

Abstract
BACKGROUND
The use of quadruple therapy for Helicobacter pylori (H. pylori) eradication is a highly efficacious, gold standard regimen. However, according to a number of studies, this regimen has numerous compliance problems and adverse effects. In the current study we have evaluated the H. pylori eradication rate following a quadruple therapy that included omeprazole, bismuth subcitrate, amoxicillin, and metronidazole in Hormozgan, the most southern province in Iran. Hormozgan Province has high rates of H. pylori infection and its related disorders.
METHODS
A total of 100 patients diagnosed with dyspepsia and H. pylori infection as documented by the (13)C-urea breath test (UBT) or rapid urease test (RUT) were treated with the following quadruple regimen: bismuth subcitrate (120 mg, 2 tablets/q12h), amoxicillin (500 mg/q8h), metronidazole (250 mg/q8h) and omeprazole (20 mg/q12h) for a two-week period. Our primary efficacy outcome was H. pylori eradication as established by a negative UBT at least four weeks after the end of treatment.
RESULTS
Eradication rates were 79%.and 82.3%, respectively, based on the intention-to-treat and per-protocol analyses. Quadruple therapy had a similar effect in women (81%) and men (83.3%) for the eradication of H. pylori, which was not statistically significant. H. pylori eradication rates according to age groups were: 16-20 years (100%), 21-40 years (81%), and 41-60 years (77.8%; p=0.001). There was no significant difference in H. pylori eradication rate between genders in those less than 20 years of age and the middle age group. However in the older group the eradication rate was significantly higher in women (100%) compared to men (66.6%).
CONCLUSION
A two-week quadruple therapy that includes omeprazole, bismuth subcitrate, amoxicillin and metronidazole is a highly effective treatment for H. pylori infection. This treatment has an acceptable eradication rate in Southern Iran. The eradication rate appears to be lower in older men compared with younger men or in women.
Keywords: Helicobacter pylori, Treatment, Iran
INTRODUCTION
Eradication of Helicobacter pylori (H. pylori) infection is a clinically important issue because of its association with benign and malignant diseases of the upper gastrointestinal tract as well as the presence of an increasing antibiotic resistance.1- 3 Despite different regimens for its eradication, complete H. pylori eradication is difficult because the bacterium lives beneath the gastric mucus, adhering to the gastric epithelium, where antimicrobial drugs have restricted access to this area.3 Additionally, H. pylori is resistant to commonly used antimicrobial agents.4 This high resistance has required the development of a new mode of treatment protocols. The ideal therapy for H. pylori eradication has not yet been clearly defined, but it should be simple, safe, and free from side effects, with 100% efficacy and low cost.1 Some studies have shown a decline in the success rate of common therapies, in particular triple regimens whose success rate has plummeted to 25%–60%.5- 7 The numerous causes of this decline are varied, but include poor compliance, high antibiotic resistance, high gastric acidity, high bacterial loading, and polymorphism.7 Recently, the use of quadruple therapy for H. pylori eradication has been considered a highly efficacious, gold standard regimen.8- 10 However some studies have suggested that quadruple therapy is related to increased compliance problems and adverse effects compared with simpler regimens. In a study by de Boer et al., despite limitations, 98% of H. pylori eradication has been reported by using a quadruple regimen that included omeprazole, bismuth, and two types of antibiotics.11
In current study, we evaluated the H. pylori eradication rate following a quadruple therapy of omeprazole, bismuth subcitrate, amoxicillin, and metronidazole in Hormozgan, the most southern province in Iran. This province has high rates of H. pylori infection and its related disorders.
MATERIALS AND METHODS
This clinical trial was performed in 2010 at Shahid Mohammadi Hospital in Hormozgan Province, Iran. Eligible patients were aged 16 years or older who had confirmed H. pylori and dyspepsia or peptic ulcers. Patients were excluded if they had recently used antibiotics to eradicate an adequately recorded H. pylori infection or if they had used antibiotics four weeks prior to study entry. Written informed consent was obtained from all patients before enrollment. Our protocol and one amendment were approved by the Research Ethics Committee of the Hormozgan University of Medical Sciences and the study was undertaken in accordance with the Principles of the Declaration of Helsinki.
For participation, patients had to be positive for H. pylori by the (13)C-urea breath test (UBT) or rapid urease test (RUT). Eligible patients received the quadruple therapy regimen of bismuth subcitrate (120 mg, 2 tablets/q12h), amoxicillin (500 mg/q8h), metronidazole (250 mg/q8h), and omeprazole (20 mg/q12h) for a two-week period.
Our primary efficacy outcome was H. pylori eradication as established by a negative UBT at least four weeks after the end of treatment.
RESULTS
A total of 100 patients were enrolled in the study, of which 72% had a positive UBT, 28% had a positive RUT and 8 patients were diagnosed with peptic ulcers. Of these, 96 patients that were assigned to receive quadruple therapy completed the study. Patient loss was due to either the lack of treatment compliance or not undergoing the UBT. The mean age of participants was 34 years (range: 16-58). Patients were divided into the following age groups: 16 to 20 years (n=8), 21 to 40 years (n=74), and 41 to 58 years (n=18). Males comprised 42% of the study population. After completion of the H. pylori eradication regimen, all patients underwent a UBT between 4 to 24 weeks (mean: 14 weeks) after the end of treatment. The per-protocol eradication rate was 82.3% and intent-to-treat eradication rate was 79%. Quadruple therapy results for H. pylori eradication were similar between women (81.0%) and men (83.3%). This difference was statistically insignificant. However, the H. pylori eradication rates with quadruple therapy were better in the younger age group. The eradication rates according to age category were: 16 to 20 years (100%), 21 to 40 years (81%), and 41 to 58 years (77.8%; p=0.001). Figure 1 compares eradication rates between men and women in each age group. As shown, there was no significant difference in H. pylori eradication rate between genders in the age groups less than 20 years and the middle age group, however in the older group the eradication rate was significantly higher in women than men (100% V/S 66.6%; p=0.001). The most common adverse effects to treatment were metallic taste, diarrhea, dyspepsia, nausea/vomiting and abdominal pain. All adverse effects were mild. Although no severe adverse effects were observed, however two patients discontinued treatment due to non-compliance.
Fig. 1.
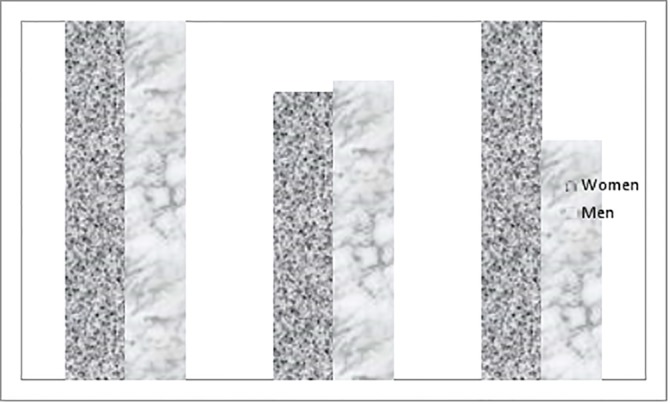
Compares eradication rates between men and women in each age group.
DISCUSSION
In different clinical settings triple therapy is considered to be the first choice for treating H. pylori, however the eradication rate with triple therapy has gradually decreased to less than 80% and as low as 70%. Bismuth-containing quadruple therapy has been attempted in an effort to resolve the high resistance to antibiotics, particularly resistance to clarithromycin in the former regimens. Malfertheiner and colleagues12 showed that bismuth-containing quadruple therapy was effective and acceptable for a first-line therapy to eradicate H. pylori in regions with high levels of clarithromycin resistance. In their study, eradication rates were 80% with quadruple therapy and 55% with triple therapy. In other studies, relatively good results with this quadruple regimen were empirically prescribed, with a mean eradication rate of 77%.13- 21 However, most of these studies prescribed tetracycline, which appeared to be less effective than the amoxicillin used in this study.
Multiple drugs and combination of a PPI-based regimen have been evaluated in the therapy of H. pylori. Combination quadruple therapy for 14 days provides the greatest efficacy than PPI-based triple regimen but may be associated with a relatively higher incidence of drug induced adverse effects.
The duration of treatment with bismuth-containing quadruple therapy is an important consideration that influences compliance rate, which is controversial. In the present study, we have used a similar regimen and longer treatment duration of 14 days, compared to the Malfertheiner study.12 We had a higher eradication rate compared with their study. However, in support of the current study, a Korean study22 that prescribed quadruple therapy for 14 days was more effective than a 7-day regimen. Per-protocol analysis showed a 77% (7 day treatment) versus a 94% (14 day treatment) eradication rate as second-line treatment for H. pylori when empirical triple therapy had failed. One of the most common regimens prescribed in Iran consist variable combination of bismuth, omeprazole, metronidazole and amoxicillin.
In a study by Saberi-Firoozi et al., the eradication rate was only 35% with omeprazole (2 x 40 mg) plus amoxicillin (4 x 500 mg) that was prescribed for two weeks.23 In one study, the combination of omeprazole, amoxicillin and metronidazole was administered to pediatric patients for 14 days and resulted in a 78.9% per-protocol and 73% intention-to-treat eradication rate.24 In a study by Sun et al., patients with peptic ulcers received the triple therapy combination of omeprazole (20 mg), amoxicillin (1000 mg) and metronidazole (400 mg) twice daily for seven days. The eradication rate of H. pylori for the per-protocol analysis was 84.1%. Based on the intention-to-treat analysis, the eradication rate of H. pylori was 82.2%.25 In another Iranian study an intention-to-treat analysis showed eradication rates of 62.5% after a two-week administration of amoxicillin (1 g bid), metronidazole (500 mg bid), bismuth subcitrate (240 mg bid) and ranitidine (300 mg bid).26
In another report from Iran, eradication was assessed by the C-urea breath test four weeks after the end of a ten-day treatment period with omeprazole, amoxicillin, metronidazole and bismuth citrate. Eradication rates were 84% according to the per-protocol approach and 68.8% in the intention-to-treat approach.27 In the Mousavi et al. study, patients received a combination of omeprazole, bismuth subcitrate, amoxicillin, and metronidazole twice daily for a two-week period. In this study, the eradication rate was 70.4% for intention-to-treat and75.7% for per-protocol analysis.28 A quadruple-drug regimen that consisted of bismuth, a PPI, amoxicillin and metronidazole showed a 68% intention-to-treat eradication rate.29- 30 Aminian et al. have reported an eradication rate of 84.1% in intention-to-treat and 85.7% for per-protocol analyses after omeprazole, amoxicillin, metronidazole and bismuth were prescribed twice daily for two weeks.31 Thus, it seems that 14 days of bismuth-containing quadruple therapy might be more appropriate than other regiments with different treatment durations.
In our study, we noted that the eradication rate was associated with some baseline variables such as patients’ age and gender. Older women had a higher eradication rate compared with men in the same age group. Additionally, the eradiation rate gradually decreased with increasing patients’ age. In a study by Cai et al.,32 occupation, gender and protocol compliance were positively associated with eradication rate. Lower eradication rates were observed in farmers and women. In another study by Silva,33 no significant difference was observed regarding sex, tobacco use, alcohol consumption, and NSAID use for H. pylori eradication. However for elderly patients the difference was meaningful. According to our findings, it appeared that older men compared with other sex-age groups had a lower H. pylori eradication rate. Factors that affect this rate such as poor compliance, high antibiotic resistance, high gastric acidity, high bacterial loading, and some polymorphisms might be highlighted more in older males. This should be studied further.
In summary, quadruple therapy including omeprazole, bismuth, amoxicillin and metronidazole results an acceptable eradication rate for H. pylori in Southern Iran. The eradication rate seems to be lower in older men compared to young men or women.
CONFLICT OF INTEREST
The authors declare no conflict of interest related to this work.
Please cite this paper as:
Masoodi M, Panahian M, Rezadoost A, Heidari A. Eradication Rate of Helicobacter pylori using a Two-week Quadruple Therapy: A Report from Southern Iran. Middle East J Dig Dis 2013;5:81-5.
References
- 1.Harris A. Current regimens for treatment of Helicobacter pylori infection. Br Med Bull. 1998;54:195–205. doi: 10.1093/oxfordjournals.bmb.a011670. [DOI] [PubMed] [Google Scholar]
- 2.An international association between Helicobacter pylori infection and gastric cancer . The EUROGAST Study Group Lancet. 1993;341:1359–62. [PubMed] [Google Scholar]
- 3.Veldhuyzen van Zanten SJO, Sherman PM. Helicobacter pylori infection as a cause of gastritis, duodenal ulcer, gastric cancer and non-ulcer dyspepsia: a systematic overview. CMAJ. 1994;150:177–85. [PMC free article] [PubMed] [Google Scholar]
- 4.Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet. 1984;1:1311–5. doi: 10.1016/s0140-6736(84)91816-6. [DOI] [PubMed] [Google Scholar]
- 5.Gumurdulu Y, Serin E, Ozer B, Kayaselcuk F, Ozsahin K, Cosar AM. et al. Low eradication rate of Helicobacter pylori with triple 7-14 days and quadriple therapy in Turkey. World J Gastroenterol. 2004;10:668–71. doi: 10.3748/wjg.v10.i5.668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bigard MA, Delchier JC, Riachi G, Thibault P, Barthelemy P. One-week triple therapy using omeprazole, amoxycillin and clarithromycin for the eradication of Helicobacter pylori in patients with non-ulcer dyspepsia: influence of dosage of omeprazole and clarithromycin. Aliment Pharmacol Ther. 1998;12:383–8. doi: 10.1046/j.1365-2036.1998.00315.x. [DOI] [PubMed] [Google Scholar]
- 7.Chuah SK, Tsay FW, Hsu PI, Wu DC. A new look at anti-Helicobacter pylori therapy. World J Gastroenterol. 2011;17:3971–5. doi: 10.3748/wjg.v17.i35.3971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Malfertheiner P, Megraud F, O’Morain C, Bazzoli F, El-Omar E, Graham D. et al. Current concepts in the management of Helicobacter pylori infection: the maastricht III consensus report. Gut. 2007;56:772–781. doi: 10.1136/gut.2006.101634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.O’Connor A, Gisbert JP, McNamara D, O’Morain C. Treatment of Helicobacter pylori infection 2010. Helicobacter. 2010;15:46–52. doi: 10.1111/j.1523-5378.2010.00774.x. [DOI] [PubMed] [Google Scholar]
- 10.Selgrad M, Malfertheiner P. Treatment of Helicobacter pylori. Curr Opin Gastroenterol. 2011;27:565–70. doi: 10.1097/MOG.0b013e32834bb818. [DOI] [PubMed] [Google Scholar]
- 11.de Boer W, Driessen W, Jansz A, Tytgat G. Effect of acid suppression on efficacy of treatment for Helicobacter pylori infection. Lancet. 1995;345:817–9. doi: 10.1016/s0140-6736(95)92962-2. [DOI] [PubMed] [Google Scholar]
- 12.Malfertheiner P, Bazzoli F, Delchier JC, Celiñski K, Giguère M, Rivière M. et al. Helicobacter pylori eradication with a capsule containing bismuth subcitrate potassium, metronidazole, and tetracycline given with omeprazole versus clarithromycin-based triple therapy: a randomised, open-label, non-inferiority, phase 3 trial. Lancet. 2011;12:905–13. doi: 10.1016/S0140-6736(11)60020-2. [DOI] [PubMed] [Google Scholar]
- 13.Baena Díez JM, López Mompó C, Rams Rams F, García Lareo M, Rosario Hernández Ibáñez M, Teruel Gila J. Efficacy of a multistep strategy for Helicobacter pylori eradication: quadruple therapy with omeprazole, metronidazole, tetracycline and bismuth after failure of a combination of omeprazole, clarithromycin and amoxicillin. Med Clin (Barc) 2000;115:617–9. doi: 10.1016/s0025-7753(00)71640-x. [DOI] [PubMed] [Google Scholar]
- 14.Bilardi C, Dulbecco P, Zentilin P, Reglioni S, Iiritano E, Parodi A. et al. A 10-day levofloxacin-based therapy in patients with resistant Helicobacter pylori infection: a controlled trial. Clin Gastroenterol Hepatol. 2004;2:997–1002. doi: 10.1016/s1542-3565(04)00458-6. [DOI] [PubMed] [Google Scholar]
- 15.Choung RS, Lee SW, Jung SW, Han WS, Kim MJ, Jeen YT. et al. Comparison of the effectiveness of quadruple salvage regimen for Helicobacter pylori infection according to the duration of treatment. Korean J Gastroenterol. 2006;47:131–5. [PubMed] [Google Scholar]
- 16.Chung SJ, Lee DH, Kim N, Jung SH, Kim JW, Hwang JH. et al. Eradication rates of helicobacter pylori infection with second-line treatment: non-ulcer dyspepsia compared to peptic ulcer disease. Hepatogastroenterology. 2007;54:1293–6. [PubMed] [Google Scholar]
- 17.Lee JH, Cheon JH, Park MJ, Kim N, Lee DH, Kim JM. et al. The trend of eradication rates of second-line quadruple therapy containing metronidazole for Helicobacter pylori infection: an analysis of recent eight years. Korean J Gastroenterol. 2005;46:94–8. [PubMed] [Google Scholar]
- 18.Marko D, Calvet X, Ducons J, Guardiola J, Tito L, Bory F. et al. Comparison of two management strategies for Helicobacter pylori treatment: clinical study and cost-effectiveness analysis. Helicobacter. 2005;10:22–32. doi: 10.1111/j.1523-5378.2005.00288.x. [DOI] [PubMed] [Google Scholar]
- 19.Navarro-Jarabo JM, Fernández N, Sousa FL, Cabrera E, Castro M, Ramírez LM. et al. Efficacy of rifabutin-based triple therapy as second-line treatment to eradicate Helicobacter pylori infection. BMC Gastroenterol. 2007;7:31. doi: 10.1186/1471-230X-7-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Nista EC, Candelli M, Cremonini F, Cazzato IA, Di Caro S, Gabrielli M. et al. Levofloxacin-based triple therapy vsquadruple therapy in second-line Helicobacter pylori treatment: a randomized trial. Aliment Pharmacol Ther. 2003;18:627–33. doi: 10.1046/j.1365-2036.2003.01676.x. [DOI] [PubMed] [Google Scholar]
- 21.Chung JW, Lee JH, Jung HY, Yun SC, Oh TH, Choi KD. et al. Second-line Helicobacter pylori eradication: a randomized comparison of 1-week or 2-week bismuth-containing quadruple therapy. Helicobacter. 2011;16:289–94. doi: 10.1111/j.1523-5378.2011.00844.x. [DOI] [PubMed] [Google Scholar]
- 22.Lee BH, Kim N, Hwang TJ, Lee SH, Park YS, Hwang JH. et al. Bismuth-containing quadruple therapy as second-line treatment for Helicobacter pylori infection: effect of treatment duration and antibiotic resistance on the eradication rate in Korea. Helicobacter. 2010;15:38–45. doi: 10.1111/j.1523-5378.2009.00735.x. [DOI] [PubMed] [Google Scholar]
- 23.Saberi-Firoozi M, Massarrat S, Zare S, Fattahi M, Javan A, Etaati H. et al. Effect of triple therapy or amoxycillin plus omeprazole or amoxycillin plus tinidazole plus omeprazole on duodenal ulcer healing, eradication of Helicobacter pylori, and prevention of ulcer relapse over a 1-year follow-up period: a prospective, randomized, controlled study. Am J Gastroenterol. 1995;90:1419–23. [PubMed] [Google Scholar]
- 24.Rafeey M, Ghojazadeh M, Mohamadi-Azar A. Evaluation of Triple Therapy Regimens with Metronidazole or Clarithromycin for Helicobacter Pylori Eradication in Children. Govaresh. 2009;13:233–8. [Google Scholar]
- 25.Sun WH, Ou XL, Cao DZ, Yu Q, Yu T, Hu JM. et al. Efficacy of omeprazole and amoxicillin with either clarithromycin or metronidazole on eradication of Helicobacter pylori in Chinese peptic ulcer patients. World J Gastroenterol. 2005;11:2477–81. doi: 10.3748/wjg.v11.i16.2477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kaviani MJ, Malekzadeh R, Vahedi H, Sotoudeh M, Kamalian N, Amini M. et al. Various durations of a standard regimen (amoxycillin, metronidazole, colloidal bismuth sub-citrate for 2 weeks or with additional ranitidine for 1 or 2 weeks) on eradication of Helicobacter pylori in Iranian peptic ulcer patientsA randomized controlled trial. Eur J Gastroenterol Hepatol. 2001;13:915–9. doi: 10.1097/00042737-200108000-00007. [DOI] [PubMed] [Google Scholar]
- 27.Bahremand S, Nematollahi LR, Fourutan H, Tirgari F, Nouripour S, Mir E. et al. Evaluation of triple and quadruple Helicobacter pylori eradication therapies in Iranian children: a randomized clinical trial. Eur J Gastroenterol Hepatol. 2006;18:511–4. doi: 10.1097/00042737-200605000-00009. [DOI] [PubMed] [Google Scholar]
- 28.Mousavi S, Toussy J, Yaghmaie S, Zahmatkesh M. Azithromycin in one week quadruple therapy for Hpylori eradication in Iran. World J Gastroenterol. 2006;12:4553–6. doi: 10.3748/wjg.v12.i28.4553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Mikaeli J, Mir-Nasseri MM, Manafi-Anari A. Evaluation of OAMB quadruple therapy for Helicobacter pylori eradication in patients with peptic ulcer disease and gastroduodenitis. Govaresh. 2004;44:84–9. [Google Scholar]
- 30.Agah S, Shazad B, Abbaszadeh B. Comparison of Azithromycin and Metronidazole in a Quadruple-Therapy Regimen for Helicobacter pylori Eradication in Dyspepsia. Saudi J Gastroenterol. 2009;15:225–8. doi: 10.4103/1319-3767.56091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Aminian K, Farsad F, Ghanbari A, Fakhreih S, Hasheminasab SM. A randomized trial comparing four Helicobacter pylori eradication regimens: standard triple therapy, ciprofloxacin based triple therapy, quadruple and sequential therapy. Trop Gastroenterol. 2010;31:303–7. [PubMed] [Google Scholar]
- 32.Cai W, Zhou L, Ren W, Deng L, Yu M. Variables influencing outcome of Helicobacter pylori eradication therapy in South China. Helicobacter. 2009;14:91–6. doi: 10.1111/j.1523-5378.2009.00718.x. [DOI] [PubMed] [Google Scholar]
- 33.Silva FM, Zaterka S, Eisig JN, Chehter EZ, Chinzon D, Laudanna AA. Factors affecting Helicobacter pylori eradication using a seven-day triple therapy with a proton pump inhibitor, tinidazole and clarithromycin, in Brazilian patients with peptic ulcer. Rev Hosp Clin Fac Med Sao Paulo. 2001;56:11–6. doi: 10.1590/s0041-87812001000100003. [DOI] [PubMed] [Google Scholar]