

Abstract
BACKGROUND
Obesity is currently emerging as a global epidemic, affecting 10% of adult population worldwide. The primary objective of the current systematic review is to describe the trend of overall prevalence of obesity in Iranian women and menthrough a meta-analysis.
METHODS
We searched the medical literature published from 1990 to 2007 in Medline (PubMed), EMBASE database, and the Iranian digital library. All published reports of research projects, papers in relevant congresses, unpublished crude data analysis, proceedings, books and dissertations were reviewed. Data from eligible papers that fulfilled the qualification criteria entered meta-analysis (Random Model).
RESULTS
Data from 209,166 individuals were analyzed. The overall prevalence of obesity in adults was 18.5% (95%CI: 15.1-21.8), respectively. The prevalence of obesity in men and women was 12.9% (95%CI: 10.9-14.9) and 26.2% (95%CI: 21.3-30.5), respectively. The trend of obesity was similar in both genders; women had almost a constantly higher risk of obesity than men during the recent two decades.
CONCLUSION
Data from 209,166 individuals were analyzed. The overall prevalence of obesity in adults was 18.5% (95%CI: 15.1-21.8), respectively. The prevalence of obesity in men and women was 12.9% (95%CI: 10.9-14.9) and 26.2% (95%CI: 21.3-30.5), respectively. The trend of obesity was similar in both genders; women had almost a constantly higher risk of obesity than men during the recent two decades.
Keywords: Obesity, Systematic Review, Meta-analysis, Iran
INTRODUCTION
Obesity is currently emerging as a global epidemic, affecting more than 200 million men and almost 300 million women worldwide, accounting for 10% of the adult population.1 Obesity is a major culprit of poor health as it is associated with increased mortality and reduced life expectancy.2 As the most prevalent metabolic disorder in the developed countries, obesity is now on the rise as a significant cause of disease burden in developing nations.3 According to current statistics, obesity will be a major public health concern in near future in most low- and middle-income countries, particularly in urban areas.1
It is known that demographic characteristics such as age, race, gender and socio-economic status affect the prevalence of obesity.4 Urbanization, increased energy intake, and sedentary life style are common important contributors to obesity. However, the prevalence of obesity varies markedly across countries, reflecting different risk factors among various populations around the world.1
The Iranian population comprises several ethnicities with quite different lifestyles and cultures which might lead to variations in the prevalence of obesity.5 Many studies have characterized the prevalence of obesity, targeting different age groups and sex distributions around the country. However, there is considerable variation in the estimates of obesity across the studies.
Given that valuable information can be extracted from existing data sources, regular updates of the statistics of obesity are necessary to identify the epidemiologic trend of such disorders in Iran. Hence, the primary objective of the current systematic review is to estimate the trend of overall prevalence of obesity in Iranian women and men. The secondary objective is to assess the degree of heterogeneity and address its potential sources.
MATERIALS AND METHODS
Search Strategy
We searched the English-language medical literature published from January 1990 to December 2007 using the Medline database of the National Library of Medicine, Embase database and the Iranian Digital Library. The medical subject headings (Mesh) were “obesity”, “body mass index” combined with “prevalence” and “Iran” including all subheadings. In addition, all abstracts, conference proceeding, titles of thesis, dissertations and reports in other databases in Persian (Farsi) language such as Iranmedex, Irandoc, Scientific Information Systems (SID), and Iranian National Library (INL) were searched with a similar strategy; the Persian keywords were equivalent to their English words. Moreover, all submitted Scientific Journals of Iranian medical universities published since 2007 were reviewed by hand searching. As the crude data of non-communicable disease risk factor (STEPS study) are available from 2005 onwards, we also included these findings after data analysis. References of selected articles were checked to maximize the sensitivity of our search.
Obesity Definition
We included those studies that evaluated obesity based on anthropometric measurements (height and weight) in order to calculate body mass index (BMI). All the papers defining obesity as BMI ≥ 30 Kg/m2 were included.
Study selection
In the second step, all sources that reported the prevalence of obesity were reviewed. We then performed a critical appraisal of all papers, deeply and independently, by two well-educated individuals. We generated a simple checklist to evaluate the main issues in descriptive studies such as the sampling method and the validity of measurements. A total of seven items were to be checked, and articles which addressed at least five of them were included (Appendix 1). Studies gaining a quality score lower than 5 were excluded, as well as those which estimated the prevalence of obesity in a non-random sample or in a small sample (less than 100 individuals). Moreover, we excluded duplicated citations and studies that did not mention data collection date or location.
Data extraction
The relevant data from qualified studies were extracted independently by two individuals and listed on Microsoft Excel® worksheets. The unmatched scores were checked by a third investigator to make the final decision on including or excluding the study from the list. Obesity prevalence, publication date, reference date, and sample size were extracted for each individual sex and totally.
Statistical analysis
The variance of obesity prevalence in each study was computed using the binomial distribution formula. After checking the heterogeneity of prevalence
across studies, we decided to apply the random effect model to estimate the overall prevalence of obesity. The reported prevalence of obesity was modeled against the year of data collection (reference year) in both men and women, separately. The best-fit model was determined by R2 as the goodness of fit indicator to explore the trend of obesity during the last three decades. All analyses were performed using Stata software version 10.
RESULTS
Findings from a total of 32 studies, comprising 209,166 individuals aged 14 - 81 years, were included. All studies defined obesity based on BMI more than 30 Kg/m2 (Table 1). Based on time of data collection, we grouped the findings of papers into four categories. As shown in Table 2, the overall prevalence of obesity for adults was 18.5% (CI95% 15.1- 21.8). The prevalence of obesity in men and women was 12.9% and 26.2%, respectively. It is clear that the
Table 1. Description of studies fulfilling our eligibility criteria .
| Author |
Reference
year |
Province | Sample Size |
Publication
Year |
% Obesity |
Age
groups |
Quality
score |
||||
| Total | Male | Female | Total | Male | Female | ||||||
| GR.Pishdad 6 | 1993-1994 | Fars | 3378 | 2301 | 1077 | 1996 | 4.3 | 2.5 | 8 | 20-74 | 7 |
| A.Barzigar 7 | 1996 | Gilan | 2423 | 973 | 1357 | 1997 | 24.6 | 11.5 | 34 | >25 | 5 |
| R.Ghorbani 8 | 1996-1997 | Semnan | 1921 | 975 | 946 | 1999 | 19.8 | 12.6 | 27.1 | 20-55 | 5 |
| F.Azizi 9 | 1998-1999 | Tehran | 2102 | 808 | 1294 | 2005 | 16.5 | 32.7 | 20-80 | 7 | |
| M.Jamshidian 10 | 2000 | Tehran | 749 | 749 | 2004 | 41.4 | 40-60 | 6 | |||
| H.Soori 11 | 2000 | Khozestan | 1540 | 899 | 641 | 2001 | 13.9 | 11.9 | 36.6 | 18-84 | 7 |
| M.Mojibian 12 | 1999-2000 | Yazd | 570 | 570 | 2001 | 16.3 | 16.3 | 15-65 | 6 | ||
| T.Azizi 13 | 1999-2002 | Tehran | 7033 | 2992 | 4041 | 2005 | 27.5 | 16.3 | 35.8 | 30-69 | 6 |
| Z.Mortazavi 14 | 2000-2001 | Sistan&Blochestan | 720 | 292 | 428 | 2002 | 1.3 | 1 | 1.4 | 18-43 | 6 |
| A.Akhavantabib15 | 2000-2001 | Isfahan,Markazi,Najafabad | 12514 | 6141 | 6373 | 2003 | 15.5 | 9.3 | 23.4 | >19 | 7 |
| H.Sezavar 16 | 2001 | Ardabil | 384 | 200 | 184 | 2001 | 15.9 | 13.5 | 19 | 20-80 | 5 |
| F.Kavian 17 | 2001 | Tehran | 503 | 503 | 2002 | 11 | 25-45 | 6 | |||
| SM. Safari 18 | 2001 | National Survey | 8800 | 2006 | 21.7 | 12.9 | 30.5 | 45-60 | 7 | ||
| PORA study 19 | 2001 | National Survey | 8753 | 4201 | 4552 | 2004 | 22 | 12.9 | 30.5 | 45-60 | 7 |
| F.Azizi 20 | 1999-2002 | Tehran | 1766 | 911 | 855 | 2002 | 46.9 | 43.6 | 51.7 | >60 | 6 |
| H.Fakhrzadeh 21 | 2000-2001 | Booshehr | 1437 | 1437 | 2002 | 10.2 | >18 | 6 | |||
| F.Azizi 9 | 2001-2002 | Tehran | 2102 | 808 | 1294 | 2005 | 20.8 | 40.3 | 20-80 | 7 | |
| S.Akbari 22 | 2002 | Lorestan | 986 | 986 | 2003 | 7.3 | 14-18 | 6 | |||
| H.Mostafavi 23 | 2002-2003 | Fars | 3245 | 1305 | 1940 | 2005 | 11.7 | 7.3 | 14.8 | >18 | 7 |
| F.Rahmati 24 | 2003 | Tehran | 3931 | 1548 | 2360 | 2004 | 3.2 | 4.2 | 2.5 | 17-48 | 5 |
| GH.Vaghari 25 | 2003 | Golestan | 2854 | 2854 | 2004 | 16.4 | >18 | 6 | |||
| R.Heshmat 26 | 2003 | Tehran | 1573 | 615 | 958 | 2004 | 30.6 | 18.6 | 38.3 | 25-64 | 7 |
| N.Agheli 27 | 2003 | Gilan | 550 | 285 | 265 | 2005 | 19.4 | 52.8 | >30 | 6 | |
| N.Agheli 27 | 2003 | Gazvin | 550 | 274 | 276 | 2005 | 21 | 47.4 | >30 | 6 | |
| H.Bahrami 28 | 2002-2005 | Golestan | 8998 | 3787 | 5212 | 2006 | 28.4 | 17 | 36.7 | 35-81 | 7 |
| Alavi Naieiny 29 | 2004 | Isfahan | 1700 | 731 | 963 | 2006 | 21.6 | 12 | 28.9 | >60 | 5 |
| M.Mozafari 30 | 2004 | Ilam | 420 | 420 | 2006 | 22.3 | 15-49 | 5 | |||
| S.Mazloomzadeh 31 | 2004 | Zanjan | 2492 | 1251 | 1241 | 2006 | 15 | 8.9 | 21.3 | 15-64 | 7 |
| K.Hajian 32 | 2004 | Mazandaran | 3600 | 1800 | 1800 | 2007 | 18.8 | 9.9 | 27.8 | 20-70 | 6 |
| STEPS 33 | 2005 | National Survey | 89532 | 45113 | 57866 | 2007 | 19.7 | 12.7 | 27.2 | 18-64 | 7 |
| H.Farshidi 34 | 2006 | Hormozgan | 2087 | 681 | 1397 | 2006 | 12.2 | 7 | 14.7 | <63 | 6 |
| STEPS 35 | 2006 | National Survey | 29953 | 14958 | 14995 | 2008 | 15.8 | 9.9 | 21.8 | 18-64 | 7 |
Table 2. The prevalence of obesity, point estimation and 95% confidence interval classified by gender and years of data collection .
| Data Collection Years | Number of studies | Female % [95% CI] (N) | Male % [95% CI] (N) | Both % [95% CI] (N) |
| 1990-1995 | 1 | 8.0 [6.4-9.6] (1077) | 2.5 [1.9-3.1] (2301) | 4.3 [3.6-4.9] (3378) |
| 1995-2000 | 3 | 27.6 [17.7-37.5] (3597) | 11.2 [7.1-15.5] (2756) | 16.9 [9.4-24.5] (6446) |
| 2000-2005 | 25 | 27.5 [21.1-33.8] (39465) | 15.2 [12.5-17.8] (29447) | 21.3 [16.3-26.3] (77770) |
| 2005-2010 | 3 | 18.3 [11.3-25.3] (74258) | 8.6 [5.8-11.4] (60752) | 14.1 [10.5-17.6] (121572) |
| Total | 32 | 26.2 [21.3-30.5] (118397) | 12.9 [10.9-14.9] (95286) | 18.5 [15.1-21.8] (209166) |
The point, upper and lower limits was calculated by Random Model, Meta-Analysis Obesity = BMI>30 kg/m2
prevalence of obesity in women is about twice as high as men. Such a gender difference remained more or less constant during the past years. The prevalence of obesity increased sharply from 4.3% in 1990-95 to 16.9% in 1996-2000. This sharp rise was observed in both genders. Although the trend was ascending up to 2005, the overall prevalence of obesity has dropped considerably in both genders in recent years (Table 2).
Figure 1 explores the trend of reported obesity by gender and year of data collection. The figure indicates that the obesity percentage has been rising up to 30%. It remains almost constant during the next five years and finally decreases slightly (Figure 1-Total). In women, the increase in obesity had a sharper slope than men, but it finally began falling in recent years, too. The trend is similar in both gender groups (Figure 1-Female, Male).
Fig.1.
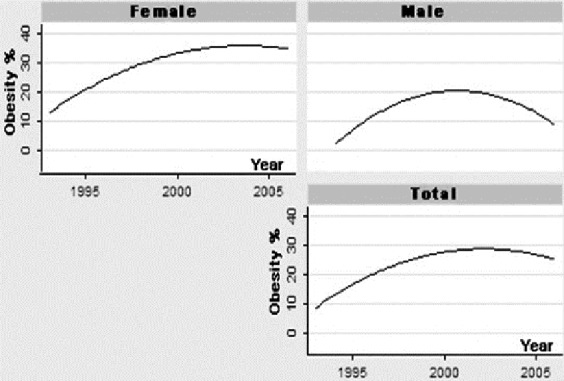
The prevalence of obesity (BMI>30 kg/m2) classified by gender Footnote: The quadratic model fitted the weighted prevalence of obesity
DISCUSSION
The peak of obesity was observed between 2000 and 2005 which were 27.5% and 15.2% in women and men, respectively. The overall prevalence of obesity was about 18%. The obesity was about twice more frequent in women compared to men and this gender difference ratio remained almost constant during the recent years. Regarding the obesity prevalence in Iran, we observe two separate periods; one begins in 1990 and lasts until 2005 during which the trend increased steadily, reaching from 4.3% to more than 21%. During this period, the percentage of obesity increased in both men and women, mainly due to rapid changes in lifestyle of Iranians from1995 to 2005.
The sharp increase in prevalence of obesity between the periods 1990-1995 and 1996-2000 (4% to 17%) may be misleading as the estimated prevalence for the years 1990 to 1995 comes from only one study conducted in Fars. This is definitely not representative of the whole country and cannot be extrapolated as the prevalence of obesity in the entire nation.
In recent years, we observe extensive campaigns in Iran run by the Ministry of Health, mass media and other organizations which might be due to the rapid increase of obesity and its complications in the past decade. Although it is very difficult to state a clear conclusion, the drop in the prevalence of obesity in recent years might be due to the impact of these campaigns. It seems that such population based public health interventions constitute one of the reasonable bases of the decline in obesity prevalence in recent years. An alternative explanation is a rapid change in the population structure. Currently, Iran has one of the youngest populations worldwide with more than 55% aged less than 40 years. While this young population is not at risk of obesity for the time being, the inevitable aging which will ensue over the coming years will bring about a rapid increase in non-communicable diseases and their related risk factors such as obesity.
Based on the data available, the worldwide prevalence of obesity varies from less than 5% in rural China, Japan and some African countries to as high as 75% of the adult population in urban Samoa.36, 37 Obesity levels also vary depending on ethnicity. In the USA, there were considerable variations in the prevalence of obesity particularly among women from different ethnical groups.38 Similarly, we found large variations in the reported obesity prevalence. Indeed, such variations are expected in Iran where more than 70 million people live in 30 provinces with different socioeconomic conditions, lifestyles and health status.5
Our findings clearly indicate that the risk of obesity is greater in women. This difference might be partly attributed to women’s tendency to be less active physically in their daily life. Based on three rounds of national surveys,WHO STEPs approach for non-communicable disease risk factors, physical activities in women was much less than men; in all categories of physical activity, women had reported lower levels of physical activity.33, 35
Popkin and Doak (1998) used data from eight mid- and low income countries that had at least two surveys to estimate trends, reporting increases of 2.3% to 19.6% in obesity (BMI≥30 kg/m2) prevalence over a 10-year period.39 In our study, the prevalence of obesity in adults was about 18.5% which is comparable to other mid-to low income countries. It may be strongly indicated that that our
population is also at risk of obesity.
The eligible studies used different age cutoff points to categorize their findings. These differences were one of the main challenges in summarizing the findings to estimate the best representative age-specific prevalence of obesity. In addition, some papers did not present their findings in details, particularly in subgroups, and we were unable to obtain more information by direct contact with the authors.
In conclusion, we found that the risk of obesity was approximately twice greater in women compared to men. In addition, it seems that the very sharp increase in risk of obesity in past 20 years has been reversing in recent years.
CONFLICT OF INTEREST
The authors declare no conflict of interest related to this work.
Appendix
Appendix - Critical Appraisal Tool
| Articles | Reviewer □1 □2 | ||||
|---|---|---|---|---|---|
| STEP1. Primary Evaluation | 1 | 2 | 3 | 4 | 5 |
| Please do this by reading the title/abstract |
□Reject
□Accept |
□Reject
□Accept |
□Reject
□Accept |
□Reject
□Accept |
□Reject
□Accept |
| STEP2. Read the full text deeply and score those articles pass the primary evaluation | |||||
| 1. Random sample or whole population | |||||
| 2. Unbiased sampling frame (i.e. census data) | |||||
| 3. Adequate sample size (>300 subjects) | |||||
| 4. Standards measures were used? | |||||
| 5. Outcomes measured by unbiased assessors | |||||
| 6. Adequate response rate (70%), refusals described | |||||
| 7. Confidence intervals, subgroup analysis | |||||
| Total score | |||||
| Final decision |
□Reject
□Accept |
□Reject
□Accept |
□Reject
□Accept |
□Reject
□Accept |
□Reject
□Accept |
| If the article meets the criteria, put score 1 in the cell. | |||||
| Articles with total score more than 5 are accepted in the study | |||||
Please cite this paper as:
Mirzazadeh A, Salimzadeh H, Arabi M, Navadeh S, Hajarizadeh B, Haghdoost AA.Trends of Obesity in Iranian Adults from 1990s to late 2000s; a Systematic Review and Meta-analysis. Middle East J Dig Dis 2013;5:151-7.
References
- 1. World Health Organization. Obesity and overweight Fact sheet N 311, http://www.who.int/mediacentre/factsheets/fs311/en/ Updated March 2013.
- 2.Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB. Years of Life Lost Due to Obesity. JAMA. 2003;289:187–93. doi: 10.1001/jama.289.2.187. [DOI] [PubMed] [Google Scholar]
- 3.Caballero B. A Nutrition Paradox - Underweight and Obesity in Developing Countries. N Engl J Med. 2005;352:1514–6. doi: 10.1056/NEJMp048310. [DOI] [PubMed] [Google Scholar]
- 4.Urek R, Crncevic-Urek M, Cubrilo-Turek M. [Obesity--a global public health problem] Acta Med Croatica. 2007;61:161–4. [PubMed] [Google Scholar]
- 5. Iran statistic yearbook: 2006 Tehran: Statistical Center of Iran Statistical Center of Iran; 2006.
- 6.Pishdad GR. Overweight and obesity in adults aged 20-74 in southern Iran. Int J Obes Relat Metab Disord. 1996;20:963–5. [PubMed] [Google Scholar]
- 7.Barzigar A, Shojaei Tehrani H. Prevalence of atherosclerosis risk factors in Sowme Sara district of Gilan in 1996. J Kerman Unive Med Sci. 1997;4:182–9. [Google Scholar]
- 8.Gorbani R, Nazari A. The prevalence of obesity and it's determining factors among the 20-55 years old residents in Semnan in 1996. J Semnan Univ of medical sciences. 1997;1:19–24. [Google Scholar]
- 9.Azizi F, Azadbakht L, Mirmiran P. Trends in Overweight, Obesity and Central Fat Accumulation among Tehranian Adults between 1998-1999 and 2001-2002: Tehran Lipid and Glucose Study. Ann Nutr Metab. 2005;49:3–8. doi: 10.1159/000084171. [DOI] [PubMed] [Google Scholar]
- 10.Jamshidian Tehrani M, Kalantari N, Azad Bakht L, Esmail Zadeh A, Rajaei A, Houshiar Rad A. et al. Osteoporosis risk factors in Tehrani women aged 40-60 years. Iran J Endocrinol Metabol. 2004;6:139–45. [Google Scholar]
- 11.Soori H. Pattern of dietary behavior and obesity in Ahwaz, Islamic Republic of Iran. East Mediterr Health J. 2001;7:163–70. [PubMed] [Google Scholar]
- 12.Mojibian M, Ghilian Z. Prevalence of obesity among women in Yazd city in 2000. J Shahid Sadoughi Univ Med Sci Health Services. 2001;9:36–42. [Google Scholar]
- 13.Azizi T, Harati H, Mir Bolooki M, Saadat N, Azizi F. Association of different anthropometric measures and type 2 diabetes in an Iranian urban population. Iran J Endocrinol Metabol. 2005;7:103–10. [Google Scholar]
- 14.Mortazavi Z, Shahrakipoor M. Body Mass Index in Zahedan University Of Medical Sciences Students. Tabib e Shargh. 2002;4:81–6. [Google Scholar]
- 15. Akhavan Tabib A, Kelishadi R, Sadri G, Sabet B, Toluei H, Baghaei A. Heathy Heard Program: Obesity in center of Iran. J Qazvin Univ of Med Sci 2003:27-35.
- 16.Sezavar H, Mohammadi MA. Prevalence of obesity and its association with cardiovascular risk factors in Ardabil city in 2000. J Ardabil Univ Med Sci. 2001;2:21–6. [Google Scholar]
- 17.Kavian F, Kimiagar M, Golestan B, Hoshiar Rad A. The prevalence of obesity and body fat distribution among females workers in Shaheed Beheshti University of Medical Sciences Pajouhandeh J 2002;25:459-63. The prevalence of obesity and body fat distribution among females workers in Shaheed Beheshti University of Medical Sciences Pajouhandeh J. 2002;25:459–63. [Google Scholar]
- 18. Safari SM, Sheikh Aleslam R, Abdolahi Z, Naghavi M, Sadeghi S, editors. The prevelance of over-weight and obesity among elderly individuals in spring 2001. The 9th congress of nutrition in Iran; 2006.
- 19. The ministry of Health and Medical Education. Research in Micro-nutrient in Iran. Tehran; 2005.
- 20.Azizi F, Emami H, Salehi P, Ghanbarian A, Mirmiran P, Mirboloki M. Risk factors of cardiovascular diseases among elderly in Tehran (Tehran Lipid and Glucose Study) Iran J Endocrinol Metabol. 2002;5:3–14. [Google Scholar]
- 21.Fakhrzadeh H, Batoei M, Faridnia P, Taeb M. Overweight and obesity in oil industry workers on Kharg Island. Iran South Med J. 2002;1:73–81. [Google Scholar]
- 22.Akbari S. The prevalence of obesity and its association with unovolation in female students of Khoram Abad high-schools. Yafteh. 2003;4:33–8. [Google Scholar]
- 23.Mostafavi H, Dabagh Manesh M, Zare N. Prevalence of obesity and over weight in adolescents and adult population in Shiraz. Iran J Endocrinol and Metabol. 2005;25:57–66. [Google Scholar]
- 24.Rahmati F, MoghadasTabrizi Y, Shidfar F, Jafari M. Prevalence of obesity and hypertension among Tehran university students. Payesh. 2004;3:123–30. [Google Scholar]
- 25.Vaghari GR. Obesity among mothers in rural golestan. J School Public Health Institude Res. 2004;3:21–8. [Google Scholar]
- 26.Heshmat R, Fakhr Zadeh H, Pour-Ebrahim R, Nouri M, Aala Adini F. Cardiovascular risk factors study in the inhibitants of Tehran university of medical sciences population lab : statistical design and sampling. Iran J Diabetes Lipid Dis. 2004;3:21–6. [Google Scholar]
- 27.Agheli N, Assef Zadeh S, Rajabi M. The prevalence of cardiovascular risk factors among population aged over 30 years in Rasht and Qazvin. J Qazvin Univ of Med Sci. 2005;35:59–65. [Google Scholar]
- 28.Bahrami H, Sadatsafavi M, Pourshams A, Kamangar F, Nouraei M, Semnani S. et al. Obesity and hypertension in an Iranian cohort study; Iranian women experience higher rates of obesity and hypertension than American women. BMC Public Health. 2006;6:1–9. doi: 10.1186/1471-2458-6-158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Alavi Naieny AM, Dorosti motlagh AR, Aghdak P. Survey of obesity, underweight and associated factors in elderly people, using some of anthropometric indices in Isfahan city, 2004. J Mazandaran Univ Med Sci. 2006;16:117–23. [Google Scholar]
- 30.Mozafari M, Nosrati S, Purmansour G, Rezaei M. Factors affecting the prevalence of obesity among 15-49 years old women referred to urban health clinics in Ilam in 2004. J Ilam Univ Med Sci. 2006;14:8–17. [Google Scholar]
- 31.Mazloomzadeh S, Moosavi Viri A, Dinmohamadi H. Epidemiology of overweight and obesity in Zanjan province in 2005. J Zanjan Med Univ. 2004;14:57–64. [Google Scholar]
- 32.Hajian-Tilaki KO, Heidari B. Prevalence of obesity, central obesity and the associated factors in urban population aged 20–70 years, in the north of Iran: a population-based study and regression approach. Obes Rev. 2007;8:3–10. doi: 10.1111/j.1467-789X.2006.00235.x. [DOI] [PubMed] [Google Scholar]
- 33. The ministry of Health and Medical Education. WHO STEPs appraoch on non-comunicable disease; Iran - round 1. 2007.
- 34.Farshidi H, Zare S, Booshehri E. Association of different anthropometric measures and blood pressure in adult population of Bandar-Abbas city. Hormozgan Med J. 2006;10:111–8. [Google Scholar]
- 35. The ministry of Health and Medical Education. WHO STEPs approach on non-comunicable disease; Iran - round 2. 2008.
- 36.Caballero B. Symposium: Obesity in Developing Countries: Biological and Ecological Factors. J Nutr. 2001;131:866S–70S. doi: 10.1093/jn/131.3.866S. [DOI] [PubMed] [Google Scholar]
- 37.Caballero B. A Nutrition Paradox: Underweight and Obesity in Developing Countries. N Engl J Med. 2005;352:1514–16. doi: 10.1056/NEJMp048310. [DOI] [PubMed] [Google Scholar]
- 38.Goulding A, Grant AM, Taylor RW, Williams SM, Parnell WR, Wilson N. et al. Ethnic differences in extreme obesity. J Pediatr. 2007;151:542–4. doi: 10.1016/j.jpeds.2007.07.011. [DOI] [PubMed] [Google Scholar]
- 39.Popkin BM, Doak CM. The obesity epidemic is a worldwide phenomenon. Nutr Rev. 1998;56:106–14. doi: 10.1111/j.1753-4887.1998.tb01722.x. [DOI] [PubMed] [Google Scholar]