

Abstract
A large proportion of gastric cardia adenocarcinoma (GCA) present initially in an advanced stage in China. Skin metastasis of primary GCA rarely occurs and the incidence of it is still unclear yet. Here we report one case of skin metastasis from GCA in a 58-year-old male patient who underwent gastric cardia resection in 2002 and did not undergo chemotherapy. However, he was diagnosed with anastomotic stoma adenocarcinoma by gastroscopy and histological biopsy in 2012.4. Then he underwent four cycles of “XELOX” regimen chemotherapy and the evaluation was PR. Upper gastrointestinal bleeding occurred and he was administered hemostatic therapy in 2012.9; meanwhile, he suffered from severe pains all over the body and received slow-release morphine. However, he was found to have dozens of cutaneous metastasizes in the skin of abdominal and back. Then, he underwent best supportive care and died of cachexia in 2013.5. GCA cutaneous metastasis indicates a highly invasive potential of tumors, poor chemo-radiotherapy efficacy and poor prognosis. The patient may survive just for another several months without the treatment of anti-tumor agents. Appropriate treatment may prolong patient survival.
Keywords: Gastric cardia adenocarcinoma, cutaneous metastasis
Introduction
Skin metastases of malignant tumor occur in about 0.5 to 10% of patients with tumors, and usually, they were the first sign of extranodal metastatic disease [1-8]. Among skin metastases, breast cancer [9,10] and melanoma [11-13] were the most common; histologic findings most frequently revealed adenocarcinoma that was sometimes suggestive of the site of origin [3]. After recognition of skin metastases, the lifetime of patients ranged from 1 to 34 months depending on tumor type [14,15]. Here, we reported a patient who developed skin metastases from the gastric cardia adenocarcinoma 10 years after his initial diagnosis.
Case presentation
A 58-year-old man, who suffered from difficulty swallowing in 2002, and was diagnosed with I stage gastric cardia adenocarcinoma according to the gastroscope examination and histological biopsy. Then he underwent gastric cardia resection and no further anti-tumor agents were administered. However, he felt difficulty swallowing again 10 years after his initial diagnosis and surgery. Gastroscopy showed that there was a 1×1.5 cm mass on the anastomotic stoma wall which was infiltrating type. Computed tomography (CT) scan was also performed and confirmed the presence of a anastomotic stoma mass with adjacent lymph node swelling (Figure 3). However, blood tumor markers examination did not show significant abnormality. Then he underwent six cycles of “XELOX” regimen chemotherapy from 2012.4-2012.9. Upper gastrointestinal bleeding occurred after the 6th cycle chemotherapy had ended 10-11 days, and he was administered hemostatic therapy. Meanwhile, he began to suffer from severe pains all over the body and received slow-release morphine for symptomatic treatment. Moreover, he was found to have dozens of cutaneous metastasizes in the skin of abdominal (Figures 1 and 2) and back. The histological biopsy verified the abdominal skin nodule is poorly differentiated adenocarcinoma origin. Then, this patients refused anti-tumor therapy and more equipment inspection, he just underwent best supportive care and died of cachexia in 2013.5.
Figure 3.
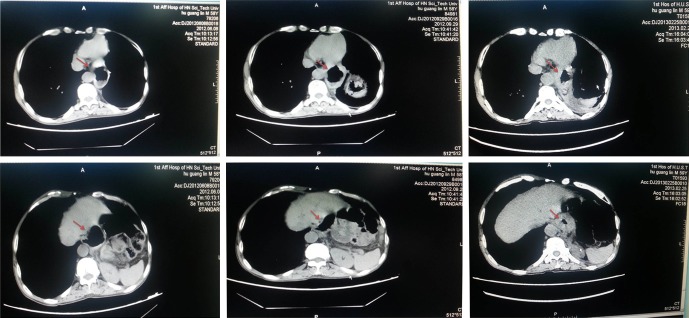
Computed tomography (CT) scan. The presence of a anastomotic stoma mass with adjacent lymph node swelling was showed in 09/2012 and enlarged in 02/2013 (red arrow).
Figure 1.

Abdominal cutaneous metastasis nodule. This nodule is located in the right abdominal wall.
Figure 2.
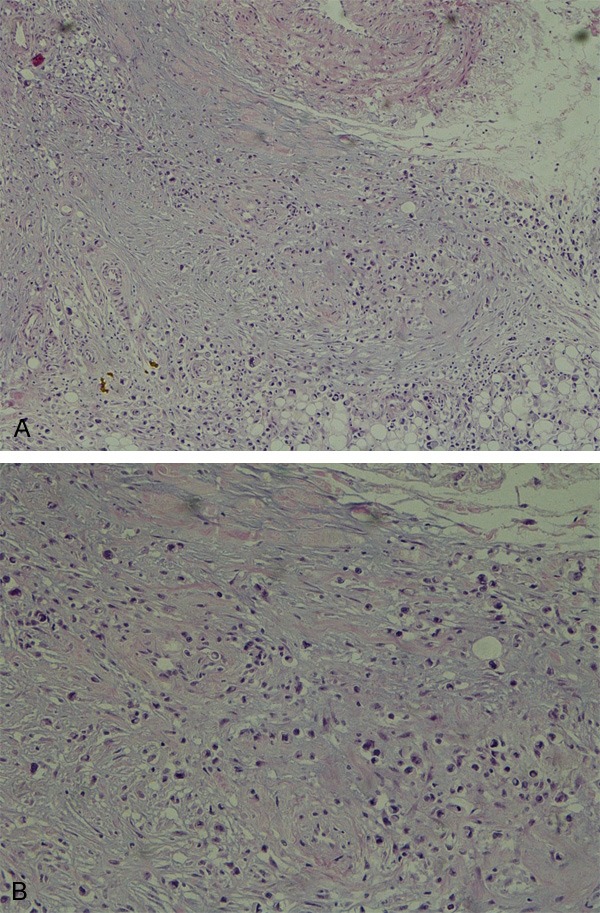
HE staining of abdominal cutaneous metastasis nodule. The pathological diagnosis of this metastasis nodule is poorly differentiated adenocarcinoma (magnitude: A: 100×, B: 200×).
This patient is a heavy smoker, he also had sever emphysema. Besides, he also suffered from multiple hepatic peribiliary cysts, left renal cysts and hydronephrosis.
Discussion
Skin metastasis from visceral carcinoma rarely occurs, and to date, few cases have been reported. According to the literature, skin metastases incidence of malignant tumor is about 0.5 to 10%, and usually, they were the first sign of extranodal metastatic disease. Among skin metastases, breast cancer and melanoma were the most common. Metastases from carcinomas of the upper digestive tract have an incidence less than 1% [3]. Umberto Morelli et al reported a patient who developed a skin metastasis from a gastric adenocarcinoma in the location of a previous surgical drain [16]. A 64-year-old male patient suffered from small-cell lung cancer metastasizing to his face at the time of initial diagnosis [2]; a 65-year-old male with a cutaneous metastasis in the root of his inferior left extremity one year after right nephrectomy for a clear cell adenocarcinoma [17]. Besides, gallbladder adenocarcinoma [18,19], sarcomatoid carcinoma of the bladder [3], colorectal cancer [15,19] et al. have also been reported to metastasize to the skin once. However, skin metastasis from gastric cardia adenocarcinoma has not been reported before.
In this report, we describe a patient who developed a skin metastasis from a gastric cardia adenocarcinoma 10 years after his initial diagnosis and surgery. However, CT and whole-body nuclear medicine bone scanning (ECT) showed no cancer metastasis to other parts of the body. It is doubtful that whether there were dormant cancer cells under skin and they were activated later. A subcutaneous nodule can be palpable when it grows to 0.5~1.0 cm size and they could be neglected unless the number of nodules is relatively high or the size of them is big enough. Hence, performing 3D positron emission tomography (PET)/CT might be a effective method to detect minor skin metastasis loci in order to administer appropriate treatment to the patients and to prolong their survival time.
Another arresting phenomenon of this case is that metastasis nodules occurred in the skin of abdomen and back, and not in limbs, buttocks, neck and face. Is it because that arterial blood pressure is higher in proximal arteries than in distal ones? So cancer cells could transverse vascular endothelial cell easier in abdominal and back skin than in limbs? Dose it mean that cancer cells that develop cutaneous metastasis possess higher metastatic potential? The answer could be no. Because no metastases nodules were found in other parts of body of this patient, hence, it is plausible that patients with tumors who had skin metastasis might had tumor subgroups because of tumor heterogeneity that tend to develop colonies in skin. Moreover, once the cutaneous metastases were developed, the patients may survive for about 1 to 34 months depending on tumor type [3]. Would anti-tumor agents work well to prolong the survival time of patients? This question needs to be further studied in the future.
Conclusion
In this report, we have described a 58-year-old male patient with gastric cardia adenocarcinoma had cutaneous metastases 10 years after his initial diagnosis and surgery, indicating that though skin metastasis of the upper digestive tract is relatively low, it really occurs. This patient survived for only four months after skin metastases were palpable under the best supportive care. It is imperative to pay close intention to the patients’ skin inspection during the periodical checkup and histological biopsy is necessary once subcutaneous nodules occurred.
Acknowledgements
Supported by National Natural Science Foundation of China, No. 81301763, 30670956, and National Outstanding Young Scientist Award of China, No. 30025016.
Disclosure of conflict of interest
All authors have nothing to disclose.
Abbreviations
- GCA
Gastric cardia adenocarcinoma
- CT
Computed tomography
References
- 1.Tanriverdi O, Meydan N, Barutca S, Kadikoylu G, Sargin G, Tataroglu C, Culhaci N. Cutaneous Metastasis of Gallbladder Adenocarcinoma in a Patient with Chronic Lymphocytic Leukemia: A Case Report and Review of the Literature. Ann Dermatol. 2013;25:99–103. doi: 10.5021/ad.2013.25.1.99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Barbetakis N, Samanidis G, Paliouras D, Samanidou E, Tzimorota Z, Asteriou C, Xirou P, Tsilikas C. Facial skin metastasis due to small-cell lung cancer: a case report. J Med Case Rep. 2009;3:32. doi: 10.1186/1752-1947-3-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lookingbill DP, Spangler N, Helm KF. Cutaneous metastases in patients with metastatic carcinoma: a retrospective study of 4020 patients. J Am Acad Dermatol. 1993;29:228–236. doi: 10.1016/0190-9622(93)70173-q. [DOI] [PubMed] [Google Scholar]
- 4.Brownstein MH, Helwig EB. Patterns of cutaneous metastasis. Arch Dermatol. 1972;105:862–868. [PubMed] [Google Scholar]
- 5.Brownstein MH, Helwig EB. Metastatic tumors of the skin. Cancer. 1972;29:1298–1307. doi: 10.1002/1097-0142(197205)29:5<1298::aid-cncr2820290526>3.0.co;2-6. [DOI] [PubMed] [Google Scholar]
- 6.Saeed S, Keehn CA, Morgan MB. Cutaneous metastasis: a clinical, pathological, and immunohistochemical appraisal. J Cutan Pathol. 2004;31:419–430. doi: 10.1111/j.0303-6987.2004.00207.x. [DOI] [PubMed] [Google Scholar]
- 7.Di Palma S, Fehr A, Danford M, Smith C, Stenman G. Primary sinonasal adenoid cystic carcinoma presenting with skin metastases–genomic profile and expression of the MYB-NFIB fusion biomarker. Histopathology. 2014;64:453–455. doi: 10.1111/his.12261. [DOI] [PubMed] [Google Scholar]
- 8.Lookingbill DP, Spangler N, Sexton FM. Skin involvement as the presenting sign of internal carcinoma: a retrospective study of 7316 cancer patients. J Am Acad Dermatol. 1990;22:19–26. doi: 10.1016/0190-9622(90)70002-y. [DOI] [PubMed] [Google Scholar]
- 9.Moore S. Cutaneous metastatic breast cancer. Clinical Journal of Oncology Nursing. 2002;6:255–260. doi: 10.1188/02.CJON.255-260. [DOI] [PubMed] [Google Scholar]
- 10.Brooks PC, Strömblad S, Klemke R, Visscher D, Sarkar FH, Cheresh DA. Antiintegrin alpha v beta 3 blocks human breast cancer growth and angiogenesis in human skin. J Clin Invest. 1995;96:1815. doi: 10.1172/JCI118227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bittner M, Meltzer P, Chen Y, Jiang Y, Seftor E, Hendrix M, Radmacher M, Simon R, Yakhini Z, Ben-Dor A. Molecular classification of cutaneous malignant melanoma by gene expression profiling. Nature. 2000;406:536–540. doi: 10.1038/35020115. [DOI] [PubMed] [Google Scholar]
- 12.Massi G, Leboit PE. Histological Diagnosis of Nevi and Melanoma. Springer; 2004. Cutaneous Metastatic Melanoma; pp. 631–644. [Google Scholar]
- 13.Thurner B, Haendle I, Röder C, Dieckmann D, Keikavoussi P, Jonuleit H, Bender A, Maczek C, Schreiner D, von den Driesch P. Vaccination with mage-3A1 peptide-pulsed mature, monocyte-derived dendritic cells expands specific cytotoxic T cells and induces regression of some metastases in advanced stage IV melanoma. J Exp Med. 1999;190:1669–1678. doi: 10.1084/jem.190.11.1669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Manzelli A, Quaresima S, Rossi P, Petrou A, Ricciardi E, Brennan N, Kontos M, Petrella G. Solitary skin metastasis from sarcomatoid carcinoma of the bladder: a case report. J Med Case Rep. 2011;5:1–4. doi: 10.1186/1752-1947-5-484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Saladzinskas Z, Tamelis A, Paskauskas S, Pranys D, Pavalkis D. Facial skin metastasis of colorectal cancer: a case report. Cases J. 2010;3:28. doi: 10.1186/1757-1626-3-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Morelli U, Cirocchi R, Mecarelli V, Farinella E, La Mura F, Ronca P, Giustozzi G, Sciannameo F. Gastric adenocarcinoma cutaneous metastasis arising at a previous surgical drain site: a case report. J Med Case Rep. 2009;3:65. doi: 10.1186/1752-1947-3-65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Barbagelata López A, Ruibal Moldes M, Blanco Díez A, Fernández Rosado E, Ponce Díaz-Reixa JL, Novas Castro S, Lancina Martín A, González Martín M. Metastasis cutánea del cáncer renal: caso clínico y revisión. Archivos Españoles de Urología (Ed. impresa) 2005;58:247–250. doi: 10.4321/s0004-06142005000300011. [DOI] [PubMed] [Google Scholar]
- 18.Drouard F, Delamarre J, Capron JP. Cutaneous seeding of gallbladder cancer after laparoscopic cholecystectomy. N Engl J Med. 1991;325:1316. doi: 10.1056/NEJM199110313251816. [DOI] [PubMed] [Google Scholar]
- 19.Krunic AL, Chen HM, Lopatka K. Signet-ring cell carcinoma of the gallbladder with skin metastases. Australas J Dermatol. 2007;48:187–189. doi: 10.1111/j.1440-0960.2007.00379.x. [DOI] [PubMed] [Google Scholar]