

Abstract
The occurrence of acute myocardial infarction following a honeybee sting has been very rarely reported in the previous literature. Possible pathogenetic mechanisms include severe hypotension, rarely hypertension and coronary vasospasm with subsequent thrombosis of coronary vessels developed after the release of vasoactive, inflammatory and thrombogenic substances contained in the bee venom. This syndrome is also known as Kounis syndrome. We report a case of a 32-year-old man who presented with acute inferior wall myocardial infarction within 3 h of honeybee sting. He was treated with thrombolytic therapy. Coronary angiogram revealed normal coronary arteries.
Background
Honeybee stings are commonly seen in rural parts of India. Local symptoms including severe pain and burning sensation at the site of sting are the most common manifestations. Acute myocardial infarction (AMI) is rarely associated with honeybee sting.1–4 Kounis syndrome is the concurrence of acute coronary syndrome following mast cell activation induced by allergic or hypersensitivity and anaphylactoid reactions caused by the honeybee sting.5
Case presentation
A 32-year-old man presented to the emergency department with acute chest pain within 3 h after being stung by many honeybees (figure 1). Other than smoking, there were no predisposing cardiac risk factors such as hypertension or diabetes. He had no significant medical history like allergy to any medications. On examination, his blood pressure was 154/90 mm Hg, heart rate 102/min, regular and respiratory rate 18/min. ECG showed sinus tachycardia with ‘ST’ elevation in the inferior leads (figure 2). He was given an injection of streptokinase as a thrombolytic therapy as he presented within 3 h of the onset of chest pain. He was not affordable for immediate primary percutaneous coronary artery intervention. As he was a smoker, it was thought that thrombotic occlusion of coronary artery could be the reason for acute myocardial infarction. He was asymptomatic following thrombolytic therapy and ECG showed signs of resolution (figure 3). Echocardiography demonstrated hypokinesia of basal and mid-inferior wall with mild left ventricular dysfunction and ejection fraction of 45%. Finally, coronary angiogram (CAG) was performed which revealed no coronary artery abnormalities and without any myocardial bridging or calcification (figure 4). He was treated with medications including dual antiplatelet drug, β-blockers, atorvastatin and ramipril. There was no evidence of any other rare condition which can give rise to early myocardial infarction in our case. His admission course was smooth and he was discharged uneventfully 5 days later.
Figure 1.

Periorbital oedema, blackening and bite mark following honeybee stings.
Figure 2.

ECG showing ‘ST’ elevation in leads II, III and aVF.
Figure 3.

ECG showing ‘ST’ resolution following thrombolytic therapy.
Figure 4.
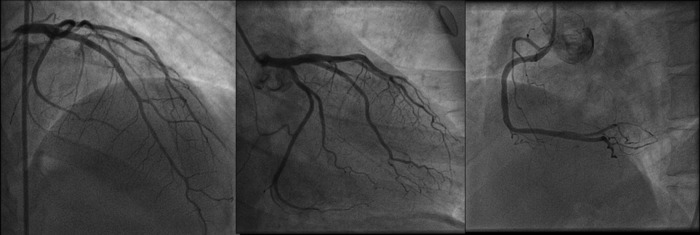
Coronary angiogram revealed normal left and right coronary arteries.
Outcome and follow-up
Since the last follow-up, he was asymptomatic and doing well.
Discussion
Hymenoptera (bees, wasps and yellow jacket) are found worldwide and some of them are venomous animals.4 Hymenoptera stings or bites are responsible for more deaths than those from all other poisonous creatures.4 Systemic reactions after stings are immediate type.1 The most frequent clinical events are hypotension, dyspnoea, anaphylactic shock and angio-oedema.2 Our patient also had angiooedema and periorbital swelling following honeybee stings. Patients usually have hypotension on admission, but a few were hypertensive as in our case. Hymenoptera (bee) venom cause acute coronary syndrome by several mechanisms such as release of allergenic proteins, vasoactive, inflammatory and thrombogenic peptides and amine constituents (histamine, serotonin, bradykinin, leukotrienes, thromboxane), which act on the coronary vasculature and induce coronary artery vasospasm and facilitate platelet aggregation as well as thrombosis; direct cardiotoxic effect of the venom and anaphylactic reaction.5 This sequence of events complicated by thrombosis at the site of spasm also precipitate acute coronary syndrome. The exact mechanism of AMI after hymenoptera sting is still unclear. In our case, as he had developed anaphylactic symptoms, followed by severe chest pain suggestive of AMI with electrocardiographic and echocardiographic features of acute inferior wall myocardial infarction within 3 h of honeybee sting, we suspect Kounis syndrome could be the reason behind acute coronary syndrome. Kounis syndrome is the concurrence of acute coronary syndrome with mast cell activation induced by allergic or hypersensitivity and anaphylactoid reactions following bee stings. There are a few cases of myocardial infarction due to bee or scorpion bites reported in the literature.1–5 Most of these cases had normal coronary artery and had reversible myocardial damage. In our case, he had normal coronary angiogram and the left ventricular function was also normalised during the follow-up. Although, coronary angiogram is the gold standard, the other modality could be CT coronary angiogram to rule out any coronary abnormality in this case, as we strongly suspected Kounis syndrome with vasospasm in this case.
Envenomation caused by honeybees may cause AMI and these reversible changes may be due to local vasoactive, anaphylactic and cardiotoxic effects of honeybee stings.
Learning points.
An acute coronary syndrome can be caused by Kounis syndrome due to a bee sting.
Kounis syndrome is the concurrence of acute coronary syndrome with mast cell activation induced by allergic or hypersensitivity and anaphylactoid reactions following bee stings.
The pathophysiological mechanisms of Kounis syndrome is due to the release of allergenic proteins, vasoactive, inflammatory and thrombogenic peptides and amine constituents (histamine, serotonin, bradykinin, leukotrienes, thromboxane), which act on the coronary vasculature and induce coronary artery vasospasm and facilitate platelet aggregation as well as thrombosis and anaphylactic reaction.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Sanghvi S, Vyas V, Hakim A. Reversible transmural inferior wall ischemia after honeybee sting. Indian Heart J 1997;49:79–80 [PubMed] [Google Scholar]
- 2.Magadle R, Weiner P, Waizman J, et al. Acute myocardial infarction after honeybee sting. Ugeskr Laeger 2000;162:4819–20 [PubMed] [Google Scholar]
- 3.Ceyhan C, Ercan E, Tekten T, et al. Myocardial infarction following a bee sting. Int J Cardiol 2001;80:251–3 [DOI] [PubMed] [Google Scholar]
- 4.Yang HP, Chen FC, Chen CC, et al. Manifestations mimicking acute myocardial infarction after honeybee sting. Acta Cardiol Sin 2009;25:31–5 [Google Scholar]
- 5.Massing JL, Bentz MH, Schlesser P, et al. Myocardial infarction after honeybee sting. Apropos of a case and review of the literature. Ann Cardiol Angiol (Paris) 1997;46:311–15 [PubMed] [Google Scholar]