

Abstract
Anemia is the most common hematologic disorder in patients with ulcerative colitis (UC). In some cases, normochromic anemia results from the presence of chronic disease; however blood loss or malabsorption may lead to an iron deficiency anemia with hypochromic appearance. Other rare hematologic manifestations associated with UC include myelodysplastic syndromes and leukemia. Several investigators have suggested a clinical association between inflammatory bowel disease and myelodysplastic syndrome, which may they share an immune dysfunction and impairment of T-lymphocytes activities. UC is an inflammatory bowel disease of unknown etiology that mainly affects the mucosa of the colon. Immune mechanisms play an important role in UC, and immunogenetic factors have been implicated in the development of the disease. Aplastic anemia is a bone marrow stem cell disorder characterized by ineffective hematopoiesis, leading to pancytopenia. Although aplastic anemia is frequently idiopathic, the immune-mediated suppression of hematopoiesis may be implicated in at least half of patients, since more than half of these patients achieve hematological remission in response to immunosuppressive therapy. We report here a rare case of UC associated with pancytopenia requiring a blood transfusion in which a bone marrow examination showed aplastic anemia. A common pathogenic link between UC and aplastic anemia is suggested in this patient on the basis of the shared immunologic impairment underlying both diseases.
Keywords: Ulcerative colitis, Aplastic anemia, HLA-DR2, Cyclosporine
INTRODUCTION
Anemia is the most common hematologic disorder in patients with ulcerative colitis (UC). In some cases, normochromic anemia results from the presence of a chronic disease; alternatively, blood loss or malabsorbtion may lead to an iron deficiency, resulting in hypochromic anemia.1 Other rare hematologic
manifestations associated with UC include myelodysplastic syndromes and leukemia.2 Several investigators have suggested a clinical association between inflammatory bowel disease and myelodysplastic syndrome, since they share an immune dysfunction that impairs the activities of T- lymphocytes.3- 6 UC is an inflammatory bowel disease of unknown etiology that mainly affects the mucosa of the rectum and colon. Immune mechanisms play an important role in UC, and immunogenetic factors have been implicated in the development of the disease. Aplastic anemia is a bone marrow stem cell disorder characterized by ineffective hematopoiesis, leading to pancytopenia. Although aplastic anemia is frequently idiopathic, the immune-mediated suppression of hematopoiesis may be implicated in at least half of patients, since more than half of these patients achieve hematological remission in response to immunosuppressive therapy. We report here a rare case of UC associated with pancytopenia requiring blood transfusion in whom bone marrow examination showed aplastic anemia. A common pathogenic link between UC and aplastic anemia is suggested in this patient, that may be explained on the basis of a shared underlying immunologic impairment in both diseases.
CASE REPORT
A 45-year-old man a known case of ulcerative colitis since 7 years ago was admitted to the hematology wardof our hospital with fatigue and high fever.
At the first (7 years ago) he presented with bloody diarrhea (up to 10 urgent trips to bathroom per day), tenesmus, emergency sensation, fever, abdominal pain, and weight loss (about 5-lb) to the emergency department for 7 days. He denied emesis or extra intestinal manifestations. Laboratory evaluation and abdominal radiographs were significant only for a hemoglobin level of 10.8 g/dl. He has had no history of medical illness or surgeries, recent antibiotic or nonsteroidal anti-inflammatory drug use, and no known sick contacts or exposure to tainted foods. He has had experienced increased emotional stress for several weeks due to tumultuous personal relationship. He is a lifelong nonsmoker.
The patient was admitted in the hospital and treated for presumed infectious enterocolitis for intravenous hydration, and empirical ciprofloxacin. Stool culture was negative for infection, but fecal leukocytes were present. After 48 hours with minimal response to therapy, he underwent a flexible sigmoidoscopy and biopsies were taken. Sigmoidoscopy (Figure 1,2), showed friable and erythematous mucosa in a diffuse circumferential distribution from the anal verge to the splenic flexure with petechial hemorrhage, shallow ulcerations surrounded by injected mucosa, and an abnormal vessel pattern in the sigmoid to descending colon. The changes involved a length of 50 cm from anal verge. There were no pseudomembranes. Histologic evaluation showed acute and chronic inflammation with crypt branching and irregularity of size and shape, with an increase in chronic inflammatory cells in the lamina propria (Figures 2,3,4).
Fig. 1.
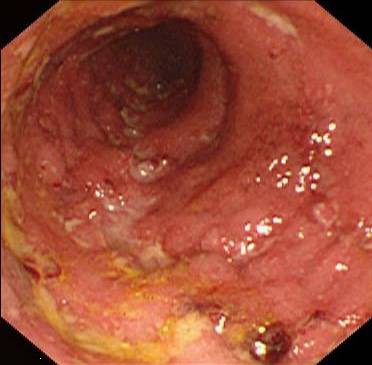
Endoscopic view of the colon revealed numerous ulcers surrounded by injected mucosa. The ulcers were irregularly shaped and shallow. Lesions were present continuously from the rectum to the transverse colon.
Fig. 2.
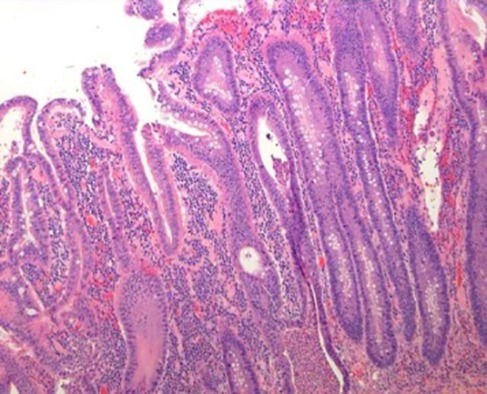
Chronic architectural changes in ulcerative colitis (UC). One can see crypt branching and irregularity of size and shape, with an increase in chronic inflammatory cells in the lamina propria.
Fig. 3.
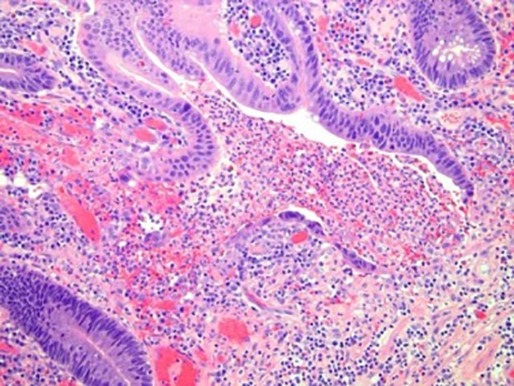
High-power view of a crypt abscess shows the crypt to be dilated and filled with neutrophils and debris.
Fig. 4.

High-power view of a crypt abscess
Ultimately the patient was diagnosed as a case of left sided UC. The bloody diarrhea resolved after 2 weeks of treatment with mesalazine (4g/day) and hydrocortisone intravenously (300mg/day). The steroid dose was reduced and eventually discontinued after 5 months of treatment.
Two years ago referred with relapse of UC, and was treated with mesalazine (4g/day) and prednisolone (30mg/day) for the exacerbation of UC. Despite his relief of his ulcerative colitis, the patient’s laboratory data showed a worsening of the pancytopenia without any gastrointestinal symptoms. His Laboratory findings revealed a hematocrit of 14.5%, and hemoglobin 11.9 g/dl with normocytic appearance (MCV; 94.1 fl & reticulocytes 9×109/liter), white blood cell count (WBC) of 2 ×109/liter, an absolute neutrophilcount (ANC) of 0.3× 109/liter, and a platelet count of 80 × 109/liter. Bone marrow biopsy was consistent with a diagnosis of aplastic anemia (AA). The patient’s medical history was negative for exposure to a myelotoxic agent, a recent infection, blood transfusion, sexual promiscuity, or acute hepatitis. The patient’s serum IgG and IgA concentrations and C3 complement were normal. Serum anti-nuclear antibody and anti-DNA antibody were also negative.
In the hospital course his hemoglobin level dropped to 5.9g/dl; WBC count was 3.1×109/liter; and platelets counts were dropped to 68×109/liter. A bone marrow aspirate and biopsy was done for patient that showed trilineage hypoplasia, and a diagnosis of aplastic anemia was made. Two units of blood were transfused, and treatment with Danazol was initiated. The dose of Danazol was adjusted between 250-300 mg/day. Three month after termination of Danazol, pancytopenia was relapsed and the treatment with cyclosporine (CyA; 300mg/day) was initiated. The dose of CyA was adjusted to maintain a trough concentration between 200~250ng/ml in the whole blood. The patient’s hemoglobin level had increased to 10.2g/dl, his WBC count raised to 5.4×109/liter, and his platelet count to 132×109/liter. The ulcerative colitis has remained in remission, and the patient’s blood counts remained stable in his follow up.
DISCUSSION
This is a reported case of UC associated with aplastic anemia. Several cases of salazosulfapyridine or mesalazine-associated aplastic anemia have been reported in UC patients; according to current recommendations, these medications should be discontinued immediately in the event of bone marrow suppression.7In our case, however, the thrombocytopenia was present before any diagnosis of UC or treatment with mesalazine. The clinical course of this case implies that the subsequent pancytopenia did not arise from 6 drug-induced aplastic anemia. Currently, the immune-mediated suppression of hematopoiesis has been considered as a potential etiology for bone marrow failure in patient’s with aplastic anemia, because more than half of aplastic anemia patients respond to immunosuppressive therapies, such as treatment with antithymocyte globulin or antilymphocyte globulin and CyA. Our patient’s aplastic anemia responded well to treatment with Danazol, CyA ”. This positive response strongly suggests an immunopathogenic etiology in the present case. A response to monotherapy with CyA is suggestive of such a pathogenesis, since CyA acts by directly suppressing lymphokine production by T cells. Other groups 8- 10 have reported an increased frequency of positive HLA-DR2 test results in patients with aplastic anemia. As with many diseases suspected of having an autoimmune etiology or pathogenesis, the associations between UC and certain HLA class Ⅱ genes have been investigated. Several investigators have been reported an associations between HLA-DR2 and UC.11, 12 Recent studies applying molecular techniques and typing for specific HLA-DRB1 subtypes have shown that within the HLA-DR2 group, the DRB1*1501 and DRB1*1502 alleles, but not the DRB1*1601 or DRB1*1602 alleles, are positively associated with UC.13, 14
Other reports concerning HLA serologic typing in Japan have shown strong associations between a susceptibility to extensive or intractable UC and the HLA-DRB1*1502 allele.14,15 The observation that the same HLA-DR2 haplotype is associated with both UC and aplastic anemia suggests a common immunologic impairment underlying the development of these diseases. Primary sclerosing cholangitis (PSC) is an instructive example of an autoimmune disorder that appears to be associated with UC. Several reports have suggested that patients prone to develop PSC might represent a DR3 subgroup among patients with UC.16 In our case, the patient’s HLA serological type was HLA-DRB1*1502. Our patient’s clinical course showed a relapse-remittance” pattern, consistent with a report that DRB1*1502 may favor an intractable form of UC. In contrast, UC associated with DRB1*1501 is less likely to show an intractable clinical course.15
Interestingly, DRB1*1501 is not only associated with a lower likelihood of intractability in UC patients, but also associated with a good response to CyA therapy in patients with aplastic anemia. Recently, CyA has been used to induce remission in patients with UC who are unresponsive to conventional therapies such as salazosulfapyridine and corticosteroids. A specific serologic HLA type may prove to predict the response to CyA therapy in UC patients, as has been seen in patients with aplastic anemia.
One plausible explanation for the association between UC and aplastic anemia in the present case is that an underlying immunologic dysfunction may arise from certain cytokines regulated by specific HLA genes. Among the various cytokines, high concentrations of proinflammatory cytokine, such as interleukin-1 (IL-1) and tumor necrosis factor-α (TNF-α), have been noted in both inflammatory bowel disease and aplastic anemia.17- 20 In particular, TNF-α has been implicated as a key mediator in the inflammatory process in UC and Crohn’s disease; for example, TNF-α antibodies are clinically effective in Crohn's disease and ulcerative colitis. On the other hand, an elevation of TNF-α has been reported in plasma from the bone marrow and peripheral blood in patients with aplastic anemia, but not from healthy individuals.20 The overproduction of TNF-α by T cells might explain the inhibition of hematopoietic precursor cells in aplastic anemia. The same overproduction of inflammatory cytokines may also account for the subsequent development of UC in the present case.
Several investigators have indicated that HLA genes can regulate the function or synthesis of cytokines. Miller and Kaplan 21 reported that serum IL-2 and TNF-α levels were elevated in patients with primary biliary cirrhosis and HLA-DR4, but were decreased in patients without HLA-DR4. Similarly, in systemic lupus erythematosus (SLE), a complex autoimmune disease with varied manifestations, the HLA-DR4 haplotype is associated with a high serum concentration of TNF-α. HLA-DR4 is also associated with a decreased likelihood of nephritis. Further investigation regarding the associations between HLA-DR2 and inflammatory cytokines, including TNF-α and IL-1, are needed.22
Myelodysplastic syndrome differs greatly from aplastic anemia. In most affected patients, myelodysplastic syndrome cannot be explained by an immunological dysfunction, despite its association with UC. These patients do not respond to immunosuppressive therapies including treatment with CyA and antithymocyte globulin. Myelodysplastic syndrome is considered to be a monoclonal bone marrow stem cell disorder characterized by peripheral cytopenia and marrow dysplasia, rather than a disorder arising from immune-mediated suppression of hematopoiesis as in aplastic anemia.
Why no previous cases of UC with aplastic anemia have been reported despite the apparent immunologic associations, is in sharp contrast to the various reports of association between UC and myelodysplastic syndrome.
Based on the findings seen in our case, aplastic anemia should be considered in a differential diagnosis of patients with UC in whom pancytopenia develops with no other evident causes, such as a drug reaction, hepatitis or other kind of viral infection. Although the association between UC and aplastic anemia may be coincidental, an immunological pathogenesis seems plausible. We suspect that the elucidation of the underlying immune dysfunction will enhance our understanding of the pathogenesis of both UC and aplastic anemia.
CONFLICT OF INTEREST
The author declares no conflict of interest related to this work.
Please cite this paper as:
Ghavidel A.Ulcerative Colitis Associated with Aplastic Anemia;A Case Report. Middle East J Dig Dis 2013;5:230-4.
References
- 1. Retsky JE, Kraft CS.The extraintestinal manifestations of inflammatory bowel disease.In Inflammatory bowel disease.Kisner JB, Shorer RG (eds). Baltimore, Williams and Wilkins, 1995:p.474-91.
- 2.Mir Madjlessi SH, Framer RG, Weick JK. Inflammatory bowel disease and leukemia. Dig Dis Sci. 1986;31:1025–31. doi: 10.1007/BF01300254. [DOI] [PubMed] [Google Scholar]
- 3.Eng C, Farraye FA, Shulman LN, Peppercorn MA, Krauss CM, Connors JM, Stone RM. The association between the myelodysplastic syndromes and Crohn disease. Ann Intern Med. 1992;117:661–2. doi: 10.7326/0003-4819-117-8-661. [DOI] [PubMed] [Google Scholar]
- 4.Harewood GC, Loftus EV Jr, Tefferi A, Tremaine WJ, Sandborn WJ. Concurrent inflammatory bowel disease and myelodysplastic syndromes. Inflam Bowel Dis. 1999;5:98–103. doi: 10.1097/00054725-199905000-00005. [DOI] [PubMed] [Google Scholar]
- 5.Sahay R, Prangnell DR, Scott BB. Inflammatory bowel disease and refractory anemia (myelodysplasia) Gut. 1993;34:1630–1. doi: 10.1136/gut.34.11.1630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hebbar M, Kozlowski D, Wattel S, Mastrini S, Dievart M, Duclos B. et al. Association between myelodysplastic syndromes and inflammatory bowel diseaseReport of seven new cases and review of the literature. Leukemia. 1997;11:2188–91. doi: 10.1038/sj.leu.2400863. [DOI] [PubMed] [Google Scholar]
- 7.Laidlaw ST, Reilly JT. Antilymphocyte globulin for mesalazine-associated aplastic anemia. Lancet. 1994;343:981–2. doi: 10.1016/s0140-6736(94)90108-2. [DOI] [PubMed] [Google Scholar]
- 8.Nakao S, Takami A, Sugimori N, Ueda M, Shiobata S, Matsuda T. et al. Response to immunosupressive therapy and an HLA-DRB1 allele in patients with aplastic anemia: HLA-DRB1*1501 does not predict response to antithymocyte globulin. Br J Haematol. 1996;92:155–8. doi: 10.1046/j.1365-2141.1996.293825.x. [DOI] [PubMed] [Google Scholar]
- 9.Chapuis B, Von Fliedner VE, Jeannet M, Merica H, Vuagnat P, Gratwohl A. et al. Increased frequency of DR2 in patients with aplastic anemia and increased DR sharing in their parents. Br J Haematol. 1986;63:51–7. doi: 10.1111/j.1365-2141.1986.tb07494.x. [DOI] [PubMed] [Google Scholar]
- 10.Nimer SD, Ireland P, Meshkinpour A, Frane M. An increased HLA-DR2 frequency is seen in aplastic anemia patients. Blood. 1994;84:923–7. [PubMed] [Google Scholar]
- 11.Asakura H, Tsuchiya M, Aiso S, Watanabe M, Kobayashi K, Hibi T. et al. Association of the human lymphocyte-DR2 antigen with Japanese ulcerative colitis. Gastroenterology. 1982;82:413–8. [PubMed] [Google Scholar]
- 12.Sugimura K, Asakura H, Mizuki N, Inoue M, Yagita A, Tsuji K. et al. Analysis of genes within the HLA region affecting susceptibility to ulcerative colitis. Hum Immunol. 1993;36:112–8. doi: 10.1016/0198-8859(93)90113-f. [DOI] [PubMed] [Google Scholar]
- 13.De la Concha EG, Fernandez-Arquero M, Santa-Cruz S, Lopez-Nava G, Figueredo MA, Diaz-Rubio M. et al. Positive and negative associations of distinct HLA-DR2 subtypes with ulcerative colitis. Clin Exp Immunol. 1997;108:392–5. doi: 10.1046/j.1365-2249.1997.3951285.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Futami S, Aoyama N, Honsako Y, Tamura T, Morimoto S, Nakashima T. et al. HLA-DRB1*1502 allele, subtype of DR15, is associated with susceptibility to ulcerative colitis and its progression. Dig Dis Sci. 1995;40:814–8. doi: 10.1007/BF02064985. [DOI] [PubMed] [Google Scholar]
- 15.Masuda H, Nakamura Y, Tanaka T, Hayakawa S. Distinct relationship between HLA-DR genes and intractability of ulcerative colitis. Am J Gastroenterol. 1994;89:1957–62. [PubMed] [Google Scholar]
- 16.Leidenius MH, Koskimies SA, Kellokumpu IH, Hockerstedt KA. HLA antigen in ulcerative colitis and primary sclerosing cholangitis. APMIS. 1995;103:519–24. doi: 10.1111/j.1699-0463.1995.tb01400.x. [DOI] [PubMed] [Google Scholar]
- 17.Braegger CP, Nicholls S, Murch SH, Stephens S, MacDonald TT. Tumor necrosis factor alpha in stool as a marker of intestinal inflammation. Lancet. 1992;339:89–91. doi: 10.1016/0140-6736(92)90999-j. [DOI] [PubMed] [Google Scholar]
- 18.Casini-Raggi V, Kam L, Chong YJT, Fiocchi C, Pizarro TT, Cominelli F. Mucosal imbalance of IL-1 and IL-1 receptor antagonist in inflammatory bowel diseaseA novel mechanism of chronic intestinal inflammation. J Immunol. 1995;154:2434–40. [PubMed] [Google Scholar]
- 19.Hirayama Y, Kohgo Y, Matsunaga T, Ohi S, Sakamaki S, Niitsu Y. Cytokine mRNA expression of bone marrow stromal cells from patients with aplastic anemia and myelodysplastic syndrome. Br J Haematol. 1993;85:676–683. doi: 10.1111/j.1365-2141.1993.tb03208.x. [DOI] [PubMed] [Google Scholar]
- 20.Schulz JC, Shahidi NT. Detection of tumor necrosis factor-alfa in bone marrow plasma and peripheral blood plasma from patients with aplastic anemia. Am J Hematol. 1994;45:32–38. doi: 10.1002/ajh.2830450106. [DOI] [PubMed] [Google Scholar]
- 21.Miller LC, Kaplan MM. Serum interleukin-2 and tumor necrosis factor-α in primary biliary cirrhosis: Decrease by colchicine and relationship toHLA-DR4. Am J Gastroenterol. 1992;87:465–70. [PubMed] [Google Scholar]
- 22.Jacob CO, Fronek Z, Lewis GD, Koo M, Hansen JA, McDevitt HO. Heritable major histocompability complex class Ⅱ-associated differences in production of tumor necrosis factor a: relevance to genetic predisposition to systemic lupus erythematosus. Proc Nat lAcad Sci. 1990;87:1233–7. doi: 10.1073/pnas.87.3.1233. [DOI] [PMC free article] [PubMed] [Google Scholar]