

Abstract
In an initial study it was shown that (without hormonal influences) middle-aged (premenopausal) women show a smaller frequency and intensity range and a lower fundamental frequency of the voice compared to young women. To investigate the impact of menopause on voice and nasal resonance a cross-sectional non-randomized study design was used. Vocal characteristics and nasal resonance in premenopausal and postmenopausal women without hormone therapy (HT) were compared. Postmenopausal women without HT showed a significantly lower speaking fundamental frequency (SFF) and were able to phonate lower compared to postmenopausal women with HT. The mean difference in SFF was 14 Hz. HT can also counteract the menopausal changes in SFF. The lower SFF did not result in vocal complaints. Further research about the impact of menopause and HT on voice should concentrate on elite professional voice users.
Keywords: BMI, hormone therapy, nasal resonance, premenopausal, postmenopausal, voice
One of the major difficulties in this research field, is the distinction between effects of the aging process and those of the menopause. To investigate menopausal symptoms and distinguish between the effects of aging and those of menopause, the World Health Organization (1996) recommends two research methods. The first possible method (McKinlay, 1994) is a model requiring prospective observations on a large number of subjects followed during the pre-, peri- and postmenopausal periods to estimate the shape of the curve of data points on the variable of interest in order to distinguish better between the effects of aging and those of menopause. Another possibility is a cross-sectional approach including large numbers of middle-aged women within a restricted age range in order to distinguish the differences in symptom frequency by menopausal status, while controlling for age (WHO, 1996). The first option implies a longitudinal study over 10 years. In our study, the second option was preferred.
In an initial study (D’haeseleer et al., 2011a) the impact of aging on the voice was measured by comparing vocal characteristics of reproductive young (n = 22) and middle-aged (n = 22) women. In many studies about vocal aging the menopausal transition is not taken into account. To exclude sex hormonal influences caused by menopause, menopausal women were excluded from the study group. The results of the study revealed that (without hormonal influences) middle-aged (premenopausal) women show a smaller frequency and intensity range and a lower fundamental frequency of the voice compared to young women. These results are important for de differential diagnosis between vocal changes caused by aging and vocal changes caused by menopause. The same study design was used to investigate the impact of aging on nasal resonance of women (D’haeseleer et al., 2011b). The middle-aged (premenopausal) women (n = 31) showed a higher amount of nasal resonance by means of a higher Nasality Severity Index compared to younger women (n = 22). Caution is needed with the interpretation of the results. The differences in NSI were so small that clinical relevance was questioned. Nevertheless, age should be included as an influencing factor when studying nasal resonance in middle-aged women.
To investigate the impact of menopause on voice and nasal resonance a cross-sectional non-randomized study design was used (D’haeseleer et al., 2011c, D’haeseleer et al., 2011d). Vocal characteristics and nasal resonance in premenopausal and postmenopausal women (without HT) were compared. In contrast to other studies (Meurer et al., 2004a; Meurer et al., 2004b; Raj et al., 2010) the results were analyzed controlling for age to exclude the impact of aging. No differences in nasal resonance scores were found between premenopausal and postmenopausal women. Hormonal changes during menopause do not have an impact on nasal resonance of middle-aged women. The study about the impact of menopause on voice revealed that postmenopausal women (without HT) showed an overall good vocal quality (Dysphonia Severity Index % of 83%). However compared to premenopausal women they showed a decreased speaking fundamental frequency (SFF). The mean difference in SFF between pre- and postmenopausal women (without HT) was 13 Hz. In the literature Abitbol (Abitbol and Abitbol 1999; Caruso et al., 2000) reported organic changes in the vocal folds like dystrophy and atrophy of the vocal fold epithelium and edema of the vocal folds in postmenopausal women. In our study no differences were observed between pre- and postmenopausal women in aspect or function of the vocal folds using videostroboscopy. However, observation through laryngoscopy remains a subjective assessment technique that is not sensitive enough to evaluate small changes in mucosa. Moreover, there was a large drop-out for the stroboscopy mainly caused by the presence of pharyngeal reflex of the subjects or a decreased quality of the stroboscopic images. Future research should focus on laryngeal cytological aspects in postmenopausal women using vocal epithelium smears and the presence of sex hormone receptors in the female larynx.
HT is a frequently used therapy for menopausal complaints. However, it was not yet clear whether HT could also counteract the menopausal voice changes. The main purpose of the next study (D’haeseleer et al., 2011e) was to investigate the impact of HT on vocal characteristics in postmenopausal women by comparing postmenopausal women with HT and postmenopausal women without HT. Postmenopausal women without HT showed a significantly lower SFF and were able to phonate lower compared to postmenopausal women with HT. The mean difference in SFF was 14 Hz. HT can also counteract the menopausal changes in SFF. Lindholm (Lindholm et al., 1997) suggested that the type of HT may be an important factor when studying the impact of HT on vocal characteristics. In our study no differences in objective and subjective vocal characteristics were found between estrogen therapy (ET) and estrogen and progestogen therapy (E-PT). However, one should notice that the number of subjects in the ET group (n = 16) was rather small compared to the E-PT group (n = 43). Possible differences in vocal characteristics between different types of HT, different concentrations of HT and different ways of administration of HT should be further investigated in future research.
In postmenopausal women adipose tissue becomes the main source of estrogen production. As the fat cell mass increases, the level of endogenous estrogens also increases. Women with a higher body mass index (BMI) have a higher production of estrone and higher estrone levels than normal-weight women (Freeman et al., 2010; Randolph et al., 2004). Different estrogen levels (during menopause or by taking HT) are associated with SFF differences. The purpose of the last study was to investigate the association between BMI and SFF in premenopausal women and postmenopausal women with and without HT. Only in the group of postmenopausal women without HT a positive correlation was found between BMI and SFF. This means that the postmenopausal women (without HT) with a higher BMI tend to have a higher SFF. Thus, BMI is an important influencing variable that must be taken into account when studying voice in postmenopausal women.
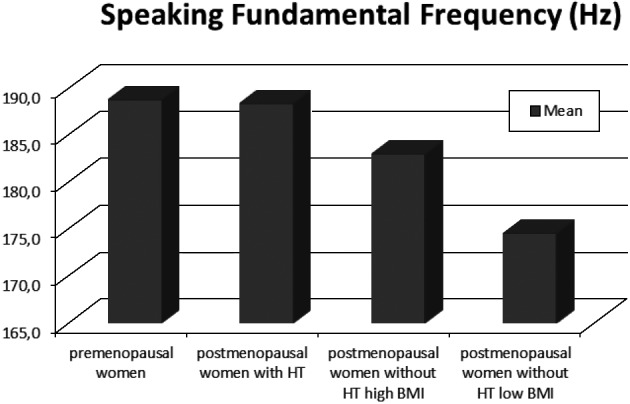
Regarding the impact of menopause and HT on voice we can distinguish four different groups of middle-aged women: premenopausal women, postmenopausal women with HT, postmenopausal women without HT and high BMI and postmenopausal women without HT and low BMI. Figure 1 shows the mean SFF during reading in these four groups of middle-aged women. Based on the results of the different studies we can conclude that menopause lowers the female voice and that HT counteracts this decrease in SFF. The mean SFF in postmenopausal women with and without HT was respectively 190Hz (SD: 21) and 176Hz (SD: 19). Both mean SFF’s are still located within the normative fundamental frequency range for a female voice of the Belgian Study Group on Voice Disorders (Van de Heyning et al., 1996) ranging from 167 Hz to 258Hz. A fundamental frequency of 165 Hz is the cutting point between the normal female fundamental frequency range and the ambiguous pitch range. The ambiguous pitch range (Oates and Dacakis, 1983) represents the pitch level at which speakers could not be confidently identified as either male or female and is based on the overlap between the male and female pitch range. The SFF of respectively 13.9% (n = 5/36) and 41.3% (n = 12/29) of the postmenopausal women with and without HT lies within the ambiguous pitch range.
Fig. 1. >Mean SFF in premenopausal women, postmenopausal women with HT, postmenopausal women without HT high BMI and postmenopausal women without HT low BMI.
The mean difference in SFF between postmenopausal women without HT and respectively postmenopausal women with HT and premenopausal women was 14 Hz and 13 Hz. These differences of 14 and 13 Hz correspond respectively with 1.32 and 1.23 semitones. An interesting question is whether these rather small differences are perceptually relevant or detectable for listeners? For pure tones between 100 and 2000 Hz the just noticeable difference (JND) also known as frequency difference limen (DLF) is 3 Hz (Shower and Biddulph, 1931; Wever and Wedell, 1941). However, voice is a complex acoustic signal. Moore and Moore (2003) investigated discrimination in F0 of complex tones and found that F0 differences of more than 1% are detectable for listeners. The difference in F0 between postmenopausal women without HT and premenopausal women or postmenopausal women with HT is respectively 6.9% [(189 Hz-176 Hz)/189 Hz] and 7.4% [(190 Hz-176 Hz)/190 Hz]. Thus, we can conclude that in general the menopausal changes in F0 must be detectable for listeners. However, listeners differ in their ability to detect F0 changes (Moore et al., 2008). Moreover, F0 differences of the own voice are easier to detect compared to F0 differences of another voice (Moore et al., 2008). Therefore, it is possible that not all postmenopausal women will detect the changes in the SFF of their voice.
The impact of vocal changes on the psychosocial functioning of these women was in this thesis measured by means of a self-evaluating questionnaire (VHI). Low scores in all groups of middle-aged women indicated an absence of a handicapping effect of vocal problems. The menopausal decrease in SFF does not necessarily result in an increase of vocal complaints. As this is a gradual process within the general aging process it is possible that the menopausal decrease in SFF is not noticed by many middle-aged women. Finally, like other menopausal complaints the severity of (vocal) symptoms can vary in each individual woman. Voice problems in each middle-aged woman should be investigated with knowledge about the impact of vocal aging, menopause and HT on voice.
Several limitations in our comprehensive studies need to be considered. The cross-sectional study design to investigate the impact of menopause and HT on voice and nasal resonance has its limitations. Middle-aged women are a very heterogeneous group with a lot of variables influencing the vocal characteristics like age, BMI, smoking habits, etc. Most of the influencing variables are controlled however some variables (like life habits, vocal habits, vocal load vocal hygiene during lifetime, etc.) are difficult to control. A longitudinal study of the voice and nasal resonance on the one hand during pre-, peri- and postmenopausal stages and on the other hand pre and post HT would exclude more variables. Another shortcoming of our studies is the absence of serum levels of the different sex hormones. Menopause is a clinical diagnosis. However, in future studies serum levels of sex hormones would provide additional information and could be used in a correlation between the levels of sex hormones and vocal characteristics.
Based on the results of our study we can conclude that postmenopausal women with and without HT show an overall good vocal quality. However, menopause lowers the voice with approximately 14Hz and HT counteracts this decrease in SFF. In postmenopausal women without HT the BMI should be taken into account since BMI is positively correlated to the SFF in this group. In the general population of postmenopausal women we do not recommend voice therapy or prevention campaigns since the majority of these women have an overall good vocal quality and the impact of the postmenopausal vocal changes on the psychosocial functioning is low. However, vocal complaints in individual women caused by hormonal fluctuations should be recognized by voice therapists, otorhinolaryngologists, gynecologists and general practitioners when working with middle-aged women. With an accurate diagnosis voice therapy whether or not in combination with HT (according to the medical advice) can be considered in these women.
Further research about the impact of menopause and HT on voice should concentrate on elite professional voice users. In this group even small vocal changes can have occupational consequences. In the future, research about the presence of hormone receptors in the larynx and the postmenopausal morphological (cytological aspects) changes in the larynx can lead to a better understanding of the mechanisms of postmenopausal voice changes. Regarding the impact of HT on the voice comparisons between the different types of HT and the different ways of administration would be useful for the clinicians prescribing the HT.
References
- Abitbol J, Abitbol P, Abitbol B. Sex hormones and the female voice. J Voice. 1999;13:424–446. doi: 10.1016/s0892-1997(99)80048-4. [DOI] [PubMed] [Google Scholar]
- Caruso S, Roccasalva L, Sapienza G. Laryngeal cytological aspects in women with surgically induced menopause who were treated with transdermal estrogen replacement therapy. Fertil Steril. 2000;74:1073–1079. doi: 10.1016/s0015-0282(00)01582-x. [DOI] [PubMed] [Google Scholar]
- haeseleer E, Depypere H, Claeys S. Vocal characteristics of middle-aged premenopausal women. J Voice. 2011;25:360–366. doi: 10.1016/j.jvoice.2009.10.016. [DOI] [PubMed] [Google Scholar]
- haeseleer E, Depypere H, Claeys S. Nasal resonance in middle aged women: a multiparameter approach. Ann Otol Rhinol Laryngol. 2011 doi: 10.1177/000348941112000904. [DOI] [PubMed] [Google Scholar]
- haeseleer E, Depypere H, Claeys S. The impact of the menopause on vocal quality. Menopause. 2011;18:267–272. doi: 10.1097/gme.0b013e3181f3ee36. [DOI] [PubMed] [Google Scholar]
- Freeman E, Sammel MD, Lin H. Obesity and reproductive hormone levels in the transition to menopause. Menopause. 2010;17:718–726. doi: 10.1097/gme.0b013e3181cec85d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindholm P, Vilkman E, Raudaskoski T. The effect of postmenopause and postmenopausal HRT on measured voice values and vocal symptoms. Maturitas. 1997;28:47–53. doi: 10.1016/s0378-5122(97)00062-5. [DOI] [PubMed] [Google Scholar]
- McKinlay S. Issues in design, measurement, and analysis for menopause research. Exp Gerontol. 1994;29:479–493. doi: 10.1016/0531-5565(94)90029-9. [DOI] [PubMed] [Google Scholar]
- Meurer E, Celeste M, Wender O. Phono-articulatory variations of woman in reproductive age and postmenopausal. J Voice. 2004;18:369–374. doi: 10.1016/j.jvoice.2003.02.001. [DOI] [PubMed] [Google Scholar]
- Meurer E, Wender M, Corleta H. Female suprasegmental speech parameters in reproductive age and postmenopause. Maturitas. 2004;48:71–77. doi: 10.1016/j.maturitas.2003.12.005. [DOI] [PubMed] [Google Scholar]
- Moore R, Estis J, Hickey S. Pitch Discrimination and Pitch Matching Abilities. J Voice. 2008;22:399–407. doi: 10.1016/j.jvoice.2006.10.013. [DOI] [PubMed] [Google Scholar]
- Moore B, Moore G. Discrimination of the fundamental frequency of complex tones with fixed and shifting spectral envelopes by normally hearing and hearing-impaired subjects. Hear Res. 2003;182:153–163. doi: 10.1016/s0378-5955(03)00191-6. [DOI] [PubMed] [Google Scholar]
- Oates J, Dacakis G. Speech pathology considerations in the management of transsexualism-a review. Br J Disord Commun. 1983;18:139–151. doi: 10.3109/13682828309012237. [DOI] [PubMed] [Google Scholar]
- Raj A, Gupta B, Chowdhury A. A study in various phases of menstrual cycle and in postmenopausal women. J Voice. 2010;24:363–368. doi: 10.1016/j.jvoice.2008.10.005. [DOI] [PubMed] [Google Scholar]
- Randolph J, Sowers M, Bondarenko I. Change in estradiol and follicle-stimulating hormone across the early menopausal transition: effects of ethnicity and age. J Clin Endocrinol Metab. 2004;89:1555–1561. doi: 10.1210/jc.2003-031183. [DOI] [PubMed] [Google Scholar]
- Shower E, Biddulph R. Differential pitch sensitivity of the ear. J Am Statist Assoc. 1931;3:275–287. [Google Scholar]
- Van de Heyning P, Remacle P, Van Cauwenberghe P. Research work of the Belgian Study Group on Voice Disorders 1996. Acta oto-rhino-laryngologica Belgica. 1996;50:321–341. [Google Scholar]
- Wever E, Wedell C. Pitch discrimination at high frequencies. Psychol Bull. 1941;38:727. [Google Scholar]
- World Health Organization. Research on the Menopause in the 1990s. Report of a WHO Scientific Group. WHO Technical Report Series. 1996;(866) [PubMed] [Google Scholar]