

Abstract
Local steroid injections are widely used for diagnostic and therapeutic purposes in the management of carpal tunnel syndrome. The median nerve injury is the most serious complication in association with carpal tunnel injections although the incidence is low. A median nerve injury will be presented with shooting pain at the injection time along with other sensory distortion, motor weakness and muscle atrophy. The management includes a conservative treatment and a surgical exploration. Carpal tunnel injections should be used at a minimum only. If such steroid injection is required, an appropriate needle positioning is vital for the nerve injury prevention. The patient should not be heavily sedated and should be encouraged to inform experiences of numbness/paresthesia during the procedure immediately.
Keywords: carpal tunnel syndrome, median nerve, steroid
INTRODUCTION
Local steroid injections are widely used in the management of carpal tunnel syndrome (CTS) [1,2,3,4,5,6,7,8]. The management of CTS with steroid injections was first reported by Kopell [9] in 1958. Since then numerous cases have been reported. Steroid injections can provide a symptoms relief and a diagnosis aid for CTS. Such injections can also act as a prognostic factor. For example, a good response to a steroid injection will result in a favorable surgical outcome; however, the opposite may not be true [3].
Despite this, steroid injections can cause complications such as ischemia, skin depigmentation and atrophy. The median nerve injury (MNI) is the most serious complication associated with a local steroid injection for CTS among them [10,11,12,13].
The incidence of MNI during carpal tunnel injections is unclear. Also the incidence seems not common although the MNI are underreported probably. Bland [14] reviewed the published studies of steroid injection and documented a pool of combined series with over 3,000 injections without any instance of median nerve injury which means the risk may be less than 0.1% in competent hands.
METHODS
For this study a PubMed database search was performed from 1950 to 2012 using the search terms median nerve, median nerve injury, injection injury, steroid injections, management of carpal tunnel syndrome, and different structures relevant to this review including palmaris longus tendon, flexor carpi radialis tendon and flexor digitorum superficialis.
MECHANISMS OF INJURY
Median nerve injuries result from direct needle injuries [1,11,12], breakdown of the blood-nerve barrier [15], neurotoxicity of the injected steroids [16], and pressure effect of the steroid [17]. A median nerve injury may lead to a formation of a granuloma. Both, myelinated and unmyelinated nerve fibers, are affected. There is also a direct neurotoxic effect on the axon and the Schwann cells [15].
Typically, the median nerve is just dorsal and radial to the palmaris longus tendon at the carpal tunnel level. If the needle inserted radial to the palmaris longus tendon, the nerve can be injured. However, the patients with CTS are more vulnerable to needle injury than healthy subjects even if the needle is inserted at correct position, because the median nerve is swollen and/or flatten around the wrist crease. Anatomic variation such as a median nerve in an abnormal location, a bifid median nerve and anomalous muscle also may affect the procedure [18,19,20,21].
Several agents were reported as potential causes for median nerve injuries, including local analgesics and preservatives [11], celestone [17] and methylprednisolone in polyethylene glycol mixed with bupivacaine hydrochloride containing methylparaben preservative [11]. Other members of the polyethylene glycol family and buffers and other compounds which were found in some steroids are neurotoxic [22,23]. Also an injection of bupivacaine administered in the intrafascicular plane has been reported as a cause of axons degeneration [24]. Owen [25] postulated the preservatives used in local anesthetics may in combination cause a flocculation of steroid preparations.
Mackinnon et al. [16] experimented with different steroids in an animal study and reported as followed:
- Hydrocortisone and triamcinolone caused widespread axonal and myelin degeneration.
- Methylprednisolone was moderately toxic.
- Dexamethasone was the least neurotoxic agent.
- All steroids are neurotoxic when injected in the intrafascicular plane. Injecting in the extrafascicular plane has no effect on the nerve.
- No association between the degree of nerve damage and the hydrophilicity of the agent was found.
The degree of nerve damage depends on the agent which was used and the site in which the agent was injected [16,26,27]. Gentili et al. [26] performed experimental studies on Wistar rats and found that the site of injection was the most important factor for the degree prediction of nerve damage. For injections in the intrafascicular plane, the degree varied depending on the agents which were used. In some instances pathological changes could be seen in less than 30 minutes after injection [15].
PRESENTATION AND INVESTIGATIONS
Shooting pain at the time of the injection along with numbness, paresthesia and other sensory deficits and distortions in the median nerve supply area will be presented in a patient with MNI. Other reported symptoms include motor weakness, thenar atrophy, allodynia, hyperesthesia and hypoalgesia. The patient may also show positive Phalen's and Tinel's signs [1,11,13,15,17]. A transient exacerbation of CTS symptoms following the steroid injection is present in many patients. A median nerve damage should be considered if the symptoms persist for more than 48 hours [1,2,8].
B-mode ultrasonography helps in lesion localization. An usual finding for a postiatrogenic nerve injury is an enlarged hypoechoic nerve. A sonoelastography can evaluate the tissue stiffness and the elasticity of the peripheral nerve. A with sonoelastography observed change from stiff to soft tissue correlates with the peripheral nerve recovery over the time. Nerve stimulation studies are also important for an evaluation of the regenerative capacity and the state of the nerve [13,28]. Park et al. [13] reported serial changes of ultrasonography, sonoelastographic and electrodiagnostic studies to evaluate a median sensory neuropathy after a carpal tunnel steroid injection. A swelling of the median nerve and a focal heterogenous hyperechoic area lateral to the median nerve were observed in the proximal carpal tunnel 3 days after injection. The appearance of the hyperechoic area was red under sonoelastographic imaging, which indicated hard tissue. A conservative treatment was initiated. On day 14 after injection, a prolonged onset latency of compound muscle action potential of median nerve was revealed. Six months after injection, symptoms such as pain or paresthesia were cured. The hyperechoic area was no longer visible and the cross-sectional area of the median nerve had decreased. Under sonoelastography, the area appeared yellow-green, which indicated an intermediate tissue hardness. Also a shorter onset latency of compound muscle action potential was revealed.
MANAGEMENT
Some physicians suggest an immediate surgical intervention of carpal tunnel release if symptoms of acute median nerve compression were present after steroid injection. Other physicians believe conservative management alone should be appropriate for an incomplete nerve injury [1,11].
The management recommended in general is in continuity similar to that of other nerve lesions. A nonsurgical management consists of activity modification, splinting physiotherapy, medication and local steroid injections [13,14]. If no spontaneous resolution or no sign of recovery can be observed for over 3 months, then a surgery may be considered. Other indications for a surgery include a severe neuromotor functional loss, a severe debilitating pain or if the injected agent is known to be extremely neurotoxic [11,15,26,29,30].
A surgical intervention such as neurolysis, resection or graft repair is recommended for complete lesions. Also a gentle debridement of the crystal from the nerve may be performed [12]. An appropriate graft availability, difficulties in obtaining the autologous grafts, unsatisfactory cable grafts and rejection of homografts can be issues which are associated with the resection. Therefore, a resection is recommended only for cases in which the nerve function is lost completely and a self-recovery cannot be expected, when a neuroma has replaced the nerve or when the nerve action potential is through the neuroma negative or with the possibility to obtain a good length of the dissected nerve for an opposing of the resected ends. Intraoperative electrophysiological techniques may improve the quality of the nerve repair [31]. With a regenerative capacity, the surgeon should thus consider that the recovery occurring after surgery might be due to the natural course of nerve regeneration [29].
PREVENTION
Carpal tunnel injections should be used at a minimum. However, the optimal management of CTS is still controversy. Phalen [2] reported a thickened flexor synovium in most of CTS cases and prescribed steroids to reduce the inflammation of flexor tenosynovitis. He suggested up to 3 steroid injections should be attempted in patients with CTS before a surgery should be considered. Marshall et al. [32] reported 2 steroid injections compared with 1 injection did not provide further clinical improvement. They concluded also local steroid injections did not improve the clinical outcome significantly when compared to either anti-inflammatory drugs and splinting after 8 weeks or helium-neon laser treatment after 6 months. Other investigators suggest steroid injections for the CTS management should be used in cases in which temporary relief is required, such as pregnancy, change in occupation or myxedema [1,10,17]. Some surgeons believe steroid injections provide only symptomatic relief and the medial nerve degeneration continues until the surgery becomes inevitable [14]. Ly-Pen et al. [33,34] evaluated the effect of steroid injections and surgery in patients with CTS over a 2 years period. At the 1-year follow-up, little differences in the symptomatic relief was seen between the two treatment options. However, the surgery had an additional long-term benefit at the 2-year follow-up. In another recent study, the authors found that while both local steroid injection and decompressive surgery were clinically effective in reducing symptoms of CTS, the neurologic parameters of the nerve conduction study were improved only in patients with surgery at 12-months follow-up [35].
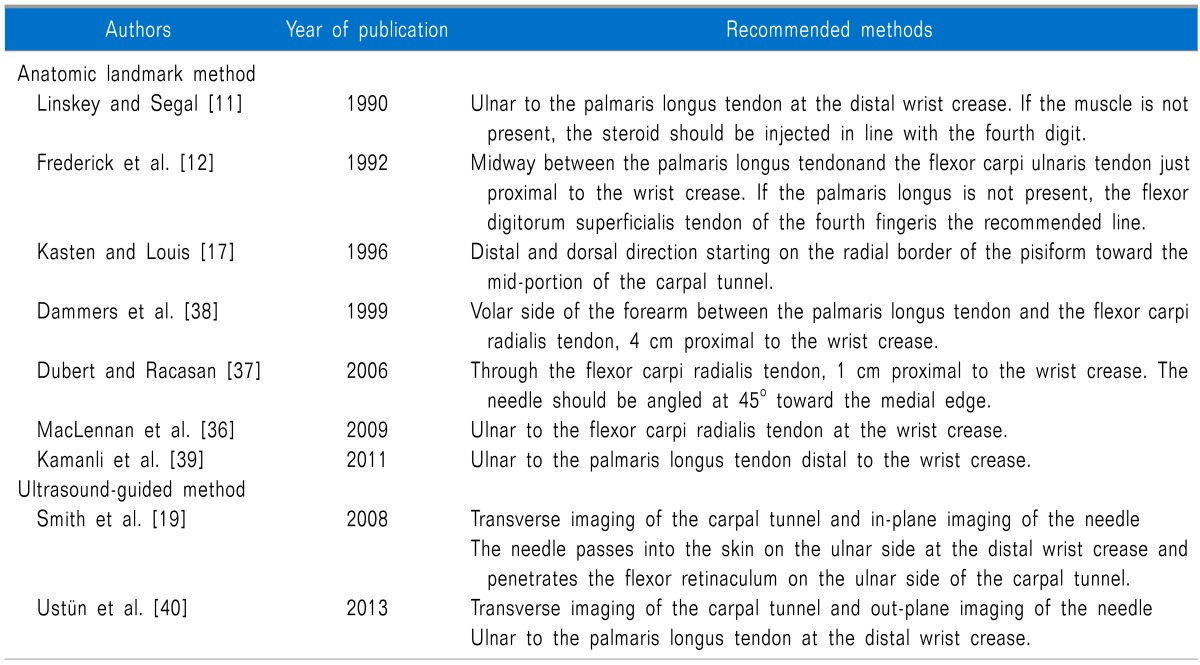
If the steroid injection is required, careful attention to anatomic landmarks and an appropriate needle positioning is vital for nerve injury prevention. Most widely accepted approach is in which the needle is inserted just ulnar to the palmaris longus tendon at the wrist crease [3,11,36]. Other routes of injections based on anatomic landmarks have been described [11,12,17,36,37,38,39]. Recently, ultrasound-guided carpal tunnel injections have been raised in several studies [18,19,40]. Ultrasound provides real-time anatomic image, therefore it could improve the accuracy of the intervention (Fig. 1). A randomized prospective study compared the efficacy of ultrasound-guided and blind steroid injection in patients with CTS. Although both methods were effective in reducing the symptoms of CTS, earlier onset and better improvement of symptom relief were detected in the ultrasound-guided group [40]. However, more studies are needed to clarify the safety issue that image-guided injection could significantly reduce the incidence of MNI in patients with CTS. Several recommended methods for preventing MNI are summarized in Table 1.
Fig. 1.

(A) Ultrasound-guided carpal tunnel injection. It shows transducer position for transverse imaging of the carpal tunnel and in-plane needle approach. (B) Transverse sonogram of the left carpal tunnel in a patient with carpal tunnel syndrome. Arrows indicate flexor retinaculum, Asterisk: anechoic injectate, N: needle, MN: median nerve, T: flexor tendons (These figures are quoted from the paper of Smith et al. [19] after permission.).
Table 1.
Recommended Methods for Prevention of Median Nerve Injuries Caused by Carpal Tunnel Injections
To choice a least neurotoxic agent is also an important factor. Frederick et al. [12] used betamethasone, although McConnell and Bush [1] recommend the use of a soluble dexamethasone preparation. Also the use of a blunt beveled 22-gauge needle may diminish the risk of nerve penetration and compromise [41]. An injection administered into the skin can cause pigment changes and fat atrophy in the subcutaneous layer. Hence, the steroid should be injected only into the carpal tunnel.
During the CTS management, the patient should not be heavily sedated and should be encouraged to inform the interventionist if he/she experiences numbness/paresthesia during the procedure immediately. In this case the needle should be repositioned.
When a steroid injection is given for CTS treatment, pain may be caused due to transient inflammatory changes. Such changes may be confused with a median nerve injury. Therefore the follow-up with the patient is important. If the pain symptom continues 48 hours post injection, a median nerve injury should be suspected [1,11,13,17].
CONCLUSIONS
A MNI due to a carpal tunnel injection is a preventable complication. Injections should be used at a minimum. If an injection is needed, the appropriate needle positioning is vital to prevent a nerve injury. If a nerve injury is suspected, an immediate and optimal management can reduce the neurological sequels and maximize the recovery.
ACKNOWLEDGEMENTS
This research was supported by the 2014 specific promotion program funded by Jeju National University.
References
- 1.McConnell JR, Bush DC. Intraneural steroid injection as a complication in the management of carpal tunnel syndrome. A report of three cases. Clin Orthop Relat Res. 1990;(250):181–184. [PubMed] [Google Scholar]
- 2.Phalen GS. The carpal-tunnel syndrome. Seventeen years' experience in diagnosis and treatment of six hundred fifty-four hands. J Bone Joint Surg Am. 1966;48:211–228. [PubMed] [Google Scholar]
- 3.Green DP. Diagnostic and therapeutic value of carpal tunnel injection. J Hand Surg Am. 1984;9:850–854. doi: 10.1016/s0363-5023(84)80065-9. [DOI] [PubMed] [Google Scholar]
- 4.Gelberman RH, Aronson D, Weisman MH. Carpal-tunnel syndrome. Results of a prospective trial of steroid injection and splinting. J Bone Joint Surg Am. 1980;62:1181–1184. [PubMed] [Google Scholar]
- 5.Goodman HV, Foster JB. Effect of local corticosteroid injection on median nerve conduction in carpal tunnel syndrome. Ann Phys Med. 1962;6:287–294. doi: 10.1093/rheumatology/6.7.287. [DOI] [PubMed] [Google Scholar]
- 6.Ozdoğan H, Yazici H. The efficacy of local steroid injections in idiopathic carpal tunnel syndrome: a double-blind study. Br J Rheumatol. 1984;23:272–275. doi: 10.1093/rheumatology/23.4.272. [DOI] [PubMed] [Google Scholar]
- 7.Schuchmann JA, Melvin JL, Duran RJ, Coleman CR. Evaluation of local steroid injection for carpal tunnel syndrome. Arch Phys Med Rehabil. 1971;52:253–255. [PubMed] [Google Scholar]
- 8.Wood MR. Hydrocortisone injections for carpal tunnel syndrome. Hand. 1980;12:62–64. doi: 10.1016/s0072-968x(80)80031-3. [DOI] [PubMed] [Google Scholar]
- 9.Kopell HP. Carpal tunnel compression median neuropathy treated nonsurgically. N Y State J Med. 1958;58:744–745. [PubMed] [Google Scholar]
- 10.Tavares SP, Giddins GE. Nerve injury following steroid injection for carpal tunnel syndrome. A report of two cases. J Hand Surg Br. 1996;21:208–209. doi: 10.1016/s0266-7681(96)80099-4. [DOI] [PubMed] [Google Scholar]
- 11.Linskey ME, Segal R. Median nerve injury from local steroid injection in carpal tunnel syndrome. Neurosurgery. 1990;26:512–515. doi: 10.1097/00006123-199003000-00021. [DOI] [PubMed] [Google Scholar]
- 12.Frederick HA, Carter PR, Littler JW. Injection injuries to the median and ulnar nerves at the wrist. J Hand Surg Am. 1992;17:645–647. doi: 10.1016/0363-5023(92)90309-d. [DOI] [PubMed] [Google Scholar]
- 13.Park GY, Kim SK, Park JH. Median nerve injury after carpal tunnel injection serially followed by ultrasonographic, sonoelastographic, and electrodiagnostic studies. Am J Phys Med Rehabil. 2011;90:336–341. doi: 10.1097/PHM.0b013e31820ff67a. [DOI] [PubMed] [Google Scholar]
- 14.Bland JD. Treatment of carpal tunnel syndrome. Muscle Nerve. 2007;36:167–171. doi: 10.1002/mus.20802. [DOI] [PubMed] [Google Scholar]
- 15.Hudson AR. Nerve injection injuries. Clin Plast Surg. 1984;11:27–30. [PubMed] [Google Scholar]
- 16.Mackinnon SE, Hudson AR, Gentili F, Kline DG, Hunter D. Peripheral nerve injection injury with steroid agents. Plast Reconstr Surg. 1982;69:482–490. doi: 10.1097/00006534-198203000-00014. [DOI] [PubMed] [Google Scholar]
- 17.Kasten SJ, Louis DS. Carpal tunnel syndrome: a case of median nerve injection injury and a safe and effective method for injecting the carpal tunnel. J Fam Pract. 1996;43:79–82. [PubMed] [Google Scholar]
- 18.Kim DH, Jang JE, Park BK. Anatomical basis of ulnar approach in carpal tunnel injection. Pain Physician. 2013;16:E191–E198. [PubMed] [Google Scholar]
- 19.Smith J, Wisniewski SJ, Finnoff JT, Payne JM. Sonographically guided carpal tunnel injections: the ulnar approach. J Ultrasound Med. 2008;27:1485–1490. doi: 10.7863/jum.2008.27.10.1485. [DOI] [PubMed] [Google Scholar]
- 20.Lindley SG, Kleinert JM. Prevalence of anatomic variations encountered in elective carpal tunnel release. J Hand Surg Am. 2003;28:849–855. doi: 10.1016/s0363-5023(03)00365-4. [DOI] [PubMed] [Google Scholar]
- 21.Propeck T, Quinn TJ, Jacobson JA, Paulino AF, Habra G, Darian VB. Sonography and MR imaging of bifid median nerve with anatomic and histologic correlation. AJR Am J Roentgenol. 2000;175:1721–1725. doi: 10.2214/ajr.175.6.1751721. [DOI] [PubMed] [Google Scholar]
- 22.Chino N, Awad EA, Kottke FJ. Pathology of propylene glycol administered by perineural and intramuscular injection in rats. Arch Phys Med Rehabil. 1974;55:33–38. [PubMed] [Google Scholar]
- 23.Sun CN, White HJ. Destruction and remyelinization of peripheral nerve after alcohol injury. Exp Pathol (Jena) 1974;9:169–174. [PubMed] [Google Scholar]
- 24.Gentili F, Hudson AR, Hunter D, Kline DG. Nerve injection injury with local anesthetic agents: a light and electron microscopic, fluorescent microscopic, and horseradish peroxidase study. Neurosurgery. 1980;6:263–272. [PubMed] [Google Scholar]
- 25.Owen DS. Aspiration and injection of joints and soft tissues. In: Kelly WN, Harris ED Jr, Ruddy S, Sledge CB, editors. Kelley's textbook of rheumatology. 2nd ed. Philadelphia (PA): WB Saunders; 1985. pp. 546–560. [Google Scholar]
- 26.Gentili F, Hudson AR, Hunter D. Clinical and experimental aspects of injection injuries of peripheral nerves. Can J Neurol Sci. 1980;7:143–151. doi: 10.1017/s0317167100023520. [DOI] [PubMed] [Google Scholar]
- 27.Gentili F, Hudson AR, Kline D, Hunter D. Early changes following injection injury of peripheral nerves. Can J Surg. 1980;23:177–182. [PubMed] [Google Scholar]
- 28.Duncan I, Sullivan P, Lomas F. Sonography in the diagnosis of carpal tunnel syndrome. AJR Am J Roentgenol. 1999;173:681–684. doi: 10.2214/ajr.173.3.10470903. [DOI] [PubMed] [Google Scholar]
- 29.Clark WK. Surgery for injection injuries of peripheral nerves. Surg Clin North Am. 1972;52:1325–1328. doi: 10.1016/s0039-6109(16)39844-9. [DOI] [PubMed] [Google Scholar]
- 30.Clark K, Williams PE, Jr, Willis W, McGavran WL., 3rd Injection injury of the sciatic nerve. Clin Neurosurg. 1970;17:111–125. doi: 10.1093/neurosurgery/17.cn_suppl_1.111. [DOI] [PubMed] [Google Scholar]
- 31.Terzis JK, Dykes RW, Hakstian RW. Electrophysiological recordings in peripheral nerve surgery: a review. J Hand Surg Am. 1976;1:52–66. doi: 10.1016/s0363-5023(76)80025-1. [DOI] [PubMed] [Google Scholar]
- 32.Marshall S, Tardif G, Ashworth N. Local corticosteroid injection for carpal tunnel syndrome. Cochrane Database Syst Rev. 2007;(2):CD001554. doi: 10.1002/14651858.CD001554.pub2. [DOI] [PubMed] [Google Scholar]
- 33.Ly-Pen D, Andréu JL, de Blas G, Sánchez-Olaso A, Millán I. Surgical decompression versus local steroid injection in carpal tunnel syndrome: a one-year, prospective, randomized, open, controlled clinical trial. Arthritis Rheum. 2005;52:612–619. doi: 10.1002/art.20767. [DOI] [PubMed] [Google Scholar]
- 34.Ly-Pen D, Andréu JL, Millán I, de Blas G, Sánchez-Olaso A. Comparison of surgical decompression and local steroid injection in the treatment of carpal tunnel syndrome: 2-year clinical results from a randomized trial. Rheumatology (Oxford) 2012;51:1447–1454. doi: 10.1093/rheumatology/kes053. [DOI] [PubMed] [Google Scholar]
- 35.Andreu JL, Ly-Pen D, Millán I, de Blas G, Sánchez-Olaso A. Local injection versus surgery in carpal tunnel syndrome: Neurophysiologic outcomes of a randomized clinical trial. Clin Neurophysiol. 2013 doi: 10.1016/j.clinph.2013.11.010. [in press] [DOI] [PubMed] [Google Scholar]
- 36.MacLennan A, Schimizzi A, Meier KM, Barron OA, Catalano L, Glickel S. Comparison of needle position proximity to the median nerve in 2 carpal tunnel injection methods: a cadaveric study. J Hand Surg Am. 2009;34:875–879. doi: 10.1016/j.jhsa.2009.01.028. [DOI] [PubMed] [Google Scholar]
- 37.Dubert T, Racasan O. A reliable technique for avoiding the median nerve during carpal tunnel injections. Joint Bone Spine. 2006;73:77–79. doi: 10.1016/j.jbspin.2005.02.006. [DOI] [PubMed] [Google Scholar]
- 38.Dammers JW, Veering MM, Vermeulen M. Injection with methylprednisolone proximal to the carpal tunnel: randomised double blind trial. BMJ. 1999;319:884–886. doi: 10.1136/bmj.319.7214.884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kamanli A, Bezgincan M, Kaya A. Comparison of local steroid injection into carpal tunnel via proximal and distal approach in patients with carpal tunnel syndrome. Bratisl Lek Listy. 2011;112:337–341. [PubMed] [Google Scholar]
- 40.Ustün N, Tok F, Yagz AE, Kizil N, Korkmaz I, Karazincir S, et al. Ultrasound-guided vs. blind steroid injections in carpal tunnel syndrome: a single-blind randomized prospective study. Am J Phys Med Rehabil. 2013;92:999–1004. doi: 10.1097/PHM.0b013e31829b4d72. [DOI] [PubMed] [Google Scholar]
- 41.Wolf AW. Injection injuries to the median and ulnar nerves of the wrist. J Hand Surg Am. 1993;18:546–547. doi: 10.1016/0363-5023(93)90114-I. [DOI] [PubMed] [Google Scholar]