

Abstract
Kerosene poisoning is a common poisoning in India especially in childhood, and clinical spectrum can range from meager chemical pneumonitis to grave complications such as hypoxia, pneumothorax, pneumomediastinum, and emphysema. Pyopneumothorax that may require aggressive management in the form of thoracotomy has not been reported in literature. We hereby report a 22-year young female who had developed series of respiratory complications including pyopneumothorax following ingestion of kerosene with suicidal intent and was treated successfully.
Keywords: Chemical pneumonitis, kerosene poisoning, pyopneumothorax
INTRODUCTION
Kerosene is a refined oil and belongs to the hydrocarbon group of compounds, obtained from crude petroleum. It is a common poison in India because of easy availability and accessibility, as kerosene is the main fuel used for lighting and cooking among the poor.[1] Poisoning is usually due to ingestion either accidentally (in children) or with suicidal intent (in adults) and some time due to inhalation of fumes. The common manifestations of kerosene poisoning are dyspnoea, cough, tachypnoea, lipoid pneumonitis, bronchitis, and bronchopneumonia, although it can lead to pneumothorax, pneumatoceles, and subcutaneous emphysema.[2]
CASE REPORT
A 22-year young female presented in emergency department with history of ingestion of kerosene (around 20 ml) with suicidal intent, 6 h before admission. At the time of presentation, though she was asymptomatic, smell of kerosene was perceived. On examination, she was tachypnic (respiratory rate—30/min). Her vitals were stable and bilateral basal crepitations were present on chest examination. Other systemic examination was normal. Initial arterial blood gas (ABG) analysis, hemogram, and serum electrolytes were normal, however, chest radiograph showed bilateral lower zone consolidation with right-sided mild pleural effusion [Figure 1]. Possibility of chemical pneumonitis was kept, and she was put on empirical antibiotics (ceftriaxone, azithromycin, and metrogyl), steroid, and intravenous fluids. In next 24 h, patient became dyspnic, her respiratory rate increased up to 50/min, and crepitations were also increased bilaterally. ABG showed hypoxia (Po2 52 and Pco2 32 mmHg) and repeat X-ray chest showed increased consolidation on right side with moderate pleural effusion, left sided consolidation remained unchanged [Figure 2]. Oxygen inhalation was started at the rate of 6 l/min with 100% oxygen mask to maintain oxygen saturation. She showed gradual response to the treatment and was discharged after 2 weeks of treatment. On follow up visit after 2 weeks she had complaints of dyspnoea and fresh chest X-ray showed right-sided moderate hydropneumothorax [Figure 3]. She was readmitted and intercostal drainage (ICD) tube was put. Pleural fluid was purulent and its analysis revealed total leucocyte count of 1840 cells/cumm, differential count—polymorphs 75% and lymphocyte 25%, protein—5.36 g/dl (serum protein—7.32), sugar—56 mg/dl, adenosine deaminase level 75 IU/l, and Gram-positive cocci. Staphylococcus aureus grew on culture that was sensitive to piperacillin-tazobactum and amikacin. Patient was put on antibiotics according to sensitivity pattern but even after 2 weeks of specific therapy there was no significant improvement. Repeat X-ray showed persistent hydropneumothorax, although there was no drainage from ICD tube [Figure 4]. Computed tomography (CT) of chest showed right-sided pyopneumothorax with septations, thickening of overlying pleura, and underlying collapsed consolidated lung with ICD in situ. Small cavitatory lesions were also seen on left side with peripheral consolidation [Figures 5 and 6]. Considering the findings of CT scan, decortication was done after which she improved.
Figure 1.
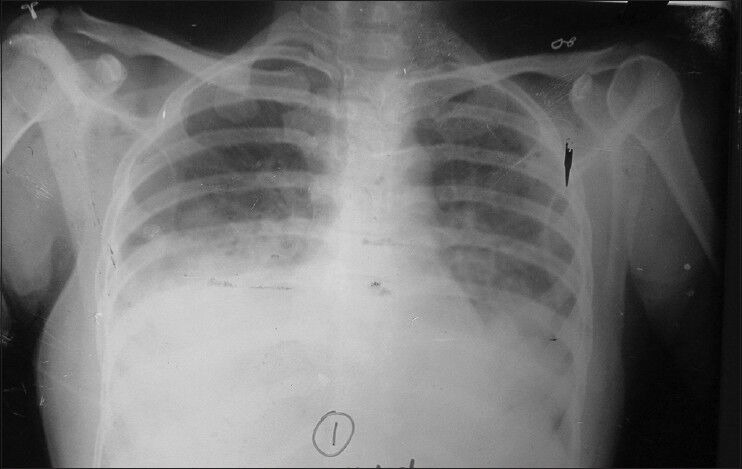
Chest radiograph showing bilateral lower zone consolidation with blunting of right costophrenic angle suggestive of mild pleural effusion
Figure 2.
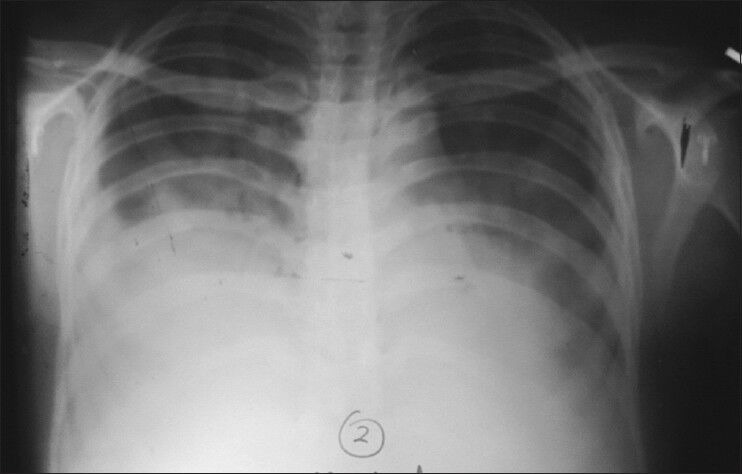
Chest radiograph showing increased consolidation on right side with moderate pleural effusion. Consolidation on left side remains unchanged
Figure 3.
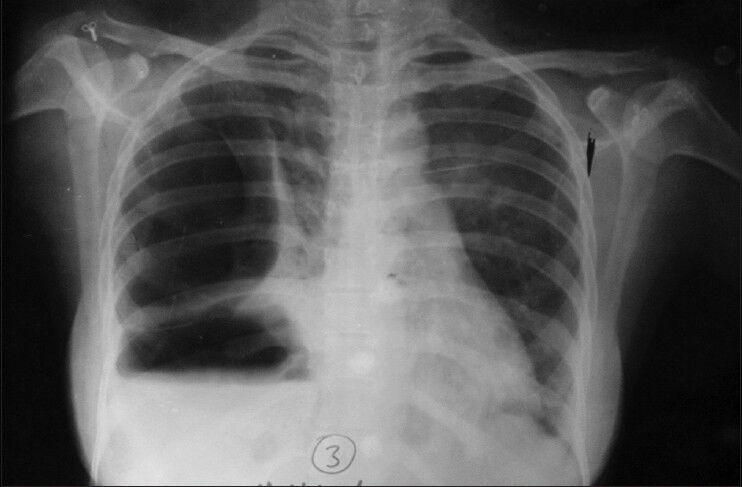
Chest radiograph showing right-sided hydropneumothorax with underlying consolidation. There was resolution of left lower lobe consolidation
Figure 4.
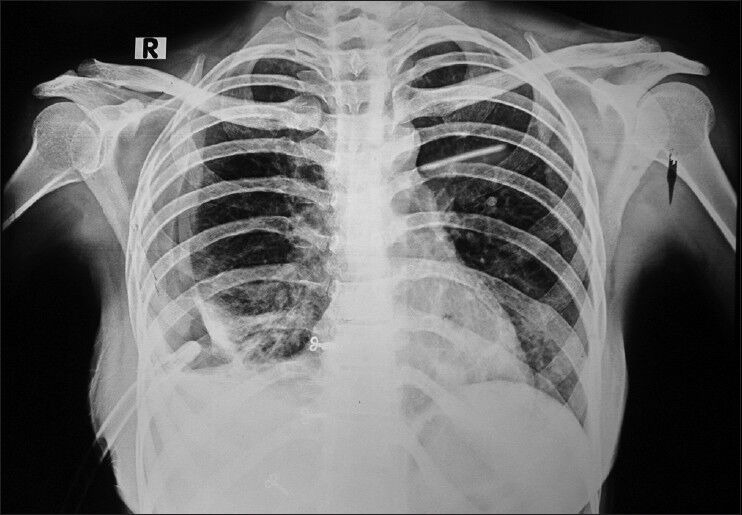
Chest radiograph showing decreased right sided hydropneumothorax with mild expansion of right upper lung with drainage tube in situ
Figure 5.

Computed tomography thorax at lung window settings shows large hydropneumothorax with little air fluid level on right side with few septations with drainage tube in situ. There is a small cavitatory lesion seen in the lower lobe of left lung with mild consolidation at the periphery of the cavity
Figure 6.
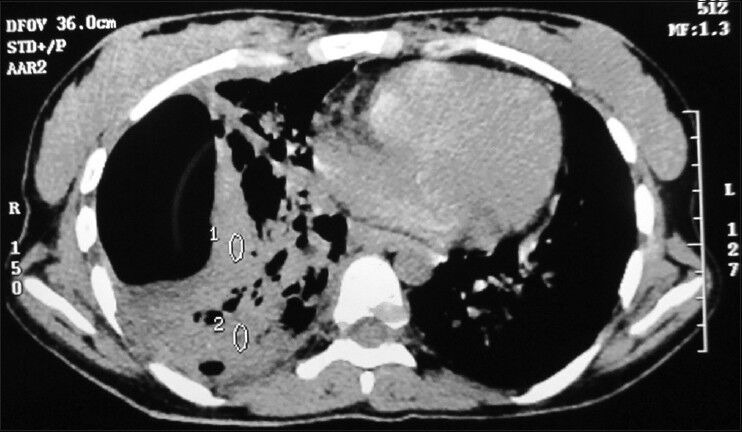
Computed tomography thorax at mediastinal window setting showing right-sided hydropneumothorax with underlying consolidation with air bronchogram sign
DISCUSSION
Kerosene is a liquid mixture of hydrocarbons (chain length C9–16) produced by the distillation of crude oil. In India, kerosene oil is extensively used as fuel for cooking and lighting purposes due to shortage of cooking gas and electricity. The symptoms following ingestion of kerosene can develop soon after to within 10 h. Breathlessness, fever, cough, restlessness due to chemical pneumonitis, and abdominal distension are commonest symptoms. Convulsions, coma, and cyanosis may occur infrequently. Radiological manifestation may appear within hour of ingestion and commonly consists of right basal followed by perihilar infiltrates.[2]
The most frequent adverse effect of any hydrocarbon poisoning is aspiration, which can cause significant pulmonary disease by inducing an inflammatory response, hemorrhagic exudative alveolitis, and loss of surfactant function. The type II pneumocytes are most commonly affected, resulting in decreased surfactant production. This decrease in surfactant results in alveolar collapse, ventilation, perfusion mismatch, and hypoxemia. Hemorrhagic alveolitis can occur, which peaks 3 days after ingestion. Secondary effects in the lungs include pneumothorax, pneumatocele, or bronchopleural fistula. Chemical pneumonitis in most of the cases is interstitial and bilateral.[3] This damage depends on the viscosity, volatility, and the chemical side chains of the hydrocarbon. Among them, viscosity is the single most important determinant of aspiration risk. Lower viscosity and higher volatility are associated with a greater chance of aspiration with resultant pulmonary injury. Lower viscosity promotes penetration into more distal airways, and lower surface tension increases spread over a larger area of lung tissue. The end result of hydrocarbon aspiration is interstitial inflammation, intra-alveolar hemorrhage, bronchial and vascular necrosis, edema, and hyperemia. The hemorrhagic alveolitis and bronchial and vascular necrosis can result in a hemorrhagic pleural effusion. It has been demonstrated clearly in animal experiments that pulmonary injury following ingestion results from aspiration and not from gastrointestinal absorption.[4] These conclusions are consistent with the clinical observation that manifestations rapidly follow ingestion. The gasping and choking that frequently accompany ingestion predispose to aspiration. Vomiting, whether spontaneous or induced, increases the risk of aspiration and adds to the severity of pneumonia. Following ingestion, there is little absorption from the gastrointestinal tract to the systemic circulation.
Few cases of kerosene poisoning-induced pneumothorax and empyema have been reported in literature but pyopneumothorax is a rare entity.[5,6] Following poisoning, respiratory effects occur as a result of aspiration and ingestion leadings to lipoid pneumonitis that increases the transpulmonary pressure. Transpulmonary pressure that exceeds the tensile strength of the non-cartilaginous terminal airways and alveolar saccules can damage the respiratory epithelium. Disruption of epithelial integrity permits air to enter the interstitium, causing pulmonary interstitial emphysema. Persistent elevated transpulmonary pressure facilitates the dissection of air toward the visceral pleural and/or hilum via the peribronchial and perivascular spaces. Rupture of pleural surface allows the adventitial air to decompress into pleural space causing pneumothorax.[5] We are reporting this case because of its rarity and possible long-term morbidity.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Prasad R, Karmakar S, Sodhi R, Karmakar S. Bilateral hemorrhagic pleural effusion due to kerosene aspiration. Lung India. 2011;28:130–2. doi: 10.4103/0970-2113.80329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gupta P, Singh RP, Murali MV, Bhargava SK, Sharma P. Kerosene oil poisoning-A childhood menace. Indian Pediatr. 1992;29:979–84. [PubMed] [Google Scholar]
- 3.Wasserman GS. Hydrocarbon poisoning. Grit Care Q. 1982;4:33–41. [Google Scholar]
- 4.Dice WH, Ward G, Kelley J, Kilpatrick WR. Pulmonary toxicity following gastrointestinal ingestion of kerosene. Ann Emerg Med. 1982;11:138–42. doi: 10.1016/s0196-0644(82)80239-4. [DOI] [PubMed] [Google Scholar]
- 5.Ashir GM, Rabasa AI, Gofama MM, Yahaya SM. Tension pneumothorax following an accidental kerosene poisoning: A case report. Niger Med J. 2009;50:95–6. [Google Scholar]
- 6.Ratageri VH, Shepur TA. Empyema following kerosene poisoning. Indian Pediatr. 2005;42:399. [PubMed] [Google Scholar]