

Abstract
The hypothalamus has been implicated in migraine based on the manifestation of autonomic symptoms with the disease, as well as neuroimaging evidence of hypothalamic activation during attacks. Our objective was to determine functional connectivity (FC) changes between the hypothalamus and the rest of the brain in migraine patients vs. control subjects. This study uses fMRI (functional magnetic resonance imaging) to acquire resting state scans in 12 interictal migraine patients and 12 healthy matched controls. Hypothalamic connectivity seeds were anatomically defined based on high-resolution structural scans, and FC was assessed in the resting state scans. Migraine patients had increased hypothalamic FC with a number of brain regions involved in regulation of autonomic functions, including the locus coeruleus, caudate, parahippocampal gyrus, cerebellum, and the temporal pole. Stronger functional connections between the hypothalamus and brain areas that regulate sympathetic and parasympathetic functions may explain some of the hypothalamic-mediated autonomic symptoms that accompany or precede migraine attacks.
Introduction
Migraine, a common neurological disorder, is characterized by episodic headache attacks, and is frequently accompanied by nausea, vomiting, hunger, yawning, thirst, photophobia, phonophobia, and/or sleep disorders [1], [2]. In addition, conjunctival injection, lacrimation, nasal congestion, rhinorrhoea, eyelid edema and forehead/facial sweating are also common in migraineurs [3]. These symptoms implicate alterations in brain autonomic systems.
By regulating many sympathetic and parasympathetic responses, the hypothalamus is thought to heavily involved in physiological functions such as food ingestion, energy balance, stress, circadian rhythms, arousal, and autonomic responses to pain. The central role of the hypothalamus in regulating autonomic functions and homeostasis suggests that it may underlie some autonomic symptoms associated with migraine [2], [4]–[7] or its prodromal phase [4], [5], [7], [8]. Evidence linking the hypothalamus to migraine include (a) imaging data showing that the hypothalamus is activated during spontaneous migraine without aura [9], (b) prevalence of obesity among chronic migraineures [5], [6], [10], (c) the cyclic nature of the condition [11], and (d) its greater prevalence in women after puberty and in homosexual men [12]–[14]. Partially responsible for changes in hypothalamic functions may be attributed to the large input it receives from ascending trigeminovascular neurons in the spinal trigeminal nucleus [7]. The cyclic nature of the disease relates to how repetitive processes including hormonal cycle in women or the sleep-wake cycle [15] may alter allostatic load in the disease [16].
While the hypothalamus appears to be an important structure in migraine, imaging studies have yet to explicitly evaluate whether the hypothalamus has altered functional processing during the interictal state. One approach is to evaluate changes in functional connectivity of this structure in patients compared with healthy controls. In fMRI, functional connectivity (FC) is defined as temporal correlations between spatially remote neurophysiological events or functional interactions [17]. Given that the hypothalamus may be significantly involved in migraine attacks, we hypothesized that fMRI FC between the hypothalamus and autonomic processing areas in the brain are enhanced in interictal migraine patients as compared with healthy control subjects. As such, the alteration in FC would not only reflect the effects of repeated activation in the migraine attack, but potentially represent a sensitization of the functional connections between the hypothalamus and other brain structures involved in autonomic function.
Materials and Methods
Using fMRI, we recorded blood oxygen level dependent (BOLD) signal fluctuations during resting state in 12 episodic migraine patients and 12 healthy age- and gender-matched control subjects.
Ethics Statement
This study was approved by the McLean Hospital Institutional Review Board, and met the scientific and ethical guidelines for human research of the Helsinki Accord (http://ohsr.od.nih.gov/guidelines/helsinki.html). All patients and subjects provided written informed consent to participate in this study.
Subjects
Episodic migraine patients (9 females, 3 males; 31·7±7·6 years old; Table 1 ) were free of neurological and other sensory dysfunctions. The patients included in the study had acute intermittent migraine without aura as defined by the International Headache Society (<14 attacks/month). Subjects were not having a migraine attack at least 72 hours prior to testing. In addition no patient had a migraine precipitated during or on the day following the baseline scan.
Table 1. Subject demographics.
| Age | Sex | Freq | Onset | Side | Pain w/o med | Pain w/med | Medications | |
| Patients | ||||||||
| M1 | 31.9 | M | 1/mo | 15 yrs | B | 9 | 4 | Acetaminophen, Ibuprofen |
| M2 | 49 | F | 5/mo | 39 yrs | U | 10 | 0 | Sumatriptan, Lisinopril |
| M3 | 36.3 | F | 1/mo | 33 yrs | L | 10 | 9 | Aspirin, Acetaminophen, Ibuprofen |
| M4 | 24.8 | F | 7–8/mo | 8 yrs | B | 8 | 4 | Amitriptyline, Atenolol, Acetaminophen, Naproxen, Rizatriptan |
| M5 | 22.9 | F | 3–4/mo | 7 yrs | B | 10 | 7 | Acetaminophen, Ibuprofen |
| M6 | 25.7 | F | 3–4/mo | 7 yrs | B | 10 | 10 | Ibuprofen |
| M7 | 32.1 | F | 2–4/mo | 21 yrs | U | 7 | 6 | None |
| M8 | 37.6 | M | 2/mo | 32 yrs | R | 10 | 9 | None |
| M9 | 24.6 | F | 1/mo | 4 yrs | L | 10 | 6 | Acetaminophen |
| M10 | 26.8 | M | 5/mo | 3 yrs | B | 5–6 | N/A | None |
| M11 | 38.8 | F | 2/mo | 28 yrs | U | 9–10 | 4 | Ibuprofen, Midrin |
| M12 | 30.2 | F | 1–3/mo | 8 yrs | R | 7 | 7 | Rizatriptan |
| Healthy Controls | ||||||||
| H1 | 32.2 | M | – | – | – | – | – | – |
| H2 | 27.9 | F | – | – | – | – | – | – |
| H3 | 24.5 | F | – | – | – | – | – | – |
| H4 | 23.3 | F | – | – | – | – | – | – |
| H5 | 36.9 | F | – | – | – | – | – | – |
| H6 | 26.4 | F | – | – | – | – | – | – |
| H7 | 38 | M | – | – | – | – | – | – |
| H8 | 30.8 | F | – | – | – | – | – | – |
| H9 | 24.3 | M | – | – | – | – | – | – |
| H10 | 31.6 | F | – | – | – | – | – | – |
| H11 | 36.3 | M | – | – | – | – | – | – |
| H12 | 49 | F | – | – | – | – | – | – |
Key: “Side” = the laterality of migraine attacks (B = Bilateral, L = Left unilateral, R = Right unilateral, U = Unilateral, alternating sides); “Pain w/o med” = average pain intensity reported during a migraine attack when no abortive medication is taken. Pain intensity was reported using a numeric rating scale from 0–10; “Pain w/med” = the average pain intensity reported during a migraine attack when abortive medication is taken. Freq = headache days per month.
Subjects verbally rated the pain intensity of their average migraine as a 5 or higher on a 0–10 scale, with 10 being the most intense pain imaginable. For those patients taking daily medications (e.g., preventive as opposed to acute medications to abort the attack), patients abstained from taking their migraine medications for one dosing interval prior to their scheduled scan session. Age- and gender-matched healthy subjects (8 females, 4 males; 31·7±7·2 years old) were also tested. Gender-matching was not exact, as the control group had one more male (and one less female) than the patient group.
MR Acquisition
Imaging was conducted using a 3T Siemens Tim Trio scanner with a quadrature head coil. T1-weighted structural images were acquired using a 3D magnetization-prepared rapid gradient echo sequence (MPRAGE - 128 1.3 mm-thick slices with an in-plane resolution of 1 mm (256×256)). For functional resting state scans, a Gradient Echo (GE) echo planar imaging (EPI) sequence with TE/TR = 30/2000 was performed, with three hundred volumes captured for each scan. Each functional scan consisted of 34 slices oriented in an oblique plane to match the brainstem axis. Slices were 4.0 mm thick with an in-plane resolution of 3.5 mm (64×64). During these resting state scans, subjects were instructed to stay awake and to keep their eyes open.
Image Analysis
Functional imaging datasets were processed and analyzed using scripts within FSL (FMRIB’s Software Library, www.fmrib.ox.ac.uk/fsl) [18]. The initial two volumes were removed from each of the functional scans to allow for signal equilibration. Visual screening of the functional volumes revealed that none of the subjects showed indications of gross movement (>1 voxel). The skull and other non-brain areas were extracted from the anatomical and functional scans using FSL’s script Brain Extraction Tool (BET). Motion Correction using FMRIB’s Linear Image Registration Tool (MCFLIRT) was performed on each functional scan. All volumes were mean-based intensity normalized by the same factor. The volumes were spatially smoothed with a 5 mm full-width at half-maximum (FWHM) filter, and a 150 s high-pass temporal filter was applied. These functional images were then co-registered with the anatomical images using FMRIB’s Linear Image Registration Tool (FLIRT), which uses an automated affine registration algorithm.
The hypothalamus was identified for each subject based on anatomical landmarks in the MPRAGE as described previously ( Figure 1 ) [19]. A bilateral hypothalamic mask was conservatively defined for each subject using the following criteria: (1) the anterior extent was limited by the anterior commissure; (2) the inferior extent was limited by the mammillary bodies and optic tracts; (3) the posterior extent was limited by the mammillary bodies; (4) the medial extent was limited by the third ventricle; and (5) the region of interest extended 8 mm laterally from the medial extent.
Figure 1. Hypothalamus seeds across subjects registered to the MNI152 standard brain.
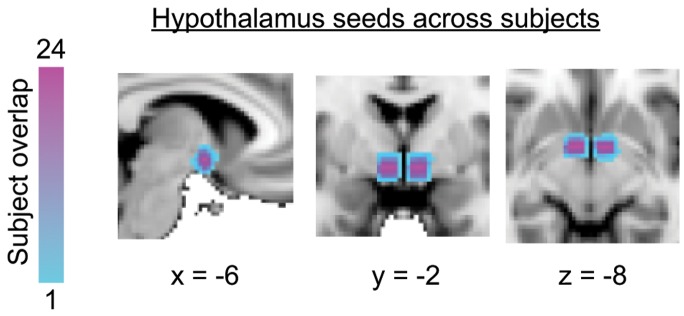
Anatomical boundaries for each subject were based on Saleem et al., 2007 (see Methods for details).
First-level functional connectivity analysis of single subject data was performed using FMRI Expert Analysis Tool using FMRIB’s Improved Linear Model (FEAT FILM) Version 6.00 with local autocorrelation correction [20]. For single subject analysis, the mean time course for each corresponding hypothalamic mask was calculated, and entered as an explanatory variable (EV). Eight additional covariates of no interest were included that modeled motion (3 directions for rotation, 3 directions for translation), and the mean signal time courses measured in white matter and cerebrospinal fluid, as segmented by FMRIB’s Automated Segmentation Tool (FAST). The temporal derivative of the time course was not included as an explanatory variable. Subjects were spatially normalized to the MNI152 brain for group analysis.
Group functional connectivity maps were generated by fMRI expert analysis tool (FEAT) fMRIB’s Local Analysis of Mixed Effects (FLAME). A mixed effects contrast analysis was performed to compare migraine vs. control group functional connectivity. Statistical parametric maps were thresholded using Gaussian Mixture Modeling (GMM) [21], a multiple comparisons-based analysis which has previously been used in the context of detecting functional connectivity in brain imaging [22], [23]. A minimum cluster criterion of 7 voxels in original space (0.30 cm3) was implemented to identify significant clusters.
Results
Subjects
Twelve patients and twelve matched healthy controls were successfully scanned. All patients were had episodic migraine without aura. None were on preventive medications ( Table 1 ). Medication use was either NSAIDs and/or triptans.
Functional Measures
A mixed effects contrast analysis was performed to compare migraine vs. control group functional connectivity showed significant differences in a number of areas (details below).
Hypothalamic Functional Connectivity
Widespread differences in hypothalamic functional connectivity were detected in migraine patients vs. healthy control subjects. The majority of these differences occurred in brain regions related to sympathetic and/or parasympathetic nervous system processing, with migraine patients showing greater functional connectivity with these structures ( Figure 2 ; Table 2 ). A neuroimaging meta-analysis of the central processing of autonomic function indicates that these regions can be categorized as sympathetic or parasympathetic nervous system structures [24], and are labeled accordingly in Figure 2 .
Figure 2. Increased hypothalamic functional connectivity in migraine-healthy controls in parasympathetic and sympathetic nervous system brain structures.

Functional connectivity contrast maps were thresholded at a posterior probability of p>0.5 using GMM. Contrast maps overlay the standard MNI152 whole-brain atlas. PNS = parasympathetic nervous system, SNS = sympathetic nervous system. In reference to coordinates, x = sagittal (posterior-anterior, from left to right of the image), y = coronal (right-left), and z = axial planes (right-left).
Table 2. Brain regions with increased hypothalamic functional connectivity in migraine patients vs. healthy control subjects.
| Brain Region | Lat. | z-stat | X | Y | Z | Vol (cm3) |
| Frontal | ||||||
| PrCG | R | 3.0019 | 6 | −32 | 72 | 0.35 |
| MFG | R | 2.8577 | 44 | 22 | 44 | 0.41 |
| Parietal | ||||||
| SPL/SMG | L | 2.8535 | −46 | −44 | 58 | 0.34 |
| Temporal | ||||||
| ITG | L | 3.7500 | −50 | 0 | −38 | 0.31 |
| Planum Polare | R | 3.6963 | 46 | −4 | −16 | 0.66 |
| TmP | L | 3.6501 | −36 | 6 | −22 | 0.41 |
| MTG | L | 3.1737 | −58 | −10 | −26 | 0.46 |
| L | 2.9026 | −58 | −12 | −14 | 0.73 | |
| PHG | L | 3.1445 | −22 | −16 | −28 | 0.42 |
| L | 2.8751 | −22 | −12 | −34 | 0.33 | |
| STG | L | 3.1319 | −62 | −30 | 0 | 0.76 |
| Hippocampus | R | 3.0327 | 44 | −16 | −24 | 0.3 |
| L | 2.9341 | −48 | −22 | −22 | 0.46 | |
| Sub-Cortical | ||||||
| Caudate | L | 2.8124 | −16 | −4 | 24 | 0.5 |
| Brainstem/Cerebellum | ||||||
| Nucleus coeruleus | R | 3.4440 | 8 | −34 | −26 | 0.58 |
| PN | L | 3.5626 | −8 | −24 | −42 | 0.59 |
| R | 2.9397 | 8 | −20 | −40 | 0.79 | |
| R | 3.0793 | 6 | −26 | −42 | 0.54 | |
| Cerebellum | ||||||
| Cr I/II | L | 3.3418 | −40 | −50 | −48 | 0.85 |
| V | L | 3.2582 | −12 | −50 | −14 | 0.78 |
| R | 3.2184 | 14 | −46 | −16 | 0.52 | |
| R | 3.1642 | 12 | −52 | −20 | 1.19 | |
| R | 3.0691 | 6 | −60 | −22 | 0.86 | |
| L | 2.8326 | −10 | −60 | −8 | 0.45 | |
| Verm VIIIa/VIIIb | L | 3.2080 | −2 | −62 | −36 | 0.33 |
| Dentate nucleus | L | 3.1411 | −24 | −50 | −34 | 0.36 |
| IX | R | 3.0394 | 8 | −46 | −46 | 0.43 |
| V/VI | R | 2.8944 | 12 | −58 | −18 | 0.35 |
Legend: Cr I/II = Crus I and II; ITG = inferior temporal gyrus; IX = hemispheric lobule IX; MFG = middle frontal gyrus; PHG = parahippocampal gyrus; PN = pontine nuclei; PrCG = precentral gyrus; SMG = supramarginal gyrus; SPL = superior parietal lobule; STG = superior temporal gyrus; TmP = temporal pole; V = hemispheric lobule V; V/VI = hemispheric lobules V and VI; Verm VIIIa/VIIIb = Vermal lobules VIIIa/VIIIb.
Migraineurs showed enhanced functional connectivity with the hypothalamus in subcortical structures and throughout the temporal lobe ( Figure 2 ). Areas of note included the nucleus coeruleus (volume: 0.58 cc, z-statistic: 3.44) pontine nuclei (volume: 1.92 cc, z-statistic: 9.58), caudate (volume: 0.50 cc, z-statistic: 2.81), cerebellar Crus I and II (volume: 0.85 cc, z-statistic: 3.34), temporal pole (volume: 0.41 cc, z-statistic: 3.65), superior temporal gyrus (volume: 0.76 cc, z-statistic: 3.13), hippocampus (volume: 0.76 cc, z-statistic: 5.97), and parahippocampal gyrus (volume: 0.75 cc, z-statistic: 6.02) ( Table 2 ). Of these, the locus coeruleus and other pontine nuclei are of particular interest because of their role in stress and in the case of the locus coeruleus, as a major source of norepinephrine and has an excitatory effect on numerous brain regions including subcortical (e.g., amygdala, thalamus) and cortical structures [25], in addition to the hypothalamus and thus involved in autonomic function [26]. We interpret increased functional connectivity as enhanced or sensitized interactions between the hypothalamus and these structures. Conversely, migraineurs showed decreased functional connectivity localized to frontal and occipital lobe structures. These areas included the precentral gyrus (volume: 1.76 cc, z-statistic: 7.81), frontal pole (volume: 1.43 cc, z-statistic: 11.13), paracingulate gyrus (volume: 0.34 cc, z-statistic: 3.25), superior frontal gyrus (volume: 0.32 cc, z-statistic: 2.95), fusiform gyrus (volume: 0.46 cc, z-statistic: 4.20), and lingual gyrus (volume: 0.74 cc, z-statistic: 7.04) ( Table 3 ). Here, decreased connectivity is interpreted and lower or diminished interactions or neural communications between the hypothalamus and structures noted.
Table 3. Brain regions with decreased hypothalamic functional connectivity in migraine patients vs. healthy control subjects.
| Brain Region | Lat. | z-stat | X | Y | Z | Vol (cm3) |
| Frontal | ||||||
| PrCG | R | 3.9425 | 48 | 4 | 34 | 1.34 |
| R | 3.872 | 24 | −10 | 60 | 0.42 | |
| FrPole | L | 3.8249 | −40 | 38 | 16 | 0.41 |
| L | 3.6729 | −34 | 44 | 20 | 0.58 | |
| L | 3.6329 | −28 | 38 | 28 | 0.44 | |
| ParaCG | L | 3.2542 | −4 | 40 | 32 | 0.34 |
| SFG | R | 2.9452 | 18 | −2 | 64 | 0.32 |
| Occipital | ||||||
| Fusiform G | R | 4.2019 | 16 | −78 | −12 | 0.46 |
| Lingual G | L | 3.7044 | −4 | −84 | 0 | 0.43 |
| L | 3.3314 | 4 | −86 | −8 | 0.31 |
Legend: FrPole = frontal pole; ParaCG = paracingulate gyrus; PrCG = precentral gyrus; SFG = superior frontal gyrus.
Discussion
This study found that interictal migraineurs have enhanced functional connectivity (FC) between the hypothalamus and brain structures related to autonomic function. Enhanced connectivity was observed to overlap with central representations of autonomic nervous system function, which has recently been characterized in a neuroimaging meta-analysis [24]. Our findings imply that these autonomic connections are sensitized in migraine patients, perhaps leading to increased autonomic symptoms associated with ictal events in migraine. As discussed below, anatomical correlates between the hypothalamus and the regions noted are present.
Hypothalamo-Sympathetic FC
In migraineurs, the hypothalamus demonstrated increased functional connectivity with sympathetic nervous system structures, such as the parahippocampal gyrus and cerebellar Crus I and II. The hypothalamus is structurally connected to the hippocampus through the fornix [27], and to the cerebellum through hypothalamo-cerebellar connections [28]. Enhanced connectivity with these sympathetic structures may prime cortical responses to external stressors relating to anxiety, memory, spatial location, and aversive stimuli [29]–[31]. BOLD signals in these hippocampal and cerebellar regions have also previously been found to co-vary with sympathetic activity in the form of skin blood flow measures and skin conductance response [32]. In this previous experiment, sympathetic responses were elicited using an aversive conditioning paradigm and measured during anticipation of noxious heat and the painful experience itself. While the authors acknowledged a potential confound between sympathetic responses with motor tasks and sensory stimuli in their data, we were able to see a hypothalamic link with these structures at rest without confounds stemming from explicit motor tasks or sensory stimuli.
Hypothalamo-Parasympathetic FC
Migraineurs also showed increased hypothalamic connectivity with parasympathetic nervous system structures, including the temporal pole, superior temporal gyrus, and cerebellar lobules V and VI. Structural connectivity between these areas and the hypothalamus has been established previously [28], [33]. We have shown recently that the temporal pole is hyperexcitable in migraine patients [22]. This structure, along with the superior temporal pole, may be involved in the interictal hypersensitivity to smell and light [34], [35]. Cerebellar lobules V and VI have been related to a wide variety of tasks, including cognitive and emotional processing [31], [36]. The enhanced functional connectivity between the hypothalamus and these parasympathetic brain regions allows them to interact in ways that may impact interoceptive processes in migraine patients.
Locus Coeruleus and Caudate Nucleus
Structures related to both sympathetic and parasympathetic processing, such as the locus coeruleus (LC), also exhibited increased hypothalamic connectivity. The LC is the largest noradrenergic nucleus in the brain. Through heavy innervation of multiple forebrain regions including the hypothalamus [25], [26], it is involved in number of vital functions including wakefulness [37], responses to stress [38], and regulation of emotion [39]. Although a specific role in migraine is unknown, LC involvement in the inhibition of nociceptive reflexes [40] and firing mode of thalamic and prefrontal cortex neurons in response to noxious stimuli [41] raise the possibility that it may also be involved in normal (and perhaps abnormal) pain modulation during migraine.
Another structure showing altered hypothalamic FC that is implicated in sympathetic and parasympathetic function is the caudate nucleus. Efferent connections between the hypothalamus and the caudate have been shown in tracing studies in the rat [42]. The caudate has also recently been associated with arousal [43], but is also related to motivation, learning and memory, and pain and sensory processing [44], [45]. Increased hypothalamic connectivity with these structures may be responsible for the recurring chronobiological features of migraine [1], [2] and appetitive drive [46].
The data indicates decreased functional connectivity with a number of brain regions of migraineurs vs. healthy controls ( Table 3 ). These include cortical regions in the frontal and occipital regions. Hypothalamic connections to the frontal lobes have been documented in monkeys [47]. While unknown, the decreased FC between frontal regions may be specific to diminished defined functions. For example, these may be anti-correlated (potentially related to parasympathetic processes) to sympathetic hypothalamic drive [24], [48]. Furthermore, regions such as the fusiform gyrus, also showing diminished decreased functional connectivity with the hypothalamus may relate to autonomic responses to emotional stimuli [49].
The study did not differentiate between migraine patients with and without aura. Migraine with aura is a more aggressive disease, at least based on observed brain changes [50]. Based on alterations in autonomic function in patients reported with aura [51], [52] we would expect that such patients would have functional connectivity further diminished when compared with migraineurs without aura.
Conclusions
While the resting state connectivity data suggests that the hypothalamus has widespread influence on autonomic nervous system structures in migraine patients, it does not necessarily indicate that the hypothalamus has a central role in generating migraines. The connectivity results are correlative, and the inference of functional impact is based on previous studies. However, the results do indicate that changes in hypothalamic connectivity are a central feature in migraine patients, and may be responsible for the manifestation of autonomic symptoms. While other autonomic brain systems must clearly play a role in migraine, only those areas noted in the results showed differences between healthy subjects and controls for the resting state data acquired. Thus, measures of hypothalamic hyperactivity to a stressor (e.g., heat or a migraine attack) or measures of hypothalamic hormones would contribute to our understanding of the structure in the migraine condition.
Acknowledgments
We thank Lauren Nutile and Gabi Barmettler for recruiting, scheduling and scanning patients and Nasim Maleki for helping with imaging. We would like to thank Rosanna Veggeberg for her help retrieving patient records.
Funding Statement
This work was supported by the National Institutes of Health (R01NS073997 to D.B., K24NS0624050 to D.B.); the L Herlands fund to the P.A.I.N. Group (D.B., L.B.). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. Dodick DW, Eross EJ, Parish JM, Silber M (2003) Clinical, anatomical, and physiologic relationship between sleep and headache. Headache 43: 282–292. [DOI] [PubMed] [Google Scholar]
- 2. Cortelli P, Pierangeli G (2007) Hypothalamus and headaches. Neurol Sci 28 Suppl 2S198–202. [DOI] [PubMed] [Google Scholar]
- 3. Lai TH, Fuh JL, Wang SJ (2009) Cranial autonomic symptoms in migraine: characteristics and comparison with cluster headache. J Neurol Neurosurg Psychiatry 80: 1116–1119. [DOI] [PubMed] [Google Scholar]
- 4. Alstadhaug KB (2009) Migraine and the hypothalamus. Cephalalgia 29: 809–817. [DOI] [PubMed] [Google Scholar]
- 5. Holland P, Goadsby PJ (2007) The hypothalamic orexinergic system: pain and primary headaches. Headache 47: 951–962. [DOI] [PubMed] [Google Scholar]
- 6. Akerman S, Holland PR, Goadsby PJ (2011) Diencephalic and brainstem mechanisms in migraine. Nat Rev Neurosci 12: 570–584. [DOI] [PubMed] [Google Scholar]
- 7. Burstein R, Jakubowski M (2005) Unitary hypothesis for multiple triggers of the pain and strain of migraine. J Comp Neurol 493: 9–14. [DOI] [PubMed] [Google Scholar]
- 8. Overeem S, van Vilet JA, Lammers GJ, Zitman FG, Swaab DF, et al. (2002) The hypothalamus in episodic brain disorders. Lancet Neurol 1: 437–444. [DOI] [PubMed] [Google Scholar]
- 9. Denuelle M, Fabre N, Payoux P, Chollet F, Geraud G (2007) Hypothalamic activation in spontaneous migraine attacks. Headache 47: 1418–1426. [DOI] [PubMed] [Google Scholar]
- 10. Peterlin BL, Rapoport AM, Kurth T (2010) Migraine and obesity: epidemiology, mechanisms, and implications. Headache 50: 631–648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Stankewitz A, Aderjan D, Eippert F, May A (2011) Trigeminal nociceptive transmission in migraineurs predicts migraine attacks. J Neurosci 31: 1937–1943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Stewart WF, Shechter A, Rasmussen BK (1994) Migraine prevalence. A review of population-based studies. Neurology 44: S17–23. [PubMed] [Google Scholar]
- 13. Facchinetti F, Sgarbi L, Piccinini F (2000) Hypothalamic resetting at puberty and the sexual dimorphism of migraine. Funct Neurol 15 Suppl 3137–142. [PubMed] [Google Scholar]
- 14. Cochran SD, Mays VM (2007) Physical health complaints among lesbians, gay men, and bisexual and homosexually experienced heterosexual individuals: results from the California Quality of Life Survey. Am J Public Health 97: 2048–2055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Borsook D, Erpelding N, Lebel A, Linnman C, Veggeberg R, et al.. (2014) Sex and the Migraine Brain. Neurobiol Disease In Press. [DOI] [PMC free article] [PubMed]
- 16. Borsook D, Maleki N, Becerra L, McEwen B (2012) Understanding migraine through the lens of maladaptive stress responses: a model disease of allostatic load. Neuron 73: 219–234. [DOI] [PubMed] [Google Scholar]
- 17. Buchel C, Friston K (2000) Assessing interactions among neuronal systems using functional neuroimaging. Neural Netw 13: 871–882. [DOI] [PubMed] [Google Scholar]
- 18. Smith SM, Jenkinson M, Woolrich MW, Beckmann CF, Behrens TE, et al. (2004) Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 23 Suppl 1S208–219. [DOI] [PubMed] [Google Scholar]
- 19. Saleem SN, Said AH, Lee DH (2007) Lesions of the hypothalamus: MR imaging diagnostic features. Radiographics 27: 1087–1108. [DOI] [PubMed] [Google Scholar]
- 20. Woolrich MW, Ripley BD, Brady M, Smith SM (2001) Temporal autocorrelation in univariate linear modeling of FMRI data. Neuroimage 14: 1370–1386. [DOI] [PubMed] [Google Scholar]
- 21. Pendse G, Borsook D, Becerra L (2009) Enhanced false discovery rate using Gaussian mixture models for thresholding fMRI statistical maps. Neuroimage 47: 231–261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Moulton EA, Becerra L, Maleki N, Pendse G, Tully S, et al. (2011) Painful heat reveals hyperexcitability of the temporal pole in interictal and ictal migraine States. Cereb Cortex 21: 435–448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Maleki N, Becerra L, Brawn J, McEwen B, Burstein R, et al. (2013) Common hippocampal structural and functional changes in migraine. Brain Struct Funct 218: 903–912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Beissner F, Meissner K, Bar KJ, Napadow V (2013) The autonomic brain: an activation likelihood estimation meta-analysis for central processing of autonomic function. J Neurosci 33: 10503–10511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Samuels ER, Szabadi E (2008) Functional neuroanatomy of the noradrenergic locus coeruleus: its roles in the regulation of arousal and autonomic function part I: principles of functional organisation. Curr Neuropharmacol 6: 235–253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Samuels ER, Szabadi E (2008) Functional neuroanatomy of the noradrenergic locus coeruleus: its roles in the regulation of arousal and autonomic function part II: physiological and pharmacological manipulations and pathological alterations of locus coeruleus activity in humans. Curr Neuropharmacol 6: 254–285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Saunders RC, Aggleton JP (2007) Origin and topography of fibers contributing to the fornix in macaque monkeys. Hippocampus 17: 396–411. [DOI] [PubMed] [Google Scholar]
- 28. Haines DE, Dietrichs E (1984) An HRP study of hypothalamo-cerebellar and cerebello-hypothalamic connections in squirrel monkey (Saimiri sciureus). J Comp Neurol 229: 559–575. [DOI] [PubMed] [Google Scholar]
- 29. Jeffery KJ (2007) Self-localization and the entorhinal-hippocampal system. Curr Opin Neurobiol 17: 684–691. [DOI] [PubMed] [Google Scholar]
- 30. Ploghaus A, Narain C, Beckmann CF, Clare S, Bantick S, et al. (2001) Exacerbation of pain by anxiety is associated with activity in a hippocampal network. J Neurosci 21: 9896–9903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Moulton EA, Elman I, Pendse G, Schmahmann J, Becerra L, et al. (2011) Aversion-related circuitry in the cerebellum: responses to noxious heat and unpleasant images. J Neurosci 31: 3795–3804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Seifert F, Schuberth N, De Col R, Peltz E, Nickel FT, et al. (2013) Brain activity during sympathetic response in anticipation and experience of pain. Hum Brain Mapp 34: 1768–1782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Markowitsch HJ, Emmans D, Irle E, Streicher M, Preilowski B (1985) Cortical and subcortical afferent connections of the primate’s temporal pole: a study of rhesus monkeys, squirrel monkeys, and marmosets. J Comp Neurol 242: 425–458. [DOI] [PubMed] [Google Scholar]
- 34. Demarquay G, Royet JP, Giraud P, Chazot G, Valade D, et al. (2006) Rating of olfactory judgements in migraine patients. Cephalalgia 26: 1123–1130. [DOI] [PubMed] [Google Scholar]
- 35. Demarquay G, Royet JP, Mick G, Ryvlin P (2008) Olfactory hypersensitivity in migraineurs: a H(2)(15)O-PET study. Cephalalgia 28: 1069–1080. [DOI] [PubMed] [Google Scholar]
- 36. Stoodley CJ, Schmahmann JD (2009) Functional topography in the human cerebellum: a meta-analysis of neuroimaging studies. Neuroimage 44: 489–501. [DOI] [PubMed] [Google Scholar]
- 37. Nelson LE, Guo TZ, Lu J, Saper CB, Franks NP, et al. (2002) The sedative component of anesthesia is mediated by GABA(A) receptors in an endogenous sleep pathway. Nat Neurosci 5: 979–984. [DOI] [PubMed] [Google Scholar]
- 38. Stone EA, Quartermain D, Lin Y, Lehmann ML (2007) Central alpha1-adrenergic system in behavioral activity and depression. Biochem Pharmacol 73: 1063–1075. [DOI] [PubMed] [Google Scholar]
- 39. Aston-Jones G, Rajkowski J, Kubiak P, Valentino RJ, Shipley MT (1996) Role of the locus coeruleus in emotional activation. Prog Brain Res 107: 379–402. [DOI] [PubMed] [Google Scholar]
- 40. Jones SL (1991) Descending noradrenergic influences on pain. Prog Brain Res 88: 381–394. [DOI] [PubMed] [Google Scholar]
- 41. Condes-Lara M (1998) Different direct pathways of locus coeruleus to medial prefrontal cortex and centrolateral thalamic nucleus: electrical stimulation effects on the evoked responses to nociceptive peripheral stimulation. Eur J Pain 2: 15–23. [DOI] [PubMed] [Google Scholar]
- 42. Shammah-Lagnado SJ, Alheid GF, Heimer L (1996) Efferent connections of the caudal part of the globus pallidus in the rat. J Comp Neurol 376: 489–507. [DOI] [PubMed] [Google Scholar]
- 43.Stoffers D, Altena E, van der Werf YD, Sanz-Arigita EJ, Voorn TA, et al.. (2013) The caudate: a key node in the neuronal network imbalance of insomnia? Brain. [DOI] [PMC free article] [PubMed]
- 44. Borsook D, Upadhyay J, Chudler EH, Becerra L (2010) A key role of the basal ganglia in pain and analgesia–insights gained through human functional imaging. Mol Pain 6: 27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Grahn JA, Parkinson JA, Owen AM (2008) The cognitive functions of the caudate nucleus. Prog Neurobiol 86: 141–155. [DOI] [PubMed] [Google Scholar]
- 46. Kelley AE, Baldo BA, Pratt WE, Will MJ (2005) Corticostriatal-hypothalamic circuitry and food motivation: integration of energy, action and reward. Physiol Behav 86: 773–795. [DOI] [PubMed] [Google Scholar]
- 47. Kievit J, Kuypers HG (1975) Basal forebrain and hypothalamic connection to frontal and parietal cortex in the Rhesus monkey. Science 187: 660–662. [DOI] [PubMed] [Google Scholar]
- 48. Critchley HD, Mathias CJ, Josephs O, O’Doherty J, Zanini S, et al. (2003) Human cingulate cortex and autonomic control: converging neuroimaging and clinical evidence. Brain 126: 2139–2152. [DOI] [PubMed] [Google Scholar]
- 49. Critchley HD, Elliott R, Mathias CJ, Dolan RJ (2000) Neural activity relating to generation and representation of galvanic skin conductance responses: a functional magnetic resonance imaging study. J Neurosci 20: 3033–3040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Bashir A, Lipton RB, Ashina S, Ashina M (2013) Migraine and structural changes in the brain: a systematic review and meta-analysis. Neurology 81: 1260–1268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Mosek A, Novak V, Opfer-Gehrking TL, Swanson JW, Low PA (1999) Autonomic dysfunction in migraineurs. Headache 39: 108–117. [DOI] [PubMed] [Google Scholar]
- 52. Vollono C, Gnoni V, Testani E, Dittoni S, Losurdo A, et al. (2013) Heart rate variability in sleep-related migraine without aura. J Clin Sleep Med 9: 707–714. [DOI] [PMC free article] [PubMed] [Google Scholar]