

Abstract
OBJECTIVE
To examine urinary levels of enterolactone and enterodiol, intestinal microbial metabolites of dietary lignans, in relation to type 2 diabetes (T2D) risk.
RESEARCH DESIGN AND METHODS
Urinary concentrations of the lignan metabolites were assayed by liquid chromatography-mass spectrometry among 1,107 T2D and 1,107 control subjects in a nested case-control study conducted in participants from the Nurses’ Health Study (NHS) and NHSII. Subjects were free of diabetes, cardiovascular disease, and cancer at urine sample collection in 1995–2001. Incident self-reported T2D cases identified through 2008 were confirmed with a validated questionnaire.
RESULTS
In both cohorts, T2D subjects had significantly lower concentrations of both enterolactone and enterodiol than control subjects. After multivariate adjustment for lifestyle and dietary risk factors of T2D, urinary concentrations of enterolactone were significantly associated with a lower risk of T2D (pooled odds ratio [OR] comparing the extreme quartiles 0.62 [95% CI 0.44, 0.88], P for trend = 0.003). Higher urinary concentrations of enterodiol were also marginally significantly associated with a lower T2D risk (pooled OR comparing extreme quartiles 0.67 [95% CI 0.48, 0.96], P for trend = 0.08). When concentrations of both metabolites were combined to reflect total lignan intake, the OR was 0.70 (95% CI 0.53, 0.92) for each SD increment of total lignan metabolites.
CONCLUSIONS
These results indicate that lignan metabolites, especially enterolactone, are associated with a lower risk of T2D in U.S. women. Further studies are needed to replicate these findings and to explore potential mechanisms underlying the observed association.
Introduction
Lignans are a group of plant-synthesized chemicals that are constituents of plant cell walls (1). A few of these naturally occurring compounds, primarily lariciresinol, pinoresinol, secoisolariciresinol, and matairesinol, ubiquitously exist in plant foods in the human diet (2,3). Fiber-rich foods, including whole grains, seeds, and legumes, as well as some beverages, such as coffee and wine, contain measurable amounts of lignans, and flaxseeds are a particularly rich source (1). Humans have a long history of using certain lignans for medicinal purposes (4), but evidence regarding the biological effects of lignans on human health has started to accumulate only recently.
Both animal and human experiments have demonstrated potentially beneficial effects of lignans on human health (2,3,5,6), although thus far, long-term human epidemiological studies that exclusively focused on the association of lignan intake with the risk of cancers and cardiovascular disease have generated somewhat equivocal results (3,7). Lack of complete food composition databases of lignans may primarily explain the inconsistent findings (2). Moreover, dietary lignans undergo substantial metabolism by intestinal microbiota to produce more biologically active lignan metabolites (2). Likely because of these methodological challenges, observational studies examining lignan intake and type 2 diabetes (T2D) risk are largely lacking. In the current investigation, therefore, we used data from two well-characterized cohorts of U.S. women, the Nurses’ Health Study (NHS) and NHSII, to prospectively evaluate the hypothesis that urinary concentrations of enterolactone and enterodiol, major metabolites of dietary lignans, are associated with a lower T2D risk.
Research Design and Methods
Study Population
In 1976, 121,700 female registered nurses aged 30–55 years living in one of 11 U.S. states responded to a study questionnaire and established the NHS cohort. In 1989, a younger counterpart of the NHS was initiated using the same enrollment approach, and 116,686 female registered nurses aged 25–42 years were included in the NHSII. In these two cohorts, similar data collection methods and participant follow-up strategies are used. In both cohorts, follow-up questionnaires inquiring about a wide array of variables, including body weight and height, demographics, lifestyle practices, history of chronic diseases, and medication use, are administered biennially to update information assessed at baseline and to collect new data.
Urine Sample Collection
A total of 29,611 NHSII participants aged 32–52 years provided blood and urine samples in 1995–2000, and 18,717 NHS participants aged 53–79 years provided samples in 2000–2001. In both cohorts, the samples were sent to a central biorepository by overnight courier, immediately processed on arrival, and aliquoted into cryotubes, which were stored in the vapor phase of liquid nitrogen freezers at ≤−130°C. Among participants who provided blood and urine samples, a high follow-up rate of >90% has been maintained.
Prospective Case-Control Study Design
In both cohorts, we conducted a prospective, nested case-control study of T2D among participants who provided urine samples and were free of self-reported diabetes, cardiovascular disease, and cancer at sample collection. During follow-up through 2008 (NHS) or 2007 (NHSII), we prospectively identified and confirmed 1,107 T2D case subjects (NHS: n = 452; NHSII: n = 655) and randomly selected one control subject for each case subject. Case and control subjects were matched for age at urine sample collection, month of sample collection, fasting status (≥8 h or not), first morning urine (yes, no), race (white or other races), menopausal status, and hormone replacement therapy (NHSII only). To minimize reverse causation bias, we excluded diabetes cases diagnosed within the first year since urine sample collection. The study protocol was approved by the institutional review board of the Brigham and Women’s Hospital and the Human Subjects Committee Review Board of the Harvard School of Public Health.
Ascertainment of T2D
We sent a validated supplemental questionnaire to subjects who reported a physician diagnosis of T2D to confirm new-onset disease. We used at least one of the following American Diabetes Association 1998 criteria to confirm self-reported T2D diagnosis: 1) an elevated glucose concentration (fasting plasma glucose ≥7.0 mmol/L, random plasma glucose ≥11.1 mmol/L, or plasma glucose ≥11.1 mmol/L after an oral glucose load) and at least one symptom related to diabetes; 2) no symptoms, but elevated glucose concentrations on two separate occasions; or 3) treatment with insulin or oral hypoglycemic medication. Only confirmed T2D cases were included in the current study.
Assessment of Diet
Validated food frequency questionnaires (FFQs) were administered in 1984 and 1986 in the NHS and in 1991 in the NHSII. Similar FFQs were subsequently sent to participants quadrennially to update diet. In these FFQs, we inquired about the average consumption frequency of 118–166 food items in the past year with a prespecified serving size for each item. Reasonable validity and reproducibility of the assessments of food sources of lignans, including whole grains, wine, coffee, fruits, and vegetables, have been demonstrated in validation studies (8). Of note, consumption of flaxseeds was not assessed by the FFQs.
Laboratory Measurements
In the current study, we used electrospray ionization orbitrap liquid chromatography-mass spectrometry (9) to measure enterodiol and enterolactone in urine samples (Supplementary Data). Urinary creatinine levels were measured with a Roche-Cobas MiraPlus clinical chemistry autoanalyzer (Roche Diagnostics). The average intra-assay coefficient of variation was 15.3% for enterodiol, 7.9% for enterolactone, and 5.6% for creatinine. We calculated creatinine-adjusted concentrations (nmol/g creatinine) of lignan metabolites by dividing the metabolite levels (nmol/L) by creatinine levels (g/L). In a pilot study that evaluated within-person stability of the metabolites, intraclass correlation coefficients (ICCs) between levels in two urine samples collected 1–2 years apart from 58 NHSII participants were 0.45 for enterodiol and 0.53 for enterolactone.
Statistical Methods
We used linear regression to identify significant food predictors of log-transformed concentrations of enterodiol and enterolactone following the stepwise selection algorithm with multivariate adjustment for age at sample collection, fasting status, smoking status, BMI, physical activity, total calorie intake, and cohort (NHS or NHSII). We then calculated Spearman partial correlation coefficients (rs) between the metabolites and their significant food predictors to evaluate the strength of association. These analyses were conducted among control subjects to improve generalizability to the whole cohorts.
We categorized the study population into quartiles according to the distribution of enterolignan levels among control subjects. We used conditional logistic regression to model the associations of interest. To control for confounding, we adjusted for matching factors, BMI, smoking status, physical activity, alcohol use, oral contraceptive use (NHSII only), hormone replacement therapy (NHS only), family history of diabetes, history of hypercholesterolemia or hypertension, and the alternate Healthy Eating Index (AHEI) score (10). P values for linear trend were calculated by entering an ordinal score based on the median value in each quartile of enterolignan levels into the multivariate models. Odds ratios (ORs) from the two cohorts were pooled using a fixed-effects model. Heterogeneity of ORs between the two cohorts was evaluated by the Cochrane Q statistic (P < 0.05 was considered indicative of statistically significant heterogeneity) and the I2 statistic.
We used restricted cubic spline regressions with 3 knots to model a potential dose-response relationship. In this analysis, we excluded participants with the highest 5% of lignan levels to minimize the potential impact of outliers. Tests for nonlinearity were based on the likelihood ratio test, comparing the model with only the linear term to the model with the linear and the cubic spline terms, and corresponding P values of linearity and curvature were derived. To maximize statistical power, we pooled individual-level data from the two cohorts in this dose-response analysis while maintaining the matched case-control pairs by using conditional logistic regression. In secondary analyses, we also used a method developed by Rosner et al. (11) to correct for random within-person variability of lignan metabolites, which was measured by the ICC in the pilot study.
All P values were two-sided. Data were analyzed with SAS version 9.3 statistical software (SAS Institute Inc., Cary, NC).
Results
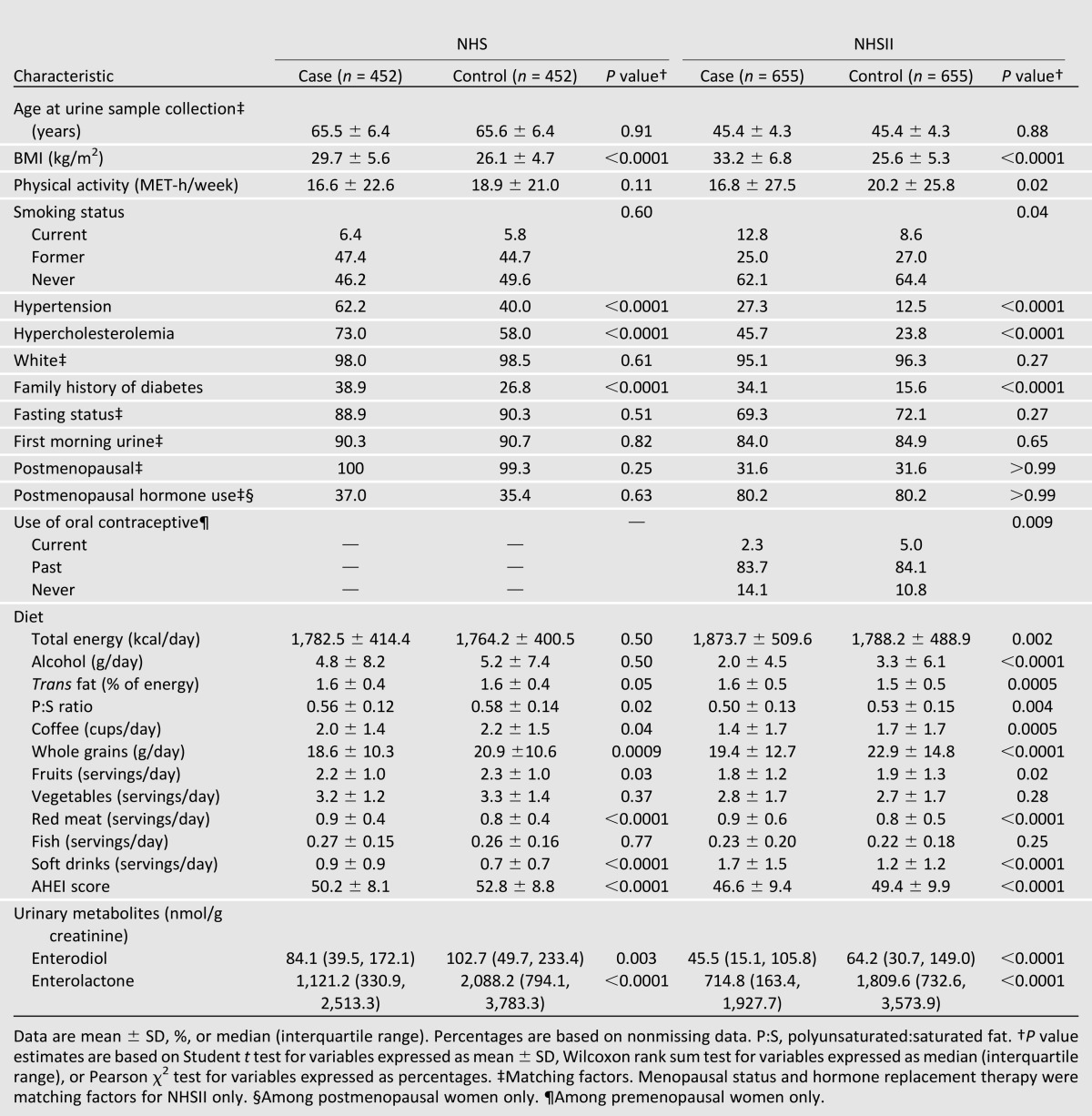
Characteristics of study participants assessed using baseline questionnaires (NHS, 1998; NHSII, 1995) are shown in Table 1. As expected, diabetic subjects had a high-risk profile in both cohorts except for the matching factors. They were heavier, were more likely to have a history of hypertension and high blood cholesterol and a family history of diabetes, ate a less healthful diet, and engaged in less physical activity than control subjects. In both cohorts, case subjects had lower urinary levels of both lignan metabolites than control subjects, with an approximately twofold difference for enterolactone levels. A notable difference between the two cohorts was the older age at sample collection in the NHS than in the NHSII.
Table 1.
Baseline characteristics of diabetic case subjects and control subjects in the NHS and NHSII
Intake of various foods was modestly but significantly correlated with enterolignan concentrations among control subjects (Supplementary Table 1). The highest multivariate-adjusted Spearman correlations between food intake and enterolactone concentrations were observed for whole grains (rs = 0.14), apples (rs = 0.14), coffee (rs = 0.13), romaine or leaf lettuce (rs = 0.13), raw spinach (rs = 0.12), and red wine (rs = 0.11). Correlations between food predictors and enterodiol concentrations were generally weaker. We also examined the correlation between enterodiol and enterolactone in control subjects and found moderate correlations in both the NHS (rs = 0.53) and the NHSII (rs = 0.45).
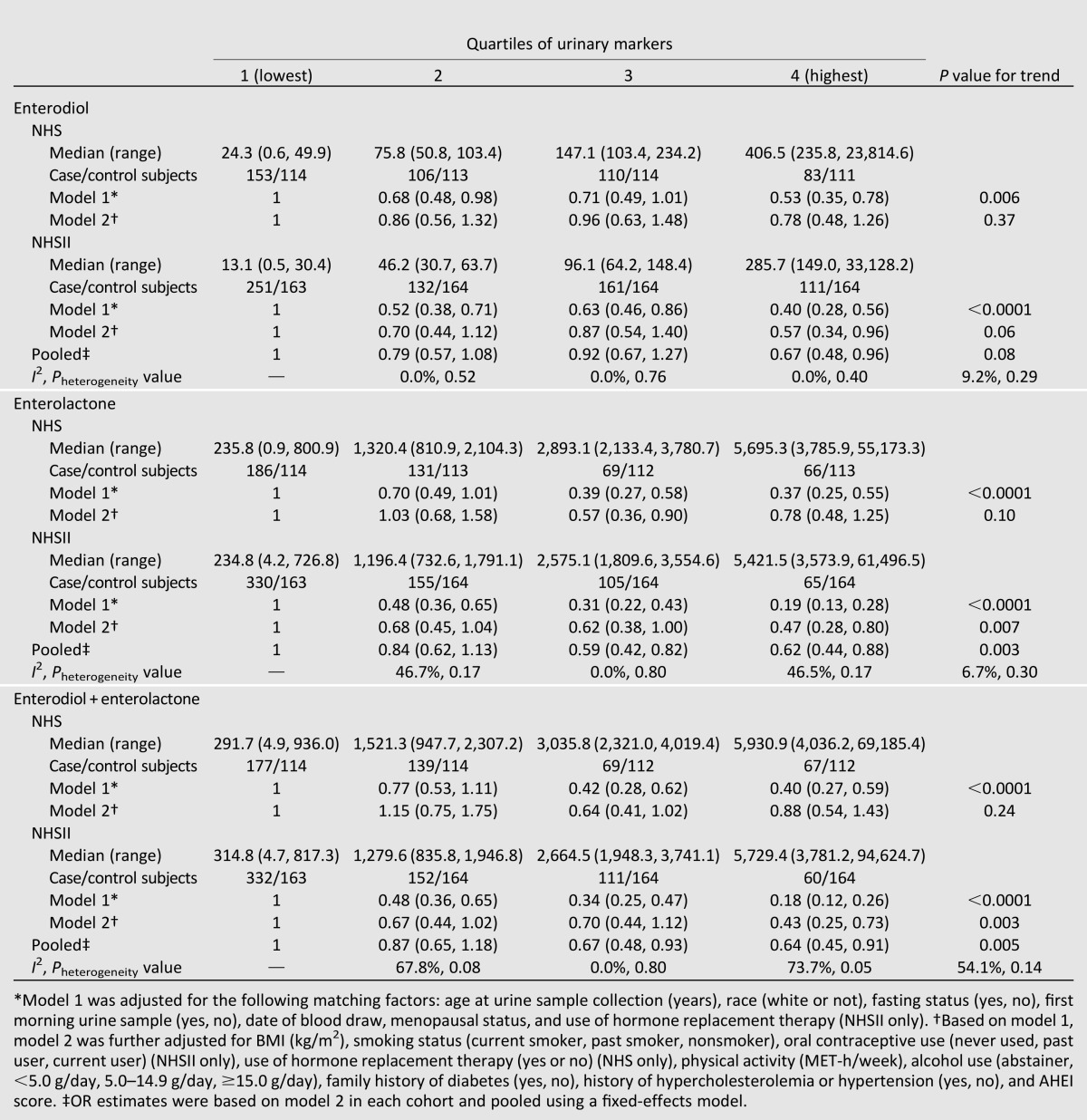
Table 2 presents associations between enterolignan levels and diabetes risk in the two cohorts. In the crude model adjusted for matching factors only, concentrations of both enterolactone and enterodiol were associated with a lower T2D risk in the two cohorts. In the NHS, further adjustment for diabetes risk factors, especially BMI, attenuated the significant associations for the lignan metabolites. In the NHSII, associations for the metabolites were attenuated as well, but the associations for the highest quartiles of both metabolites remained statistically significant. The distribution of covariates by levels of enterolignans is presented in Supplementary Table 1. In both cohorts, higher enterolignan levels were associated with a lower BMI, consistent with the observation that BMI was the strongest confounder for the studied associations. Pooled associations of the enterolignans from the two studies showed a significant inverse association for enterolactone (pooled OR [95% CI] 0.62 [0.44, 0.88], P for trend = 0.003), comparing extreme quartiles. A significant inverse association was observed for the highest enterodiol quartile only (pooled OR [95% CI] 0.67 [0.48, 0.96], P for trend = 0.08). We did not observe significant heterogeneity among these associations between the two cohorts (P for heterogeneity = 0.40 and 0.17, for highest quartiles of enterodiol and enterolactone levels, respectively). Associations for combined levels of enterodiol and enterolactone were similar to those for enterolactone. A sensitivity analysis using a random-effects model to pool the results showed a similar pattern of associations: comparing extreme quartiles, the pooled ORs (95% CIs) were 0.61 (0.38, 0.996; P for trend = 0.004) for enterolactone and 0.67 (0.48, 0.96; P for trend = 0.09) for enterodiol levels.
Table 2.
OR (95% CI) of T2D by quartiles of lignan metabolites (nmol/g creatinine) in the NHS and NHSII
We subsequently explored whether a dose-response relation existed for the association between enterolactone and diabetes risk. We detected a significant linear trend for the association between enterolactone levels and diabetes risk (P for linearity = 0.007 and P for curvature = 0.49) (Fig. 1). A nonsignificant inverse trend was found for enterodiol. Combined levels of enterodiol and enterolactone also showed a similar significant linear trend (P for linearity = 0.009 and P for curvature = 0.64). Furthermore, we estimated that for each SD increment of log-transformed total enterolignan levels, the OR was 0.85 (95% CI 0.74, 0.96). After correction for random errors in the assessment of total enterolignans (stability ICC = 0.54), this OR was 0.70 (0.53, 0.92).
Figure 1.
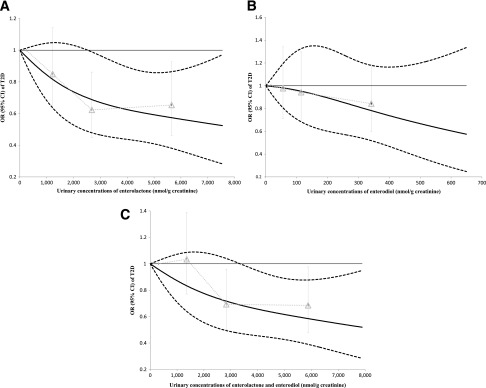
Dose-response relationship between lignan metabolites and risk of T2D based on combined data from the NHS and NHSII. Study participants with the highest 5% of metabolite levels were excluded to minimize the potential impact of outliers. Multivariate conditional logistic regression models were adjusted for the same set of covariates for model 2 in Table 2. A: Enterolactone. B: Enterodiol. C: Enterolactone and enterodiol. Solid lines are ORs and dashed lines are 95% CIs. Gray triangles represent the OR for quartiles of biomarkers based on pooled data from the NHS and NHSII.
We examined joint associations between the lignan metabolites and AHEI score to further evaluate whether the lower diabetes risk associated with higher enterolignan concentrations was due to better diet quality. In general, within each tertile of the AHEI score, enterolactone remained associated with a lower diabetes risk. The P value for interaction was 0.62 (Fig. 2). We further examined the same joint associations between enterolactone and BMI (Supplementary Fig. 1). In general, within obese and overweight groups, participants with the higher enterolactone concentrations had a lower diabetes risk, and this association was less clear among lean participants, although we did not find a signification interaction by BMI (P for interaction = 0.39).
Figure 2.

Joint associations between enterolactone and AHEI score. Multivariate conditional logistic regression models were adjusted for the same set of covariates for model 2 in Table 2.
Conclusions
In this prospective investigation among two cohorts of U.S. women, we found that urinary levels of enterolactone, a lignan metabolite produced by intestinal microbiota, are associated with lower T2D risk in a dose-dependent fashion. These associations are independent of demographic and lifestyle risk factors of T2D and of overall diet quality.
Our knowledge of food composition and metabolism of lignans has evolved rapidly, especially in the past decade. Early investigations regarding food composition of lignans only measured secoisolariciresinol and matairesinol, which are found in particularly high concentrations in flaxseed (12). More recent work has quantified several other dietary lignans, including lariciresinol and pinoresinol, which are the major lignans in foods and beverages other than flaxseed (2,13). Thus far, a comprehensive food composition database of lignans is lacking, resulting in significant difficulties for using traditional instruments to accurately quantify lignan intake. More importantly, all plant lignans undergo substantial metabolism by intestinal microbiota to produce enterolignans (14), which either are excreted in the feces or enter the circulation, although the conversion rate to enterolignans varies among plant lignans (3). Studies have shown that at the population level, a clear time-integrated dose-response relationship exists between lignan consumption levels and concentrations of enterolignans in plasma or urine (15,16). Meanwhile, these investigations also demonstrated wide interindividual variability in their metabolism (15,16), predominantly because of variation in gut microbiota composition. In terms of biological effects, enterolignans are believed to be more potent than their parent molecules (2). Thus, using urinary metabolites of plant lignans to examine associations of lignan intake with disease risk is a unique strength in that the urinary concentrations of enterolignans are more likely to reflect tissue exposure to bioavailable lignans (17).
To our knowledge, the current study is the first to prospectively examined urinary concentrations of enterolignans in relation to T2D risk. The observations are largely consistent with several short-term human trials that examined flaxseeds or flaxseed-derived lignans in relation to metabolic risk factors. For example, beneficial effects of flaxseed supplements on glucose homeostasis as measured by oral glucose tolerance test or fasting glucose levels were documented in healthy young (18) and postmenopausal (19) women. Trials conducted among participants with glucose intolerance generated somewhat mixed results. In a 12-week feeding trial among Chinese diabetic patients, Pan et al. (20) observed beneficial effects of flaxseed-derived lignan supplements on HbA1c and C-reactive protein levels but not on insulin resistance. In a smaller trial among obese participants with glucose intolerance, flaxseed supplements significantly improved insulin resistance (21). In contrast, in older Canadians who participated in a long-term walking program, no effects of lignan supplements on blood glucose levels were observed (22) possibly because of the elevated physical activity levels in these participants. Another line of evidence in support of the potential effects on diabetes risk comes from investigations that evaluated some other food sources of lignans in relation to diabetes risk. For example, higher consumption of whole grains, fruits, coffee, and red wine have been associated with a lower risk of T2D in observational studies (23–27), although the extent to which lignans account for the beneficial effects of these foods is unclear.
Mechanisms underlying the putative beneficial effects of lignans are still poorly understood. Antioxidation of lignans through scavenging free radicals is the most elucidated mechanism in in vitro studies, although such effects have not been substantiated in vivo (28). Meanwhile, the close relationship between lignans and sex hormone metabolism has drawn much attention. Enterolignans, especially enterolactone, preferably bind to estrogen receptor (ER)-α over ERβ and lead to subsequent ER-mediated gene transcription in vitro (29). In vivo experiments corroborate the estrogenic effects of enterolignans through preferably activating ERα in female mice, although the strength of the estrogenic effects varies in these studies (29–31). Accumulating evidence suggests that ERα plays a pivotal role in maintaining normal body weight and insulin sensitivity, whereas ERβ seems to have the opposite effect (32,33). Of note, lignans may also exert antiestrogenic effects through increasing the level of sex hormone–binding proteins (34,35), which are strongly associated with a lower risk of developing T2D in men and women (36). These pathways may explain the inverse associations observed in the current investigation as well as the effects of lignan intake on delaying onset of diabetes, attenuating diet-induced fat accumulation, and promoting adiponectin expression in rodent models (37,38). However, the current results do not directly support the benefits of increased lignan intake or supplementation because other factors affecting production of enterolignans by gut microbiota composition may have contributed to the observed associations. In addition, other products of enterolactone-producing gut bacteria may have confounded the results. Thus, further research is warranted to identify the bacterial species that are responsible for lignan metabolism and to elucidate their physiological effects.
There are several caveats in the current study that merit discussion. First, the half-lives of enterolignans are short (4.4 h for enterodiol) to modest (12.6 h for enterolactone) (15), suggesting that a single measurement of these biomarkers is more likely to reflect relatively short-term levels. Meanwhile, the urinary lignan concentrations were reasonably strongly correlated over 1–2 years as observed in the pilot study, probably owing to a stable diet and intestinal microbiota over time. Nonetheless, use of multiple assessments of the lignan metabolites over time would be a more desirable approach to better reflect usual exposure levels. Second, compared with 24-h urine samples, spot urine samples may not be optimal to assess lignan levels accurately, although the spot urine is much more accessible, allowing collection in large epidemiological studies. Third, we did not measure enterofuran, a minor enterolignan, in the current study and, therefore, could not evaluate this specific marker in relation to diabetes risk. Fourth, although we controlled for a wide range of established diabetes risk factors, including dietary factors, the possibility of residual confounding still exists. Finally, because the lignan metabolites may be derived from multiple parent plant lignans that come from various food sources, we are unable to conclusively ascribe the associations to intake of individual plant lignans or foods.
In summary, this prospective investigation conducted in two cohorts of U.S. women demonstrates that urinary levels of enterolignans are associated with a lower risk of developing T2D. These novel findings complement the current knowledge on the effects of lignan intake on glucose metabolism and other metabolic risk factors in short-term trials. In light of the accumulating evidence suggesting that gut microbiota composition may play a role in the development of obesity and T2D (39), the current data suggest that the enterolignan production by gut microbiota may potentially affect risk of T2D. In addition, these results are in line with recommendations on increasing intakes of lignan-rich foods, such as whole grains, fruits, and green leafy vegetables, for the prevention of T2D.
Article Information
Funding. This study was funded by research grants CA-87969, CA-4449, DK-58845, DK-58785, DK-082486, CA-50385, CA-67262, P30-CA-71789, U54-CA-155626, and P30-DK-46200 from the National Institutes of Health (NIH). Q.S. was supported by a career development award, R00-HL-098459, from the National Heart, Lung, and Blood Institute. A.C. is a Royal Society Wolfson Research Merit Award holder.
The funding sources had no role in the study design; collection, analysis, and interpretation of data; writing of the report; or decision to submit the article for publication. The authors are not affiliated with the funding institutions.
Duality of Interest. No potential conflicts of interest relevant to this article were reported.
Author Contributions. Q.S. contributed to the data collection of dietary flavonoids or urinary metabolites, conducted pilot studies for the current investigation, provided statistical expertise, contributed to the data analysis and interpretation, wrote the first draft of the manuscript, and contributed to the critical revision of the manuscript for important intellectual content and approval of the final version of the manuscript. N.M.W. and A.P. provided statistical expertise and contributed to the critical revision of the manuscript for important intellectual content and approval of the final version of the manuscript. M.K.T. contributed to the data collection of dietary flavonoids or urinary metabolites, conducted pilot studies for the current investigation, provided statistical expertise, and contributed to the critical revision of the manuscript for important intellectual content and approval of the final version of the manuscript. A.C. and E.B.R. contributed to the data collection of dietary flavonoids or urinary metabolites, critical revision of the manuscript for important intellectual content, and approval of the final version of the manuscript. A.A.F. contributed to the data collection of dietary flavonoids or urinary metabolites, measurement of urinary metabolites with liquid chromatography-mass spectrometry, critical revision of the manuscript for important intellectual content, and approval of the final version of the manuscript. F.B.H. obtained funding from NIH, contributed to the data collection of dietary flavonoids or urinary metabolites, provided statistical expertise, and contributed to the critical revision of the manuscript for important intellectual content and approval of the final version of the manuscript. R.M.v.D. obtained funding from NIH, contributed to the data collection of dietary flavonoids or urinary metabolites, conducted pilot studies for the current investigation, provided statistical expertise, and contributed to the critical revision of the manuscript for important intellectual content and approval of the final version of the manuscript. Q.S. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
This article contains Supplementary Data online at http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc13-2513/-/DC1.
A slide set summarizing this article is available online.
References
- 1.Tham DM, Gardner CD, Haskell WL. Clinical review 97: potential health benefits of dietary phytoestrogens: a review of the clinical, epidemiological, and mechanistic evidence. J Clin Endocrinol Metab 1998;83:2223–2235 [DOI] [PubMed] [Google Scholar]
- 2.Landete JM. Plant and mammalian lignans: a review of source, intake, metabolism, intestinal bacteria and health. Food Res Int 2012;46:410–424 [Google Scholar]
- 3.Peterson J, Dwyer J, Adlercreutz H, Scalbert A, Jacques P, McCullough ML. Dietary lignans: physiology and potential for cardiovascular disease risk reduction. Nutr Rev 2010;68:571–603 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kelly MG, Hartwell JL. The biological effects and the chemical composition of podophyllin: a review. J Natl Cancer Inst 1954;14:967–1010 [PubMed] [Google Scholar]
- 5.Pan A, Demark-Wahnefried W, Ye X, et al. Effects of a flaxseed-derived lignan supplement on C-reactive protein, IL-6 and retinol-binding protein 4 in type 2 diabetic patients. Br J Nutr 2009;101:1145–1149 [DOI] [PubMed] [Google Scholar]
- 6.Prasad K. Hydroxyl radical-scavenging property of secoisolariciresinol diglucoside (SDG) isolated from flax-seed. Mol Cell Biochem 1997;168:117–123 [DOI] [PubMed] [Google Scholar]
- 7.Velentzis LS, Cantwell MM, Cardwell C, Keshtgar MR, Leathem AJ, Woodside JV. Lignans and breast cancer risk in pre- and post-menopausal women: meta-analyses of observational studies. Br J Cancer 2009;100:1492–1498 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Salvini S, Hunter DJ, Sampson L, et al. Food-based validation of a dietary questionnaire: the effects of week-to-week variation in food consumption. Int J Epidemiol 1989;18:858–867 [DOI] [PubMed] [Google Scholar]
- 9.Franke AA, Custer LJ, Wilkens LR, et al. Liquid chromatographic-photodiode array mass spectrometric analysis of dietary phytoestrogens from human urine and blood. J Chromatogr B Analyt Technol Biomed Life Sci 2002;777:45–59 [DOI] [PubMed] [Google Scholar]
- 10.McCullough ML, Feskanich D, Stampfer MJ, et al. Diet quality and major chronic disease risk in men and women: moving toward improved dietary guidance. Am J Clin Nutr 2002;76:1261–1271 [DOI] [PubMed] [Google Scholar]
- 11.Rosner B, Spiegelman D, Willett WC. Correction of logistic regression relative risk estimates and confidence intervals for random within-person measurement error. Am J Epidemiol 1992;136:1400–1413 [DOI] [PubMed] [Google Scholar]
- 12.Mazur W, Adlercreutz H. Overview of naturally occurring endocrine-active substances in the human diet in relation to human health. Nutrition 2000;16:654–658 [DOI] [PubMed] [Google Scholar]
- 13.Peñalvo JL, Adlercreutz H, Uehara M, Ristimaki A, Watanabe S. Lignan content of selected foods from Japan. J Agric Food Chem 2008;56:401–409 [DOI] [PubMed] [Google Scholar]
- 14.Heinonen S, Nurmi T, Liukkonen K, et al. In vitro metabolism of plant lignans: new precursors of mammalian lignans enterolactone and enterodiol. J Agric Food Chem 2001;49:3178–3186 [DOI] [PubMed] [Google Scholar]
- 15.Kuijsten A, Arts IC, Vree TB, Hollman PC. Pharmacokinetics of enterolignans in healthy men and women consuming a single dose of secoisolariciresinol diglucoside. J Nutr 2005;135:795–801 [DOI] [PubMed] [Google Scholar]
- 16.Nesbitt PD, Lam Y, Thompson LU. Human metabolism of mammalian lignan precursors in raw and processed flaxseed. Am J Clin Nutr 1999;69:549–555 [DOI] [PubMed] [Google Scholar]
- 17.Pérez-Jiménez J, Hubert J, Hooper L, et al. Urinary metabolites as biomarkers of polyphenol intake in humans: a systematic review. Am J Clin Nutr 2010;92:801–809 [DOI] [PubMed] [Google Scholar]
- 18.Cunnane SC, Ganguli S, Menard C, et al. High alpha-linolenic acid flaxseed (Linum usitatissimum): some nutritional properties in humans. Br J Nutr 1993;69:443–453 [DOI] [PubMed] [Google Scholar]
- 19.Lemay A, Dodin S, Kadri N, Jacques H, Forest JC. Flaxseed dietary supplement versus hormone replacement therapy in hypercholesterolemic menopausal women. Obstet Gynecol 2002;100:495–504 [DOI] [PubMed] [Google Scholar]
- 20.Pan A, Sun J, Chen Y, et al. Effects of a flaxseed-derived lignan supplement in type 2 diabetic patients: a randomized, double-blind, cross-over trial. PLoS ONE 2007;2:e1148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Rhee Y, Brunt A. Flaxseed supplementation improved insulin resistance in obese glucose intolerant people: a randomized crossover design. Nutr J 2011;10:44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Cornish SM, Chilibeck PD, Paus-Jennsen L, et al. A randomized controlled trial of the effects of flaxseed lignan complex on metabolic syndrome composite score and bone mineral in older adults. Appl Physiol Nutr Metab 2009;34:89–98 [DOI] [PubMed] [Google Scholar]
- 23.Beulens JW, van der Schouw YT, Bergmann MM, et al. InterAct Consortium Alcohol consumption and risk of type 2 diabetes in European men and women: influence of beverage type and body size The EPIC-InterAct study [published correction appears in J Intern Med 2013;273:422]. J Intern Med 2012;272:358–370 [DOI] [PubMed] [Google Scholar]
- 24.van Dam RM, Hu FB. Coffee consumption and risk of type 2 diabetes: a systematic review. JAMA 2005;294:97–104 [DOI] [PubMed] [Google Scholar]
- 25.de Munter JS, Hu FB, Spiegelman D, Franz M, van Dam RM. Whole grain, bran, and germ intake and risk of type 2 diabetes: a prospective cohort study and systematic review. PLoS Med 2007;4:e261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Muraki I, Imamura F, Manson JE, et al. Fruit consumption and risk of type 2 diabetes: results from three prospective longitudinal cohort studies. BMJ 2013;347:f5001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wedick NM, Brennan AM, Sun Q, Hu FB, Mantzoros CS, van Dam RM. Effects of caffeinated and decaffeinated coffee on biological risk factors for type 2 diabetes: a randomized controlled trial. Nutr J 2011;10:93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Adolphe JL, Whiting SJ, Juurlink BH, Thorpe LU, Alcorn J. Health effects with consumption of the flax lignan secoisolariciresinol diglucoside. Br J Nutr 2010;103:929–938 [DOI] [PubMed] [Google Scholar]
- 29.Penttinen P, Jaehrling J, Damdimopoulos AE, et al. Diet-derived polyphenol metabolite enterolactone is a tissue-specific estrogen receptor activator. Endocrinology 2007;148:4875–4886 [DOI] [PubMed] [Google Scholar]
- 30.Penttinen-Damdimopoulou PE, Power KA, Hurmerinta TT, Nurmi T, van der Saag PT, Mäkelä SI. Dietary sources of lignans and isoflavones modulate responses to estradiol in estrogen reporter mice. Mol Nutr Food Res 2009;53:996–1006 [DOI] [PubMed] [Google Scholar]
- 31.Damdimopoulou P, Nurmi T, Salminen A, et al. A single dose of enterolactone activates estrogen signaling and regulates expression of circadian clock genes in mice. J Nutr 2011;141:1583–1589 [DOI] [PubMed] [Google Scholar]
- 32.Chen JQ, Brown TR, Russo J. Regulation of energy metabolism pathways by estrogens and estrogenic chemicals and potential implications in obesity associated with increased exposure to endocrine disruptors. Biochim Biophys Acta 2009;1793:1128–1143 [DOI] [PMC free article] [PubMed]
- 33.Nadal A, Alonso-Magdalena P, Soriano S, Quesada I, Ropero AB. The pancreatic beta-cell as a target of estrogens and xenoestrogens: implications for blood glucose homeostasis and diabetes. Mol Cell Endocrinol 2009;304:63–68 [DOI] [PubMed] [Google Scholar]
- 34.Adlercreutz H, Mousavi Y, Clark J, et al. Dietary phytoestrogens and cancer: in vitro and in vivo studies. J Steroid Biochem Mol Biol 1992;41:331–337 [DOI] [PubMed] [Google Scholar]
- 35.Martin ME, Haourigui M, Pelissero C, Benassayag C, Nunez EA. Interactions between phytoestrogens and human sex steroid binding protein. Life Sci 1996;58:429–436 [DOI] [PubMed] [Google Scholar]
- 36.Ding EL, Song Y, Manson JE, et al. Sex hormone-binding globulin and risk of type 2 diabetes in women and men. N Engl J Med 2009;361:1152–1163 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Prasad K. Secoisolariciresinol diglucoside from flaxseed delays the development of type 2 diabetes in Zucker rat. J Lab Clin Med 2001;138:32–39 [DOI] [PubMed] [Google Scholar]
- 38.Fukumitsu S, Aida K, Ueno N, Ozawa S, Takahashi Y, Kobori M. Flaxseed lignan attenuates high-fat diet-induced fat accumulation and induces adiponectin expression in mice. Br J Nutr 2008;100:669–676 [DOI] [PubMed] [Google Scholar]
- 39.Diamant M, Blaak EE, de Vos WM. Do nutrient-gut-microbiota interactions play a role in human obesity, insulin resistance and type 2 diabetes? Obes Rev 2011;12:272–281 [DOI] [PubMed] [Google Scholar]