

Abstract
This study aimed to evaluate the clinical value of a novel ureter dilatation method during ureteroscopic pneumatic lithotripsy in patients with ureteral calculi and polyps. Clinical information of 86 patients with ureter calculi and polyps who underwent ureteroscopic pneumatic lithotripsy was reviewed. A cavity-distention machine was used in 44 cases to inject normal saline for keeping clear operation view (cavity-distention machine-assisted group). A high handled water bag with artificial water injection (traditional pneumatic lithotripsy group) was used in 42 cases. The total operation time, time of stone removal, stone clearance rate and surgery complications were compared between two groups. All operations were successful with no patients transferred to open surgery. No ureter breakage or avulsion occurred in two groups. Two patients in traditional pneumatic lithotripsy group suffered from ureter perforation. In cavity-distention machine-assisted group and traditional pneumatic lithotripsy group, the total operation time was 30.1±4.8 min and 36.2±6.0 min, respectively (t=-5.22, P<0.01); the time of stone removal was 6.4±1.3 min and 9.3±1.5 min, respectively (t=-9.59, P<0.01); the stone clearance rate was 100% (44/44) and 95.2% (40/42; upper ureter stone immigrated to the renal pelvis in 2, and extraorgan shock wave lithotripsy was performed), respectively. Thus, intraoperative infusion of saline with a cavity-distention machine may replace the hydromantic perfusion pump to maintain a clear operation view and favor the stone removal in lesser time. This method has important clinical value in the treatment of ureteral calculi and polyps.
Keywords: Urinary tract calculi, lithotripsy, cavity-distention machine, ureteroscopy, fibroepithelial polyps
Introduction
With the development of advanced instruments and endourologic techniques, ureteroscopic lithotripsy has gradually replaced the open surgery for the treatment of ureteral stones. Extracorporeal shock wave lithotripsy (ESWL) has been traditionally preferred due to less invasiveness, convenience, minimal anesthesia and better acceptance, while ureteroscopy is considered a favored approach with a higher stone-free rate and a lower complication rate, and the introduction of holmium laser has resulted in the improvements of therapeutic outcomes [1-3]. However, treatment of fibroepithelial polyps of the ureter accompanied by urinary tract calculi is still difficult during the intracorporeal lithotripsy [4]. Hydromantic perfusion pump is usually used in this procedure for its clear view and high success rate during the treatment of ureteral stones. In most areas of China, urologists use a high handled water bag with artificial water injection for economic concern. Herein, this study was to report our experience in the management of urinary tract calculi with polyps using cavity-distention machine and artificial water injection for ureteroscopic lithotripsy.
Patients and methods
Patients
Between December 2008 and December 2011, 86 consecutive patients (median age: 35.9 years; range: 27-65 years) with fibroepithelial polyps and urinary tract calculi who underwent ureteroscopic lithotripsy in our department were enrolled into this study. The study was approved by the Institutional Ethical Committee of our hospital and the complete medical records of these patients were reviewed. All patients were evaluated before treatment by medical history reviewing, physical examination, laboratory examinations (including urinalysis, urine culture, and renal function test), and imaging examinations (ultrasonography, plain X-ray of the kidneys, ureter and bladder, and intravenous urography).
All endoscopic procedures were performed by the same surgeon under the combined spinal-epidural anesthesia (CSEA) or general anesthesia. A urine sample was obtained for cytology. Patients were randomly divided into cavity-distention machine-assisted group in which ureteroscopic lithotripsy was performed by using a cavity-distention machine to inject normal saline and traditional group in which a high handled water bag with artificial water injection. The pressure of cavity-distention machine (Figure 1) was set at 100-120 mmHg, and the flow rate was 300-450 ml/min. The surgeon controlled the water flow rate according to the degree of ureter dilatation and the operative field definition. In the traditional group, the sterile normal saline perfusion fluid was hung 80-100 cm above the bed. If the surgical site was poorly exposed, an extension tube was set aside by the assistant bolus injection of saline to maintain a clear operative view.
Figure 1.
OLYMPUS uteromat fluid control.
Surgical procedures
All procedures were performed in the dorsal lithotomy position, and intravenous antibiotic prophylaxis was administered peri-operatively. Ureteroscopic lithotripsy was performed using an 8/9.8-rigid ureteroscope (Olympus, Japan). After placement of a safety guide wire, the rigid endoscope was inserted along the guide wire under the direct vision. Once the ureteral stone was reached, the diagnosis of FEP was based on direct visualization of the lesion with ureterorenoscopy, cold-cup biopsy, and histology. Usually, polyps are wrapped and below the stones, chrysanthemum petals, long strips, mulberry-like meat or columnar, gray or pink, pedunculated, partial ureteral wall was inflammatory thickening of the change (Figure 2). If the polyps were covered by stones and affected the gravel, forceps were used with rotation clamp to remove the stones (Figure 3). Intracorporeal lithotripsy was performed by WAZL Elektronik lithotripsy (EL27-EKL, 50-60 Hz, 70 mJ) and the energy could be adjusted depending on the efficacy of lithotripsy until the fragments were smaller than 2 mm (Figure 4). Continuous irrigation or intermittent manual pumping of irrigation to obtain a clear ureteroscopic view was used as above described. All patients underwent complete ureteropyeloscopy at the end of stone manipulations. Basket retrieval of polypoid fragments was used if necessary. A 4.8-F double-J stent was placed and indwelled for 4-6 weeks.
Figure 2.
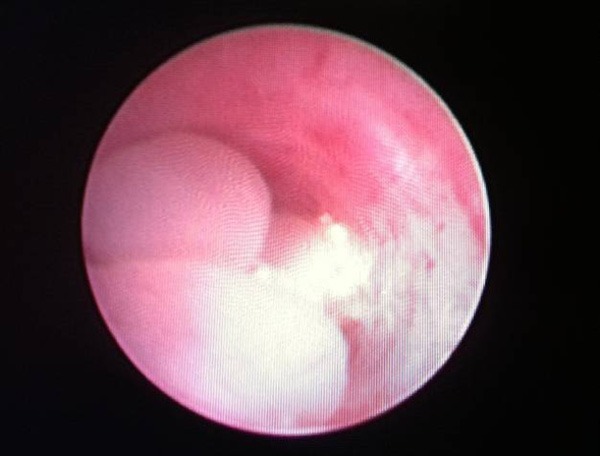
Morphological characteristics of ureteral stones polyps under ureteroscopic examination.
Figure 3.
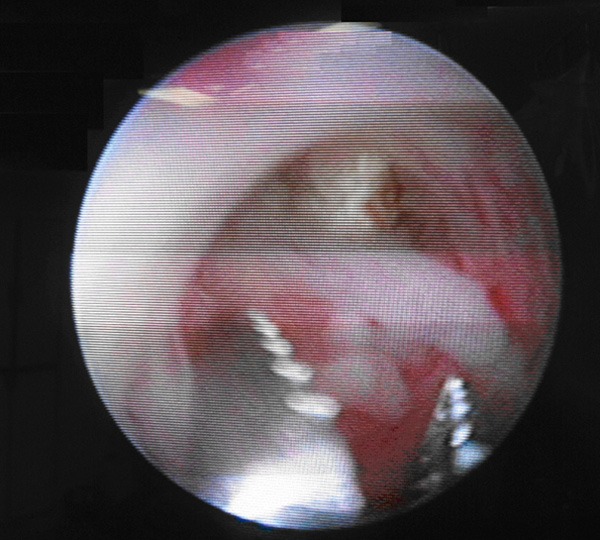
Clamping the polyps by rotation method to expose stones.
Figure 4.
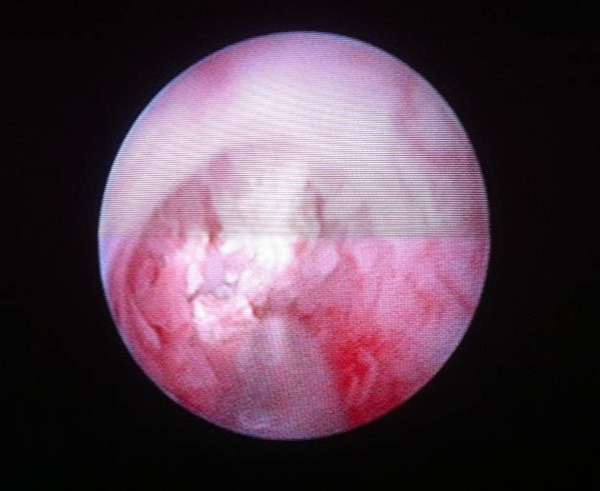
Graveling in each direction of the stone surface and evenly crushing the stones.
Follow up
All patients underwent abdominal X-ray and renal ultrasonography for hydronephrosis and residual stones on the postoperative first day. Four-six weeks after the operation, the ureteral stents were removed under the local anesthesia. To evaluate the therapeutic efficacy, US and IVU findings were used. The IVU and US findings at 3 months and 1 year after surgery were compared with those before surgery.
Statistical analysis
Data were presented as median (interquartile) for continuous variables and as frequencies (percentage) for categorical variables. Statistical analysis was performed using the t-test, χ2 test or Fisher’s exact test. Statistical analysis was done using SPSS version 15.0 (SPSS, Chicago, Illinois, USA) and a value of P<0.05 was considered statistically significant.
Results
Ureteroscopic lithotripsy was successfully performed in 86 patients with ureteral stone and FEPs who were followed up for 10.6 months (range: 6-37 months). There were 40 males and 46 females, and the median age was 35.9 years (range: 27-65 years). Moreover, 28 patients were diagnosed with upper ureter stones and 58 with middle-lower ureteral stones. The main symptoms included flank pain (38 patients) and hematuria (29 patients). The ureteral stones and FEPs were found in the left ureter of 36 patients.
The median operative time was 42 min (range: 32-63 year). There were 44 patients in cavity-distention machine-assisted group and 42 patients in traditional pneumatic lithotripsy group. All the stones were observed behind the polyps. These polyps were 1-2 cm in diameter (median: 1.5 cm). The stone size ranged from 5 mm to 13 mm (median: 8.8 mm). Fibroepithelial polyps were diagnosed in all cases by postoperative histological examination. The urine cytology showed negative. In cavity-distention machine-assisted group and traditional pneumatic lithotripsy group, the total operation time was 30.1±4.8 min and 36.2±6.0 min, respectively (t=-5.22, P<0.01); the time of stone removal was 6.4±1.3 min and 9.3±1.5 min, respectively (t=-9.59, P<0.01); the stone clearance rate was 100% (44/44) and 95.2% (40/42; ureter stone in two patients immigrated to the renal pelvis, and ESWL was performed), respectively. No major intra-operative or peri-operative complications were found except for two patients developing ureter perforation in traditional group. Blood transfusion was not performed in all these patients. The surgical information is listed in Table 1.
Table 1.
Clinical characteristics, surgical information in 2 groups
| Characteristics | Cavity-distention machine assisted group (N=44) | Traditional pneumatic lithotripsy group (N=42) | P |
|---|---|---|---|
| Gender | |||
| Male | 21 | 19 | 0.889* |
| Female | 23 | 23 | 0.899* |
| Stone size, mm | 1.44±0.41 | 1.52±0.42 | >0.05** |
| Stone location | |||
| Upper | 16 | 12 | 0.582* |
| Middle/Lower | 28 | 30 | 0.734* |
| Operative time, min | 30.1±4.8 | 36.2±6.0 | <0.01** |
| Gravel time, min | 6.4±1.3 | 9.3±1.5 | <.001** |
| Complications | |||
| Migration | 0 | 2 | |
| Perforation | 0 | 2 | |
| Unsuccessful | 0 | 2 |
All patients in two groups were followed up for 3 months to 1 year by intravenous urography (IVU) and urinary ultrasonography. No residual stones and postoperative ureteral stricture occurred in both groups. No patients displayed any symptoms and developed a new neoplasm anywhere else in the urinary tract during the study period.
Discussion
Urolithiasis with FEPs is rare and usually difficult to treat by intracorporeal lithotripsy, especially in hospitals with a small amount of endoscopic surgeries. Because the polyps of the ureter are near to the stone, bleeding, perforation and stone fragments migration may occur during the management of proximal ureteral stones, causing the operation failed. A variety of studies reveal that the success rate of therapy for urinary tract calculi with FEPs is much lower than that for simple ureter stones [5]. Although the etiology of FEPs is unclear, either congenital factors or chronic urothelial irritation (such as infection, inflammation, calculi, or obstruction) might be involved in the pathogenesis of FEPs [6]. The most common symptom of urolithiasis with FEPs is colic-like pain and hematuria. Frequent urination, dysuria, and pyuria are less common. In the pediatric age group, FEPs may present as an ureteropelvic junction obstruction. Imaging examinations usually show stones but the benign fibroepithelial polyps are often not diagnosed. The suspicious polyps may be diagnosed if radiolucent repletion defect is noted in the intravenous urography, which may or may not condition ureterohydronephrosis and change between images. CT can be used to evaluate other radiolucent filling defects of the collecting system. However, the diagnosis of polyps can be made only by the ureterorenoscopy and histological examination [6,7].
Previously, the FEP was managed by excision and reanastomosis with an open procedure. Recently, with the advent of ureteroscopes, endoscopic biopsy and resection of these tumors become popular. Most benign fibroepithelial polyps are often smoothly marginated and cylindrical, sessile or even frond-like. Additionally, it is important to differentiate the fibroepithelial polyps from the urothelial carcinoma of the urinary tract because their clinical presentations and findings in imaging examinations are similar, but their prognosis and treatments are significantly different. Endoscopic exploration of the upper urinary tract by ureterorenoscopy may offer more information in the case of a urothelial carcinoma because ureterorenoscopy not only provides a direct image of the tumor, but allows the biopsy, and the pathological examination may determine the therapeutic strategy [5,7,8].
It is difficult in intracorporeal lithotripsy for removal of urinary tract calculi with fibroepithelial polyps of the ureter, since the stones are usually covered by polyps, resulting in bleeding and blurry vision during operation [6]. Thus, ureteroscopy with hydromantic perfusion pump is frequently used in large hospitals of China. Ureteroscopy can provide continuous irrigation and control the filling pressure in surgery. However, in most areas of China, surgeons usually apply a high handled water bag with artificial water injection because of economic concern. The cavity-distention machine is widely used in the gynecological and obstetrics surgeries. We reported our experience and techniques in the management of urinary tract calculi and polyps using a cavity-distention e machine and artificial water injection during ureteroscopic lithotripsy. In present study, the operative vision was clear after irrigation with a cavity-distention machine, the working rationale of which is similar to that of hydromantic perfusion pump, and no fragment migration was observed. Results showed the time of operative duration and successful rate of lithotripsy were significantly different between two groups.
In traditional group, although high handled water bag with artificial water injection is able to keep a clear operation view, it is difficult to control the pressure of water injection. Stone fragments are easily washed back to the kidney pelvis. For the polyps parcel or covering stone, water injection fails to reveal the location of stones. The polyps should be sampled for pathological examination. To remove the covered polyps, the injection water pressure may be appropriately increased, so that the polyps got little release to move closer to the wall. Routine biopsy or special treatment is not recommended if polyps do not affect the gravel [5].
As shown in recent studies, holmium laser has some advantages in dealing with ureteral stones and polyps. The holmium laser can handle both polyps and stones, and do not need frequent replacement of equipment operation; holmium laser has hemostatic effect, and may keep the operative field clear [9]. Ureteral stones with polyps, and stones with ureteral wall adhesion are often larger in patients with ureteral stones and polyps, and the wall is thinner. Laser lithotripsy is easy to cause thermal damage to the ureteral wall, resulting in postoperative scarring and stricture [10]. In this study, stone clearance rate was 100% in cavity-distention machine group, with no intraoperative ureteral perforation, avulsion and other complications. A clear operative view is the most important to avoid ureteral injury, and cavity-distention machine can create a good view and avoid the complications of ureteral injury. Our experience was that to crush the stone in all directions by bursts at the pulse mode is able to avoid the damage to the ureteral wall and the perforation. When stones are crushed, large fragments can be pushed back to the front passes, and thus the spatial and visual field is relatively clear and the gravel may not cause damage to the wall. In addition, the surgeons should thoroughly clean the fragments adherent to the ureteral wall and polyps, because this kind of fragments is not easy to automatically discharge, and easy to cause postoperative recurrence of stones, polyps, and stricture.
When dealing with upper ureteral stones, the stones are easy to move back to the pelvis [11]. The injection speed should immediately reduce when you find stones, using the head and feet low, if necessary, available furosemide, or beside the ureteral stent to the outside resulting in top-down flow of water to avoid the stones moving back and maintain a clear view [11]. It is suggested that ureteral polyps are caused by chronic obstructive inflammation. The polyp base will shrink when the stones are removed and the obstruction or inflammatory stimuli alleviated. In addition, indwelling double J tube compression can lead to the shrinking of the polyp base. In this study, 86 patients were followed up and no ureteral stenosis was noted. Postoperative ureteral stricture was decided by polyps itself: tissue repair of ring growth, involving the ureteral wall length >1 cm polyps, and multiple polyps was likely to lead to a narrow ring, and it was not because of failing to thoroughly remove the polyps. Of note, the routine use of double J tube after surgery may prevent the postoperative ureteral mucosal edema, hemorrhage, mucosal tear and stone street formation caused by obstruction, thus avoiding renal dysfunction and secondary infection. Indwelling duration of double-J catheter should be >4 weeks, and early removal of the stent may affect the ureteral drainage and the wound repair due to local edema [12].
In summary, the intraoperative continuous perfusion of saline with cavity-distention machine instead of hydraulic perfusion pump during the lithotripsy is able to maintain a clear operation field, which is a safe, efficient micro-invasive treatment for ureteral stones and polyps and has lesser time of stone clearance during the ureteroscopic pneumatic lithotripsy. Thus, this technique has important clinical value in the treatment of ureteral calculi in the presence of polyps and is worthy of clinical application.
Acknowledgements
This work was partly supported by National Natural Science Foundation of China 81202012, Medical Scientific Research Foundation of Guangdong Province, China B2011097, Specialized Research Fund for the Doctoral Program of Higher Education of China 20110171120088 and Guangdong Science and Technology Project 2011B061200007.
References
- 1.Preminger GM, Tiselius HG, Assimos DG, Alken P, Buck AC, Gallucci M, Knoll T, Lingeman JE, Nakada SY, Pearle MS, Sarica K, Turk C, Wolf JS Jr. Guideline for the management of ureteral calculi. Eur Urol. 2007;52:1610–1631. doi: 10.1016/j.eururo.2007.09.039. [DOI] [PubMed] [Google Scholar]
- 2.Christian C, Thorsten B. The preferred treatment for upper tract stones is extracorporeal shock wave lithotripsy (ESWL) or ureteroscopic: pro ESWL. Urology. 2009;74:259–262. doi: 10.1016/j.urology.2008.08.522. [DOI] [PubMed] [Google Scholar]
- 3.Jiang H, Wu Z, Ding Q, Zhang Y. Ureteroscopic treatment of ureteral calculi with holmium: YAG laser lithotripsy. J Endourol. 2007;21:151–154. doi: 10.1089/end.2006.0209. [DOI] [PubMed] [Google Scholar]
- 4.Kara C, Resorlu B, Oguz U, Unsal A. Incidentally detected ureteral fibroepithelial polyps in children: is endoscopic treatment of them really necessary? Int Urol Nephrol. 2010;42:1–5. doi: 10.1007/s11255-009-9567-4. [DOI] [PubMed] [Google Scholar]
- 5.Mugiya S, Nagata M, Un-No T, Takayama T, Suzuki K, Fujita K. Endoscopic management of impacted ureteral stones using a small caliber ureteroscope and a laser lithotriptor. J Urol. 2000;164:329–331. [PubMed] [Google Scholar]
- 6.Turunc T, Kuzgunbay B, Canpolat T. Ureteral fibroepithelial polyps with calculi: a case series. J Med Case Rep. 2008;2:280. doi: 10.1186/1752-1947-2-280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Coloma del Peso A, Bocardo Fajardo G, Teba del Pino F, Fernandez Gonzalez I, Brime Menendez R, Fernandez Borrell A, Herrero Torres L, Pereira Sanz I. Endoscopic treatment of a giant fibroepithelial polyp of the ureter. Arch Esp Urol. 2010;63:305–308. [PubMed] [Google Scholar]
- 8.Hirata H, Eguchi K, Ohmi C, Matsuyama H, Naito K. [Transitional cell carcinoma of the ureter with inverted proliferation: a difficult case to make a differential diagnosis with ureteral polyp] . Hinyokika Kiyo. 2003;49:619–621. [PubMed] [Google Scholar]
- 9.Carey RI, Bird VG. Endoscopic management of 10 separate fibroepithelial polyps arising in a single ureter. Urology. 2006;67:413–415. doi: 10.1016/j.urology.2005.08.020. [DOI] [PubMed] [Google Scholar]
- 10.Nuttall MC, Abbaraju J, Dickinson IK, Sriprasad S. A review of studies reporting on complications of upper urinary tract stone ablation using the holmium: YAG laser. Br J Med Surg Urol. 2010;3:151–159. [Google Scholar]
- 11.Zhang J, Shi Q, Wang GZ, Wang F, Jiang N. Cost-effectiveness analysis of ureteroscopic laser lithotripsy and shock wave lithotripsy in the management of ureteral calculi in eastern China. Urol Int. 2011;86:470–475. doi: 10.1159/000324479. [DOI] [PubMed] [Google Scholar]
- 12.Wang CJ, Huang SW, Chang CH. Indications of stented uncomplicated ureteroscopic lithotripsy: a prospective randomized controlled study. Urol Res. 2009;37:83–88. doi: 10.1007/s00240-009-0175-7. [DOI] [PubMed] [Google Scholar]