

Abstract
We compared clinical characteristics, management, and clinical outcomes of nonagenarian acute myocardial infarction (AMI) patients (n=270, 92.3±2.3 yr old) with octogenarian AMI patients (n=2,145, 83.5±2.7 yr old) enrolled in Korean AMI Registry (KAMIR). Nonagenarians were less likely to have hypertension, diabetes and less likely to be prescribed with beta-blockers, statins, and glycoprotein IIb/IIIa inhibitors compared with octogenarians. Although percutaneous coronary intervention (PCI) was preferred in octogenarians than nonagenarians, the success rate of PCI between the two groups was comparable. In-hospital mortality, the composite of in-hospital adverse outcomes and one year mortality were higher in nonagenarians than in octogenarians. However, the composite of the one year major adverse cardiac events (MACEs) was comparable between the two groups without differences in MI or re-PCI rate. PCI improved 1-yr mortality (adjusted hazard ratio [HR], 0.50; 95% confidence interval [CI], 0.36-0.69, P<0.001) and MACEs (adjusted HR, 0.47; 95% CI, 0.37-0.61, P<0.001) without significant complications both in nonagenarians and octogenarians. In conclusion, nonagenarians had similar 1-yr MACEs rates despite of higher in-hospital and 1-yr mortality compared with octogenarian AMI patients. PCI in nonagenarian AMI patients was associated to better 1-yr clinical outcomes.
Graphical Abstract
Keywords: Aged, Eighty and over; Myocardial Infarction; Percutaneous Coronary Intervention
INTRODUCTION
With increased life expectancy, the population of the elderly is increasing, and cardiovascular disease is the major cause of mortality and morbidity in this age group (1). Although age itself is a definite high risk factor in cardiovascular disease adverse outcomes (2), those of extreme chorological age are often excluded from clinical trials of cardiovascular disease (3). Therefore, little is known about the management and outcomes of acute myocardial infarction (AMI) in this age group. Percutaneous coronary intervention (PCI) became pivotal step in the management of AMI. Also, recent advances in technology, procedural techniques, and medical therapy have resulted in improvement in PCI outcomes and enables for the elderly to have an opportunity of PCI. However, risk or benefit of PCI, and long term clinical outcomes in the nonagenarian AMI patients is still controversial. Although current guidelines recommend early coronary revascularization with PCI in patients with AMI, application to nonagenarian AMI patients only might be extrapolated from the data which have analyzed younger AMI patients, because of the paucity of data about nonagenarian AMI patients.
Under this circumstance, we investigated clinical characteristics, management and clinical outcomes in the very elderly AMI patients, especially with nonagenarians compared with relatively younger elderly AMI patients, octogenarians.
MATERIALS AND METHODS
Study population
Consecutive 14,885 patients enrolled in the Korea Acute Myocardial Infarction Registry (KAMIR; November 2005 to December 2007). A total of 2,415 AMI patients who were older than 80 yr old consisted of the study population. They were divided to two groups according to age (Nonagenarians; n=270, Octogenarians; n=2,145). The eligible patients were ≥80 yr old at admission (Nonagenarians, 90 to 99 yr old; octogenarians, 80 to 89 yr old), had suggestive symptoms with or without ST elevation >2 mm in ≥2 precordial leads, ST elevation >1 mm in ≥2 limb leads, or new left bundle branch block on the 12-lead electrocardiogram with a concomitant increases of at least one cardiac enzyme. The criteria for exclusion included malignant neoplasm, leukemia, lymphoma, and metastatic solid tumors. Clinical characteristics and in-hospital clinical outcomes were analyzed in all 2,415 eligible AMI patients. One year clinical outcomes were analyzed in 2,089 patients who survived at hospital discharge.
The KAMIR, launched in November 2005, is a Korean prospective multicenter data collection registry reflecting real-world treatment practices and outcomes in Asian patients diagnosed with AMI. The registry includes 50 community and teaching hospitals with facilities for primary PCI and on-site cardiac surgery. Data were collected by a trained study coordinator using a standardized case report form and protocol. The study protocol was approved by the ethics committee at each participating institution. All patients gave written informed consent.
Study definition and end points
AMI was diagnosed by the presence of characteristic clinical presentation, serial changes on electrocardiogram suggesting infarction, and increases in cardiac enzymes. Cardiogenic shock was as systolic blood pressure <90 mmHg with the evidence of tissue hypoperfusion. Atrioventricular (AV) block needing pacing was defined as the case which demonstrated higher than second degree AV bock needing temporary or permanent pacing. Cerebrovascular accident (CVA) was defined as a new focal neurologic defect with the proof of brain image. New onset heart failure was defined as newly developed New Yolk Heart Association class III/IV dyspnea, orthopnea, rales greater than one-third lung fields, elevated jugular venous pressure, or pulmonary congestion on chest radiograph thought to be related to cardiac dysfunction. Major bleeding was defined as an absolute hematocrit drop of ≥15%, any intracranial bleeding, bleeding events associated with causing death, the need for surgery, or transfusion, or any clinically relevant bleeding, as judged by the investigator. Minor bleeding was defined as any other bleeding which did not meet the major bleeding criteria, including vascular access complication.
During the in-hospital period, patients received medical treatment including beta blockers, angiotensin converting enzyme inhibitors or angiotensin receptor blockers and statins. After discharge, the patients continued receiving the same kinds of medications that they received in hospital period except some intravenous or temporary medications.
The composite of in-hospital adverse outcomes was defined as the composite of death, cardiogenic shock, AV block needing pacing, new onset atrial fibrillation, fatal arrhythmia, CVA, new onset heart failure, major bleeding or minor bleeding. The primary end point was the composite of major adverse cardiac events (MACEs) during the 12 months of clinical follow-up. MACEs was defined as the composite of all-cause death, MI, and repeated PCI or coronary artery bypass grafting (CABG). All-cause deaths were considered cardiac death unless a non-cardiac death could be defined clearly. Recurrent MI was defined as recurrent symptoms with new electrocardiographic changes compatible with MI or cardiac markers at least twice the upper limit of normal. Target-vessel revascularization (TVR) was defined as any repeated intervention driven by the lesions located in the treated vessel within and beyond the target limits.
Statistical analysis
All statistical analyses were done with SPSS 18.0 (Statistical Package for the Social Sciences, SPSS-PC Inc., Chicago, IL, USA). For continuous variables, differences between groups were evaluated by an unpaired t-test or Mann-Whitney rank-sum test. For discrete variables, differences were expressed as counts and percentages, and were analyzed with a chi-square test (or Fisher's extract) between groups as appropriate. We constructed Kaplan-Meier curves to the composite of the primary end point, as well as all cause death, cardiac death, and repeated PCI. The differences between the groups were assessed by log-rank test. A propensity score for performing PCI was calculated to adjust potential confounders using a logistic regression model. All available variables considered potentially relevant were included: gender, hypertension, diabetes mellitus, dyslipidemia, smoking, family history of coronary heart disease, previous history of angina, MI, PCI, CABG, chronic kidney disease (CKD), CVA, peripheral vascular disease, heart failure, Killip class on presentation, and left ventricular ejection fraction. Cox proportional hazards regression was used to compute hazard ratio (HR) as estimates for each end point. The HRs were adjusted for propensity score and concomitant medications. The predicted accuracy of the logistic model was assessed using the area under the receiver operating characteristic curve (c statistic), which was 0.720. All analyses were 2-tailed, with clinical significance defined as values of P<0.05.
Ethics statements
The study was conducted according to the Declaration of Helsinki. The institutional review board of all paticipating centers approved the study protocol. The approval number was I-2008--1-009 of Chonnam National University Hospital. Written informed consent was obtained from all participating patients.
RESULTS
Baseline clinical characteristics
Mean age of nonagenarians were 92.3±2.3 yr old, whereas that of octogenarians were 83.5±2.7 yr old. Vital sign at hospital admission were not different between the 2 groups. More octogenarians complained typical chest pain (75.8% vs 68.9%, P=0.013), whereas more nonagenarians complained dyspnea (45.5% vs 38.9%, P=0.038) and nonagenarians had higher Killip classification (≥3 on presentation: 31.2% vs 21.6%, P=0.001). Nonagenarians were less likely to have hypertension (46.7% vs 57.5%, P=0.001), diabetes (15.6% vs 27.9%, P<0.001) compared with octogenarians. No significant differences in other previous medical history were found between the 2 groups except that nonagenarians had higher incidence of past history of heart failure. Also, left ventricular systolic function in nonagenarians was lower than that of octogenarian (45.0% vs 49.0%, P<0.001). Laboratory findings were comparable between the groups except that serum level of low density lipoprotein-cholesterol was higher in octogenarians. The use beta-blockers, statins and glycoprotein IIb/IIIa inhibitors were lower in nonagenarians during admission. The use of clopidogrel, beta-blockers, and statins were lower in nonagenarians at discharge (Table 1).
Table 1.
Baseline clinical characteristics
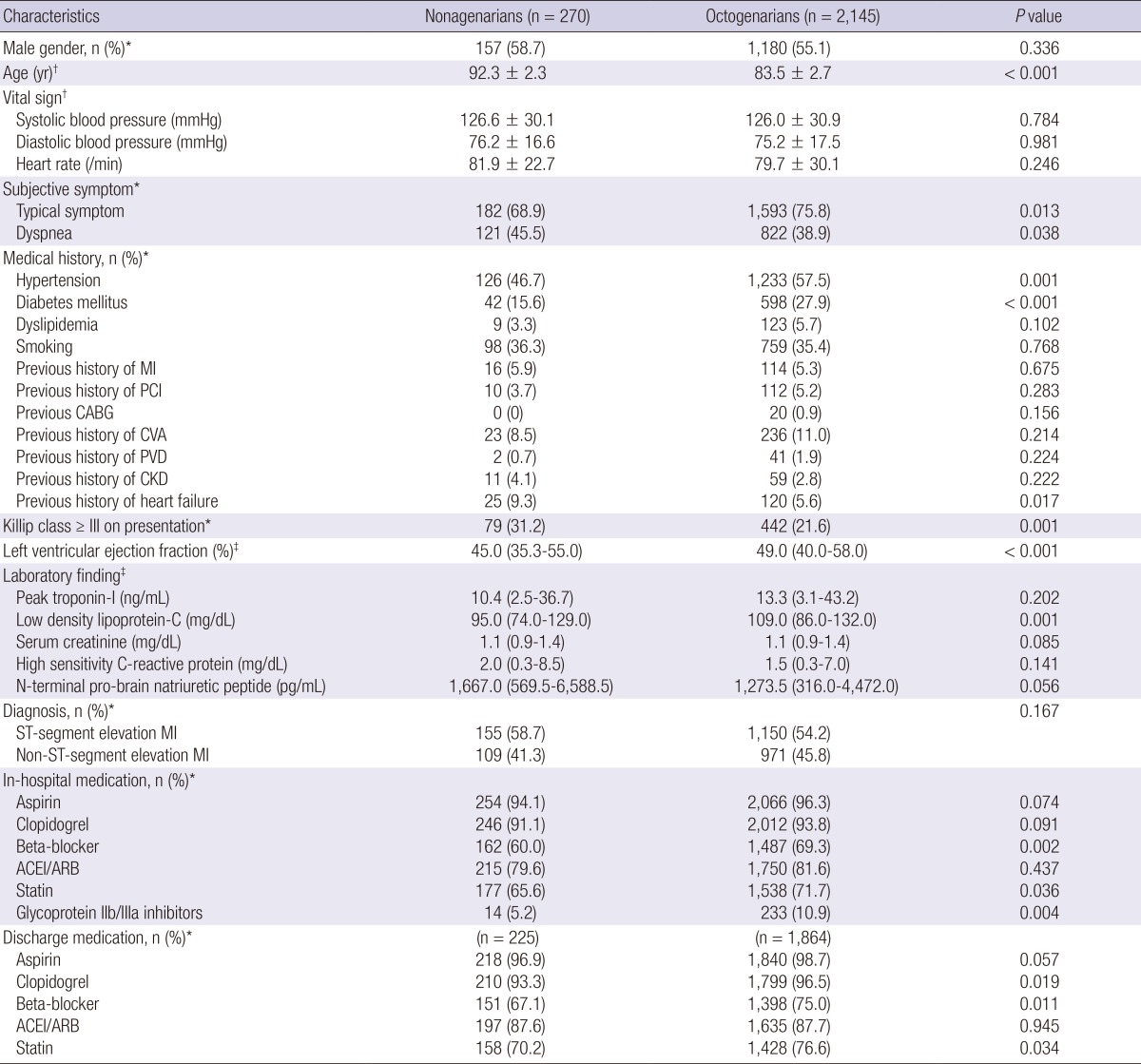
*Comparison made using chi-square test; †Mean (standard deviation); comparison made using t-test; ‡Median (25% to 75% percentiles); comparison made using Mann-Whitney test. CABG, coronary artery bypass grafting; CKD, chronic kidney disease; CVA, cerebrovascular accidents; MI, myocardial infarction; PCI, percutaneous coronary intervention; PVD, peripheral vascular disease.
Procedural characteristics
A total of 1,682 (70.1%) patients underwent PCI, which was more commonly undergone in octogenarians than nonagenarians (71.7% vs 57.2%, P<0.001). However, the success rate of PCI was comparable in both groups (96.7% vs 96.8%, P=0.984). Patients who underwent PCI presented more typical chest pain (81.4% vs 60.2%, P<0.001), and less dyspnea (34.3% vs 51.7%, P<0.001). Patients who did not undergo PCI had higher prevalence of past history of MI, PCI, CVA, CKD, heart failure, high Killip class (≥3 on presentation), and more presented as non ST-segment elevation MI (NSTEMI) (Table 2). In patients with STEMI, 244 (18.8%) patients did not underwent PCI. 19 (1.5%) patients refused PCI, whereas 117 (9.0%) patients were not indicated or poor candidate for PCI decided by physicians.
Table 2.
Baseline clinical characteristics according to PCI
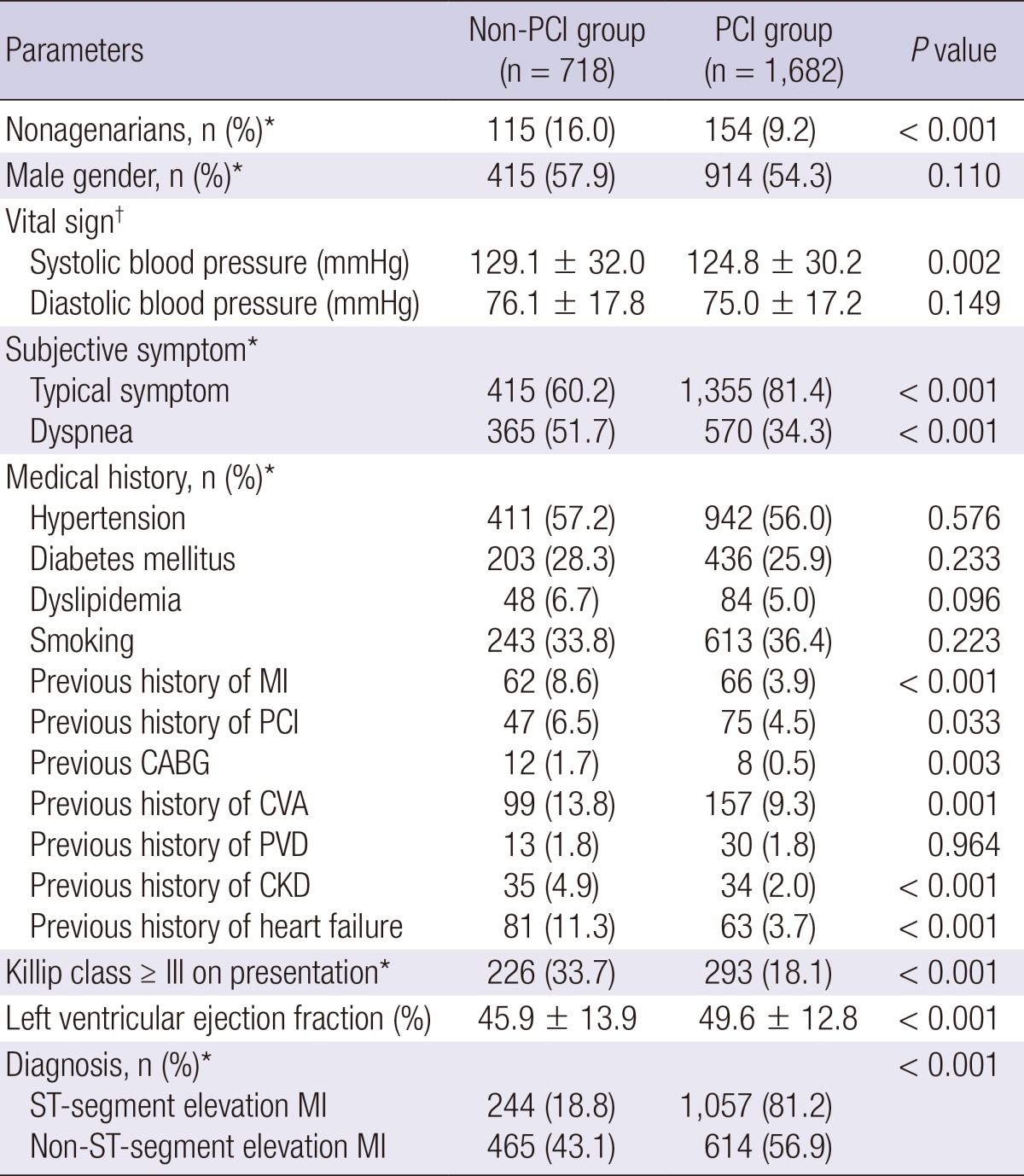
*Comparison made using chi-square test; †Mean (standard deviation), comparison made using t-test. CABG, coronary artery bypass grafting; CKD, chronic kidney disease; CVA, cerebrovascular accidents; MI, myocardial infarction; PCI, percutaneous coronary intervention; PVD, peripheral vascular disease.
Analysis of angiographic findings showed no differences in location of culprit lesions, prevalence of multi-vessel disease, American College of Cardiology/American Heart Association (ACC/AHA) lesion type, distribution of pre- and post-procedural Thrombolysis In Myocardial Infarction (TIMI) flow grade, stent type, length, and stent diameter between the nonagenarians and octogenarians (Table 3).
Table 3.
Procedural characteristics
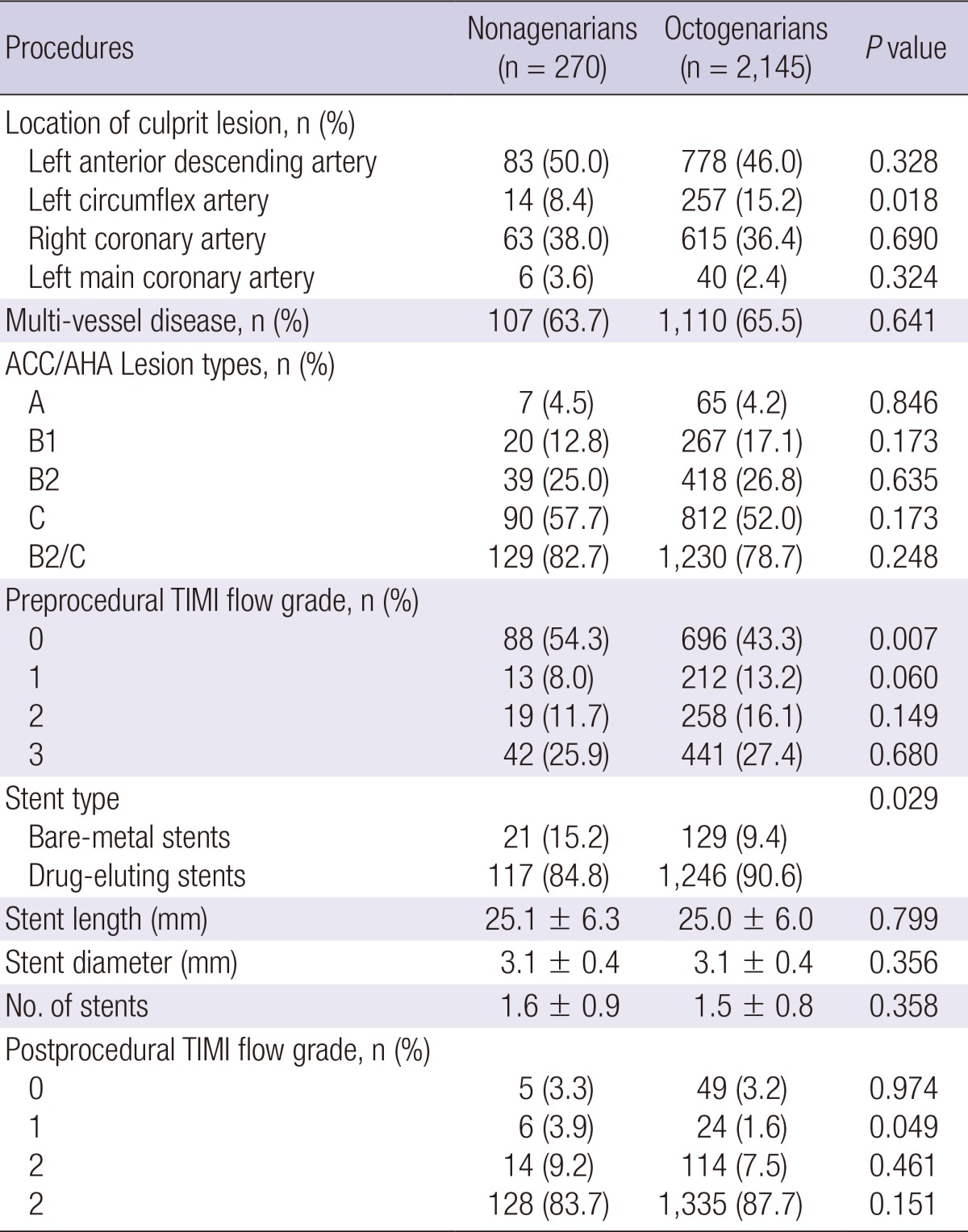
ACC/AHA, American College of Cardiology/American Heart Association; TIMI, Thrombolysis In Myocardial Infarction.
In-hospital outcomes
Compared with octogenarians, nonagenarians had higher death rate during hospitalization (15.7% vs 11.4%, P=0.041), and the composite of in-hospital adverse outcomes (26.3% vs 20.0%, P=0.017). These differences were persisted even after adjustment for potential confounding factors with adjusted hazard ratio (HR) of 1.68 (95% confidence interval [CI], 1.11-2.52; P=0.013) for death, and 1.56 (95% CI, 1.13-2.15; P=0.007) for the composite of in-hospital averse outcomes. However, the individual risk for cardiogenic shock, AV block needing pacing, fatal arrhythmia, new onset CVA, new onset heart failure, minor bleeding, major bleeding were compatible between the 2 groups, and also similar between the 2 groups after adjustment (Table 4). PCI did not reduce in-hospital mortality and the composite of in-hospital adverse outcomes both in nonagenarians and octogenarians (Fig. 1).
Table 4.
In-hospital outcomes
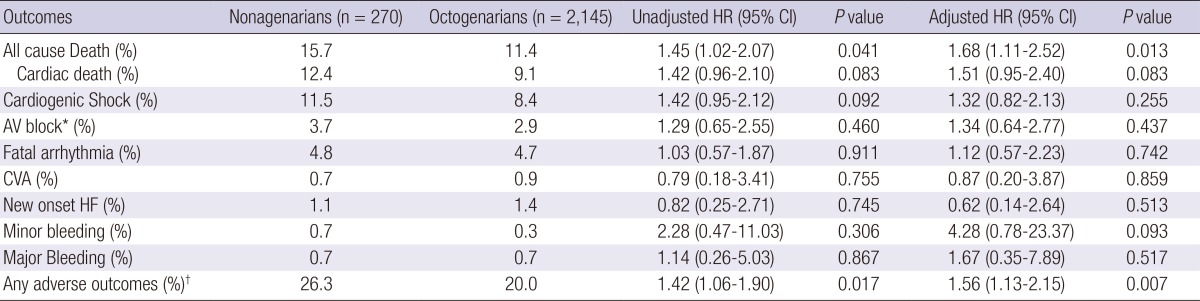
*AV block, atrioventricular block needing pacing; †any adverse outcomes, death, cardiogenic shock, AV block needing pacing, new onset atrial fibrillation, fatal arrhythmia, cerebrovascular accidents, new onset heart failure, minor bleeding, or major bleeding. CI, confidence interval; CVA, cerebrovascular accidents; HF, heart failure; HR, hazard ratio.
Fig. 1.

Estimates of the clinical outcomes according to percutaneous coronary intervention (PCI).
One year clinical outcomes
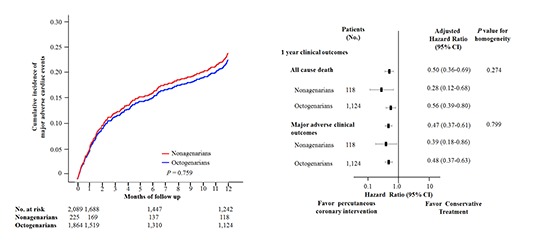
During the 12 month follow-up period, a primary end point event occurred in 24.6% of nonagenarians and 22.2% of octogenarians (log-rank P=0.759; Fig. 2A). Adjustment for propensity score, and treatment parameters also showed no difference in the primary end point between the 2 groups (HR, 1.25; 95% CI, 0.62-2.51; P=0.528; Table 5). Outcomes for the selected end points are shown in Table 5. Compared with octogenarians, nonagenarians had significantly higher all cause death rate (20.3% vs 12.2%, log-rank P=0.032; Fig. 2B). However, this difference disappeared after adjustment. Cardiac death occurred in 13.6% of nonagenarians, and in 8.1% of octogenarians (Fig. 2C). MI occurred in 0.8% of nonagenarians, and in 3.0% of octogenarians. Repeated PCI occurred in 4.2% of nonagenarians, and in 5.7% of octogenarians (Fig. 2D). Adjusted HR for cardiac death, MI, repeated PCI were not different between the 2 groups. PCI reduced the primary end point (HR, 0.47; 95% CI, 0.37-0.61; P<0.001) and 1-yr all cause death (HR, 0.50; 95% CI, 0.36-0.69; P<0.001) both in nonagenarians and octogenarians (Fig. 1).
Fig. 2.

Estimates of the clinical outcomes according to age group. (A) Cumulative incidence of major adverse cardiac events (MACEs). (B) Cumulative incidence of all cause death. (C) Cumulative incidence of cardiac death. (D) Cumulative incidence of repeated percutaneous coronary intervention (PCI).
Table 5.
Estimated hazard ratio for individual components of the primary endpoints

CABG, coronary artery bypass grafting; CI, confidence interval; HR, hazard ratio; MACE, major adverse cardiac events; MI, myocardial infarction; PCI, percutaneous coronary intervention; TVR, target vessel revascularization.
Clinical outcomes according to the diagnosis of ST-segment elevation myocardial infarction and non ST-segment elevation myocardial infarction
In nonagenarians, patients with STEMI had significantly higher in-hospital cardiac death rate than patients with NSTEMI (16.1% vs 7.3%, P=0.033) without differences in the rates of in-hospital all-cause death, and 1-yr all-cause death, MI, repeated PCI, CABG and MACEs.
In octogenarians, patients with STEMI had significantly higher in-hospital cardiac (11.8% vs 5.7%, P<0.001) and all-cause death rate (14.4% vs 7.8%, P<0.001) than patients with NSTEMI. In 1-yr clinical outcomes, patients with NSTEMI had significantly higher MI (1.7% vs 4.6%, log-rank P=0.002) and total MACE rates (19.7% vs 25.0%, log-rank P=0.019) than patients with STEMI without differences in the rates of all-cause death, repeated PCI and CABG (Table 6).
Table 6.
Clinical outcomes according to the diagnosis of ST-segment elevation myocardial infarction and non ST-segment elevation myocardial infarction
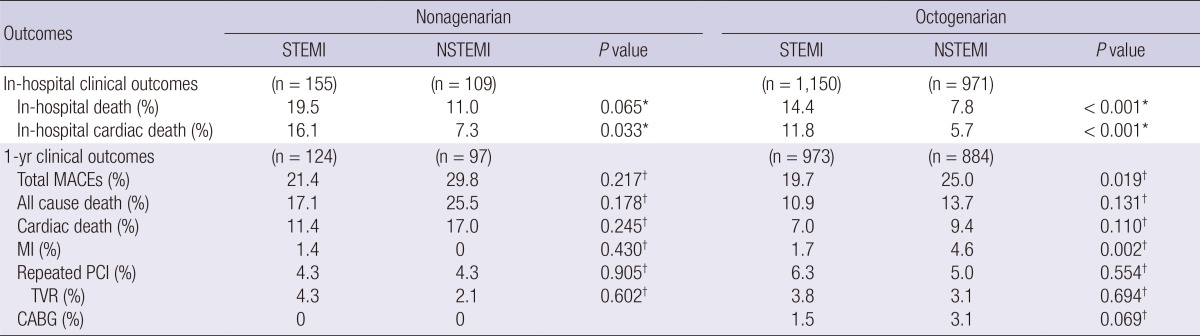
*Comparison made using chi-square test; †Comparison made using log-rank test. CABG, coronary artery bypass grafting; MACE, major adverse cardiac events; MI, myocardial infarction; NSTEMI, non ST-segment elevation myocardial infarction; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction; TVR, target vessel revascularization.
DISCUSSION
The elderly constitute an increasing segment of the population and cardiovascular disease is highly prevalent among them, accounting for most of their morbidity and mortality (1). The elderly carries higher prevalence of cardiovascular morbidities such as diabetes mellitus, hypertension and mortalities, which rank the leading cause of death among them (4, 5, 6, 7). Approximately one third of the elderly die as a direct consequence of coronary atherosclerosis (8). Especially, AMI in the elderly might be quite lethal to them. However, there is little known about the management, clinical outcomes according to the initial management in the very elderly AMI patients, because most of clinical trials were based on relatively younger patients, and the population of the very elderly AMI patients constitute very small portion. Furthermore, there have been few reports regarding nonagenarian AMI patients. Although both octogenarian and nonagenarian AMI patients were considered as the very elderly population, there might be differences between the two groups, and even physicians might approach to them with different treatment attitude. Therefore, the present study compared clinical characteristics, management, and long term outcomes between nonagenarian and octogenarian AMI patients in the contemporary PCI era.
Nonagenarians or centenarians present different clinical characteristics compared with younger elderly populations (9). In the present study, nonagenarian AMI patients were less likely to have hypertension and diabetes compared with octogenarian AMI patients. This may partially explain successful aging in nonagenarians. However, in-hospital mortality and adverse clinical outcomes were higher in nonagenarian AMI patients compared with octogenarian AMI patients. These might be attributable to the special physiologic and functional status of very old people. With increasing age, they have weaker physiologic and functional status, and are prone to develop complications by cardiovascular medications. This might limit clinicians to use all recommended cardiovascular medications in nonagenarian AMI patients.
Although advanced age is not the contraindication of PCI in patients with AMI, current guidelines describe that the elderly are at increased risk from coronary revascularization procedures, and that is usually quite challengeable to interventionists because of peri-procedural comorbidities and complications accompanying with extreme old age (10). In the present study, PCI did not increase any in-hospital adverse outcomes including minor bleeding, and major bleeding both in nonagenarians and octogenarians. Also, PCI success rate was 96.7% in octogenarians, 96.8% in nonagenarians, which were similar to that of previous reports in Korea which analyzed AMI patients in all range of age (11, 12, 13, 14). That was even higher than previous reports (15, 16, 17, 18, 19). From et al. reported nonagenarian PCI success rate as 91% in 2008 (19). The growing interest in PCI, advances in technology and procedural techniques might contribute to the improved PCI success rate in the contemporary era. Also, repeated PCI rate were not different between nonagenarian and octogenarians AMI patients. Nonetheless, in patients with STEMI, 244 (18.8%) patients did not undergo PCI in the present study. Furthermore, 117 (9.0%) patients were frustrated PCI by physicians' decision, while 19 (1.5%) patients refused PCI, 51 (3.9%) patients were planned to perform CABG, and 57 (4.4%) patients underwent thrombolysis. It might involve physicians' bias or patient preference, and exaggerated perceived bleeding risk by extreme old age. The present study showed that the elderly could get comparable PCI success rate, if they did not have contraindication undergoing PCI. These findings suggest that PCI should not be frustrated only because of old age.
The elderly have known to have more complex coronary lesions (20, 21, 22). In the present study, almost 80% of both nonagenarians and octogenarians have ACC/AHA lesion type B2 or C. Also, almost 65% of both nonagenarians and octogenarians have multivessel disease. However, there were no significant differences in angiographic findings between nonagenarians and octogenarians. Furthermore, PCI success rate and achieving post-procedural TIMI flow grade 3 were similar. These result might suggest that PCI in nonagenarian AMI patients is not much difficult technically compared with PCI in octogenarian AMI patients.
The present study showed that PCI both in nonagenarian and octogenarian AMI patients was associated to better outcomes. Although PCI improved in-hospital death only in octogenarians, it improved 1 yr MACEs without increasing complications both in octogenarians and nonagenarians. Major or minor bleeding rate of PCI group was also comparable with that of non-PCI group. This was consistent with the CRUSADE trial which reported that early coronary revascularization improved in-hospital mortality over more than 5,000 nonagenarian NSTEMI-acute coronary syndrome patients (10). From et al. also reported PCI in nonagenarian patients improved in-hospital mortality and MACEs (19). Long term survival of nonagenarians was similar to age- and gender-matched control subjects during median 3.6 yr follow-up. However, none of the previous studies analyzed the efficacy of PCI in nonagenarian AMI patients more than 1 yr follow-up duration. The present study added the evidence of beneficial effect of PCI in the management of elderly AMI patients.
The present study has several limitations. First, management strategy was left to the discretion of the operators. They might regard the general physiologic status as the higher risk profiles than chronogical age. Therefore, there might be a selection bias for PCI in favor of lower risk rather than chronological age. Second, the present study did not compare the relatively elderly AMI patients (i.e. septuagenarians) and the extreme old age AMI patients (i.e. octogenarians or nonagenarians). Therefore, it was hard to evaluate risk/benefit ratio of PCI according to selected age group. Third, all-cause death was defined as cardiac death a non-cardiac death could be defined clearly. Lots of mortality causes of very old patients include frailty, terminal disease, and organ failures, and sudden death. Therefore, some patients designated as having cardiac death might have non-cardiac cause of death actually. Fourth, the present study was analyzed retrospectively. The non-randomized nature of the registry data could have resulted in selection bias. Although most confounders were included in the multivariate regression analysis, it is possible that some potential bias were included. Large scale prospective randomized study is needed to clarify the benefits of PCI in the verly elderly AMI patients. Nonetheless, the present study have strengths in that non-randomized design of this study included many patients who would not have been enrolled in randomized trials, including those with severe comorbidities. Also the present study had strengths in that the study represented real world management trends in the very elderly AMI patients, not limited to the patients undergoing PCI like as most of other studies.
Appendix 1
The Korea Acute Myocardial Infarction Registry (KAMIR) Study Group of the Korean Circulation Society was as follows: Myung Ho Jeong, Chonnam National University Hospital, Gwangju; Young Jo Kim, Yeungnam University Hospital, Daegu; Chong Jin Kim, East West Neo Medical Center, Seoul; Myeong Chan Cho, Chungbuk National University Hospital, Chungju; Youngkeun Ahn, Chonnam National University Hospital, Gwangju; Jong Hyun Kim, Hanseo Hospital, Busan; Shung Chull Chae, Kyungbook National University Hospital, Daegu; Seung Ho Hur, Keimyung University Dongsan Medical Center, Daegu; In Whan Seong, Chungnam National University Hospital, Daejeon; Taek Jong Hong, Pusan National University Hospital, Busan; Dong Hoon Choi, Yonsei Cardiovascular center, Seoul; Jei Keon Chae, Chonbuk National University Hospital, Jeonju; Jae Young Rhew, Presbyterian Medical Center, Jeonju; Doo Il Kim, Inje University Busan Paik Hospital, Busan; In Ho Chae, Seoul National University Bundang Hospital, Seoul; Jung Han Yoon, Wonju Severance Christian Hospital, Wonju; Bon Kwon Koo, Seoul National University Hospital, Seoul; Byung Ok Kim, Inje University Sanggye Paik Hospital, Seoul; Myoung Yong Lee, Dankook University Hospital, Cheonan; Kee Sik Kim, Daegu Catholic University Medical Center, Daegu; Jin Yong Hwang, Gyeongsang National University Hospital, Jinju; Seok Kyu Oh, Wonkwang University Hospital, Iksan; Nae Hee Lee, Soon Chun Hyang University Hospital, Bucheon; Kyoung Tae Jeong, Eulji University Hospital, Daejeon; Seung Jea Tahk, Ajou University Hospital, Suwon; Jang Ho Bae, Konyang University Hospital, Daejeon; Seung Woon Rha, Korea University Guro Hospital, Seoul; Keum Soo Park, Inha University Hospital, Incheon; Kyoo Rok Han, Hallym University Kangdong Medical Center, Seoul; Tae Hoon Ahn, Gachon University Gil Medical Center, Incheon; Moo Hyun Kim, Dong-A University Hospital, Busan; Joo Young Yang, National Health Insurance Service Ilsan Hospital, Goyang; Chong Yun Rhim, Hallym University Medical Center, Seoul; Hyeon Cheol Gwon, Samsung Medical Center, Seoul; Seong Wook Park, Asan Medical Center, Seoul; Young Youp Koh, Chosun University Hospital, Gwangju; Seung Jae Joo, Jeju National University Hospital, Jeju; Soo Joong Kim, Kyunghee University Medical Center, Seoul; Dong Kyu Jin, Soon Chun Hyang University Hospital, Cheonan; Jin Man Cho, Kyunghee University Hospital, Seoul; Wook Sung Chung, Catholic University Hospital, Seoul; Yang Soo Jang, Yonsei Cardiovascular Center, Seoul; Jeong Gwan Cho, Chonnam National University Hospital, Gwangju; Ki Bae Seung, Catholic University Hospital, Seoul; and Seung Jung Park, Asan Medical Center, Seoul.
Footnotes
This work was supported by a grant of the National Research Foundation of Korea funded by the Korean Government (MEST), Republic of Korea (2010-0020261), and by a grant of the Korea Healthcare Technology R&D Project, Ministry for Health & Welfare, Republic of Korea (HI12C0275, HI12C0199, HI13C1527).
There are no potential conflicts to declare.
References
- 1.Avezum A, Makdisse M, Spencer F, Gore JM, Fox KA, Montalescot G, Eagle KA, White K, Mehta RH, Knobel E, et al. Impact of age on management and outcome of acute coronary syndrome: observations from the Global Registry of Acute Coronary Events (GRACE) Am Heart J. 2005;149:67–73. doi: 10.1016/j.ahj.2004.06.003. [DOI] [PubMed] [Google Scholar]
- 2.Singh M, Rihal CS, Lennon RJ, Garratt KN, Mathew V, Holmes DR., Jr Prediction of complications following nonemergency percutaneous coronary interventions. Am J Cardiol. 2005;96:907–912. doi: 10.1016/j.amjcard.2005.05.045. [DOI] [PubMed] [Google Scholar]
- 3.Lee PY, Alexander KP, Hammill BG, Pasquali SK, Peterson ED. Representation of elderly persons and women in published randomized trials of acute coronary syndromes. JAMA. 2001;286:708–713. doi: 10.1001/jama.286.6.708. [DOI] [PubMed] [Google Scholar]
- 4.Batchelor WB, Anstrom KJ, Muhlbaier LH, Grosswald R, Weintraub WS, O'Neill WW, Peterson ED. Contemporary outcome trends in the elderly undergoing percutaneous coronary interventions: results in 7,472 octogenarians: National Cardiovascular Network Collaboration. J Am Coll Cardiol. 2000;36:723–730. doi: 10.1016/s0735-1097(00)00777-4. [DOI] [PubMed] [Google Scholar]
- 5.Floyd KC, Jayne JE, Kaplan AV, Friedman BJ, Niles NW, Hettleman BD, Robb JF, Thompson CA. Age-based differences of percutaneous coronary intervention in the drug-eluting stent era. J Interv Cardiol. 2006;19:381–387. doi: 10.1111/j.1540-8183.2006.00192.x. [DOI] [PubMed] [Google Scholar]
- 6.Klein LW, Block P, Brindis RG, McKay CR, McCallister BD, Wolk M, Weintraub W ACC-NCDR Registry. Percutaneous coronary interventions in octogenarians in the American College of Cardiology-National Cardiovascular Data Registry: development of a nomogram predictive of in-hospital mortality. J Am Coll Cardiol. 2002;40:394–402. doi: 10.1016/s0735-1097(02)01992-7. [DOI] [PubMed] [Google Scholar]
- 7.Cohen HA, Williams DO, Holmes DR, Jr, Selzer F, Kip KE, Johnston JM, Holubkov R, Kelsey SF, Detre KM NHLBI Dynamic Registry. Impact of age on procedural and 1-year outcome in percutaneous transluminal coronary angioplasty: a report from the NHLBI Dynamic Registry. Am Heart J. 2003;146:513–519. doi: 10.1016/S0002-8703(03)00259-X. [DOI] [PubMed] [Google Scholar]
- 8.Roberts WC, Shirani J. Comparison of cardiac findings at necropsy in octogenarians, nonagenarians, and centenarians. Am J Cardiol. 1998;82:627–631. doi: 10.1016/s0002-9149(98)00385-3. [DOI] [PubMed] [Google Scholar]
- 9.Galioto A, Dominguez LJ, Pineo A, Ferlisi A, Putignano E, Belvedere M, Costanza G, Barbagallo M. Cardiovascular risk factors in centenarians. Exp Gerontol. 2008;43:106–113. doi: 10.1016/j.exger.2007.06.009. [DOI] [PubMed] [Google Scholar]
- 10.Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE, Jr, Chavey WE, 2nd, Fesmire FM, Hochman JS, Levin TN, et al. 2012 ACCF/AHA focused update incorporated into the ACCF/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61:e179–e347. doi: 10.1016/j.jacc.2013.01.014. [DOI] [PubMed] [Google Scholar]
- 11.Lee KH, Jeong MH, Ahn YK, Kim JH, Chae SC, Kim YJ, Hur SH, Seong IW, Hong TJ, Choi D, et al. Gender differences of success rate of percutaneous coronary intervention and short term cardiac events in Korea Acute Myocardial Infarction Registry. Int J Cardiol. 2008;130:227–234. doi: 10.1016/j.ijcard.2007.08.044. [DOI] [PubMed] [Google Scholar]
- 12.Cho Y, Yang HM, Park KW, Chung WY, Choi DJ, Seo WW, Jeong KT, Chae SC, Lee MY, Hur SH, et al. Paclitaxel- versus sirolimus-eluting stents for treatment of ST-segment elevation myocardial infarction: with analyses for diabetic and nondiabetic subpopulation. JACC Cardiovasc Interv. 2010;3:498–506. doi: 10.1016/j.jcin.2010.02.011. [DOI] [PubMed] [Google Scholar]
- 13.Cho KH, Jeong MH, Ahn Y, Kim YJ, Chae SC, Hong TJ, Seong IW, Chae JK, Kim CJ, Cho MC, et al. Low-density lipoprotein cholesterol level in patients with acute myocardial infarction having percutaneous coronary intervention (the cholesterol paradox) Am J Cardiol. 2010;106:1061–1068. doi: 10.1016/j.amjcard.2010.06.009. [DOI] [PubMed] [Google Scholar]
- 14.Lee KH, Jeong MH, Kim HM, Ahn Y, Kim JH, Chae SC, Kim YJ, Hur SH, Seong IW, Hong TJ, et al. Benefit of early statin therapy in patients with acute myocardial infarction who have extremely low low-density lipoprotein cholesterol. J Am Coll Cardiol. 2011;58:1664–1671. doi: 10.1016/j.jacc.2011.05.057. [DOI] [PubMed] [Google Scholar]
- 15.Skolnick AH, Alexander KP, Chen AY, Roe MT, Pollack CV, Jr, Ohman EM, Rumsfeld JS, Gibler WB, Peterson ED, Cohen DJ. Characteristics, management, and outcomes of 5,557 patients age > or =90 years with acute coronary syndromes: results from the CRUSADE Initiative. J Am Coll Cardiol. 2007;49:1790–1797. doi: 10.1016/j.jacc.2007.01.066. [DOI] [PubMed] [Google Scholar]
- 16.Teplitsky I, Assali A, Lev E, Brosh D, Vaknin-Assa H, Kornowski R. Results of percutaneous coronary interventions in patients > or =90 years of age. Catheter Cardiovasc Interv. 2007;70:937–943. doi: 10.1002/ccd.21263. [DOI] [PubMed] [Google Scholar]
- 17.Sakai K, Nagayama S, Ihara K, Ando K, Shirai S, Kondo K, Yokoi H, Iwabuchi M, Nosaka H, Nobuyoshi M. Primary percutaneous coronary intervention for acute myocardial infarction in the elderly aged ≥75 years. Catheter Cardiovasc Interv. 2012;79:50–56. doi: 10.1002/ccd.22810. [DOI] [PubMed] [Google Scholar]
- 18.Moreno R, Salazar A, Bañuelos C, Hernández R, Alfonso F, Sabaté M, Escaned J, Pérez MJ, Azcona L, Macaya C. Effectiveness of percutaneous coronary interventions in nonagenarians. Am J Cardiol. 2004;94:1058–1060. doi: 10.1016/j.amjcard.2004.06.068. [DOI] [PubMed] [Google Scholar]
- 19.From AM, Rihal CS, Lennon RJ, Holmes DR, Jr, Prasad A. Temporal trends and improved outcomes of percutaneous coronary revascularization in nonagenarians. JACC Cardiovasc Interv. 2008;1:692–698. doi: 10.1016/j.jcin.2008.07.009. [DOI] [PubMed] [Google Scholar]
- 20.Morrison DA, Bies RD, Sacks J. Coronary angioplasty for elderly patients with "high risk" unstable angina: short-term outcomes and long-term survival. J Am Coll Cardiol. 1997;29:339–344. doi: 10.1016/s0735-1097(96)00495-0. [DOI] [PubMed] [Google Scholar]
- 21.De Gregorio J, Kobayashi Y, Albiero R, Reimers B, Di Mario C, Finci L, Colombo A. Coronary artery stenting in the elderly: short-term outcome and long-term angiographic and clinical follow-up. J Am Coll Cardiol. 1998;32:577–583. doi: 10.1016/s0735-1097(98)00287-3. [DOI] [PubMed] [Google Scholar]
- 22.DeGeare VS, Stone GW, Grines L, Brodie BR, Cox DA, Garcia E, Wharton TP, Boura JA, O'Neill WW, Grines CL. Angiographic and clinical characteristics associated with increased in-hospital mortality in elderly patients with acute myocardial infarction undergoing percutaneous intervention (a pooled analysis of the primary angioplasty in myocardial infarction trials) Am J Cardiol. 2000;86:30–34. doi: 10.1016/s0002-9149(00)00824-9. [DOI] [PubMed] [Google Scholar]