cancer survival and molecular subtypes. Breast Cancer Res Treat. 2011;130:645–655. doi: 10.1007/s10549-011-1647-3. [DOI] [PubMed] [Google Scholar]
- 14.Bates GJ, Fox SB, Han C, Leek RD, Garcia JF, Harris AL, et al. Quantification of regulatory T cells enables the identification of high-risk breast cancer patients and those at risk of late relapse. J Clin Oncol. 2006;24:5373–5380. doi: 10.1200/JCO.2006.05.9584. [DOI] [PubMed] [Google Scholar]
- 15.Kobayashi N, Hiraoka N, Yamagami W, Ojima H, Kanai Y, Kosuge T, et al. FOXP3+ regulatory T cells affect the development and progression of hepatocarcinogenesis. Clin Cancer Res. 2007;13:902–911. doi: 10.1158/1078-0432.CCR-06-2363. [DOI] [PubMed] [Google Scholar]
- 16.Hiraoka N, Onozato K, Kosuge T, Hirohashi S. Prevalence of FOXP3+ regulatory T cells increases during the progression of pancreatic ductal adenocarcinoma and its premalignant lesions. Clin Cancer Res. 2006;12:5423–5434. doi: 10.1158/1078-0432.CCR-06-0369. [DOI] [PubMed] [Google Scholar]
- 17.Amedei A, Della Bella C, Silvestri E, Prisco D, D'Elios MM. T cells in gastric cancer: friends or foes. Clin Dev Immunol. 2012;2012:690571. doi: 10.1155/2012/690571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mizukami Y, Kono K, Kawaguchi Y, Akaike H, Kamimura K, Sugai H, et al. Localisation pattern of Foxp3+ regulatory T cells is associated with clinical behaviour in gastric cancer. Br J Cancer. 2008;98:148–153. doi: 10.1038/sj.bjc.6604149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Salama P, Phillips M, Grieu F, Morris M, Zeps N, Joseph D, et al. Tumor-infiltrating FOXP3+ T regulatory cells show strong prognostic significance in colorectal cancer. J Clin Oncol. 2009;27:186–192. doi: 10.1200/JCO.2008.18.7229. [DOI] [PubMed] [Google Scholar]
- 20.Elston CW, Ellis IO. Pathological prognostic factors in breast cancer I The value of histological grade in breast cancer: experience from a large study with long-term follow-up. Histopathology. 1991;19:403–410. doi: 10.1111/j.1365-2559.1991.tb00229.x. [DOI] [PubMed] [Google Scholar]
- 21.Hammond ME, Hayes DF, Dowsett M, Allred DC, Hagerty KL, Badve S, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J Clin Oncol. 2010;28:2784–2795. doi: 10.1200/JCO.2009.25.6529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Wolff AC, Hammond ME, Schwartz JN, Hagerty KL, Allred DC, Cote RJ, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J Clin Oncol. 2007;25:118–145. doi: 10.1200/JCO.2006.09.2775. [DOI] [PubMed] [Google Scholar]
- 23.Goldhirsch A, Wood WC, Coates AS, Gelber RD, Thürlimann B, Senn HJ, et al. Strategies for subtypes: dealing with the diversity of breast cancer. Highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann Oncol. 2011;22:1736–1747. doi: 10.1093/annonc/mdr304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Antony PA, Piccirillo CA, Akpinarli A, Finkelstein SE, Speiss PJ, Surman DR, et al. CD8+ T cell immunity against a tumor/self-antigen is augmented by CD4+ T helper cells and hindered by naturally occurring T regulatory cells. J Immunol. 2005;174:2591–2601. doi: 10.4049/jimmunol.174.5.2591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ghiringhelli F, Larmonier N, Schmitt E, Parcellier A, Cathelin D, Garrido C, et al. CD4+CD25+ regulatory T cells suppress tumor immunity but are sensitive to cyclophosphamide which allows immunotherapy of established tumors to be curative. Eur J Immunol. 2004;34:336–344. doi: 10.1002/eji.200324181. [DOI] [PubMed] [Google Scholar]
- 26.Nishikawa H, Sakaguchi S. Regulatory T cells in tumor immunity. Int J Cancer. 2010;127:759–767. doi: 10.1002/ijc.25429. [DOI] [PubMed] [Google Scholar]
- 27.Curti A, Pandolfi S, Valzasina B, Aluigi M, Isidori A, Ferri E, et al. Modulation of tryptophan catabolism by human leukemic cells results in the conversion of CD25- into CD25+ T regulatory cells. Blood. 2007;109:2871–2877. doi: 10.1182/blood-2006-07-036863. [DOI] [PubMed] [Google Scholar]
- 28.Gobert M, Treilleux I, Bendriss-Vermare N, Bachelot T, Goddard-Leon S, Arfi V, et al. Regulatory T cells recruited through CCL22/CCR4 are selectively activated in lymphoid infiltrates surrounding primary breast tumors and lead to an adverse clinical outcome. Cancer Res. 2009;69:2000–2009. doi: 10.1158/0008-5472.CAN-08-2360. [DOI] [PubMed] [Google Scholar]
- 29.Kang H, Cheong H, Cho MS, Koo H, Han WS, Lee KE, et al. Significance of Foxp3 positive regulatory T cell and tumor infiltrating T lymphocyte in triple negative breast cancer. Korean J Pathol. 2011;45:53–61. [Google Scholar]