

Abstract
Hydrocele of the canal of Nuck is a rare condition in females. It results from the failure of obliteration of the distal portion of evaginated parietal peritoneum within the inguinal canal which forms a sac containing fluid. Patients generally present with inguinal swelling. We present a case of left sided cyst of canal of Nuck with left inguinal hernia in a 28-year-old female, which was diagnosed on ultrasonography. Patient underwent laparoscopic excision of cyst of canal of nuck with hernioplasty. Histopathology confirmed the diagnosis. To our knowledge, this is the first reported case of laparoscopic excision of a cyst (encysted hydrocele) of the canal of Nuck.
Keywords: Cyst of canal of Nuck, hydrocoele of canal of nuck, laparoscopic excision of cyst of canal of Nuck
INTRODUCTION
The round ligament is attached to the uterus and a small evagination of the parietal peritoneum accompanies the round ligament through the inguinal ring into the inguinal canal in the female. This small evagination of the parietal peritoneum is the canal of Nuck in the female, which is homologous to the processus vaginalis in males. The canal of Nuck is normally obliterated in the first year of life. Failure to achieve complete obliteration results in an indirect inguinal hernia or hydrocele of the canal of Nuck, which is a rare entity.[1,2] We present aa case of cyst of canal of nuck in a 28-year-old female, who underwent laparoscopic excision of cyst of canal of Nuck. To our knowledge, this is the first case report of laparoscopic excision of cyst of canal of Nuck.
CASE REPORT
A 28-year-old female presented with complaint of pain and swelling in her left inguinal region since 1 month. Swelling was insidious in onset, with a slight increase in the size of the swelling since its occurrence. There was no history of vomiting, bowel and bladder dysfunction. On examination, an oval, approximately 4 × 3 cm in size, tender, cystic and fluctuant swelling was present in the left inguinal region. Transillumination test was negative. Swelling was irreducible against manual pressure. There was no expansible cough impulse, peristaltic activity or abnormal vascularity-associated with the swelling. Signs of inflammation were absent. Lymph nodal examination was normal. Ultrasonography revealed left inguinal hernia, with well-defined, oval, anechoic cystic swelling within the inguinal canal measuring 4 × 3 cm [Figure 1]. Patient underwent laparoscopic excision of cyst of canal of Nuck with left inguinal hernioplasty. Peritoneum was opened and hernia defect was identified [Figure 2]. Round ligament was identified along with the hydrocele of the canal of Nuck. Cyst of canal of nuck was separated from the round ligament and excision of the cyst of canal of Nuck was carried out [Figure 3]. A 15 × 10 cm polypropylene (Prolene, Ethicon, Mumbai, India) mesh was placed to cover the hernia defect [Figure 4]. Peritoneal flaps were approximated. Post-operative period was uneventful and patient recovered satisfactorily. Histopathologic examination confirmed it as Hydrocoele of canal of Nuck. Patient is asymptomatic on follow up.
Figure 1.
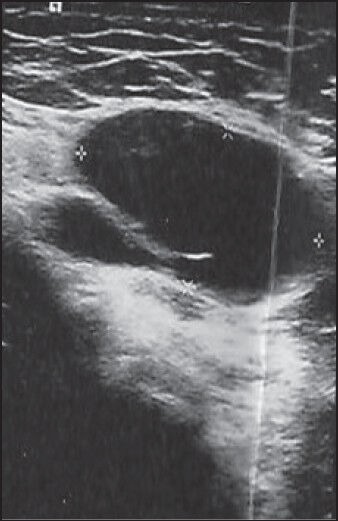
Ultrasonography of left inguinal region showing a well defined, oval, anechoic cystic lesion within the inguinal canal, measuring 4 × 3 cm
Figure 2.
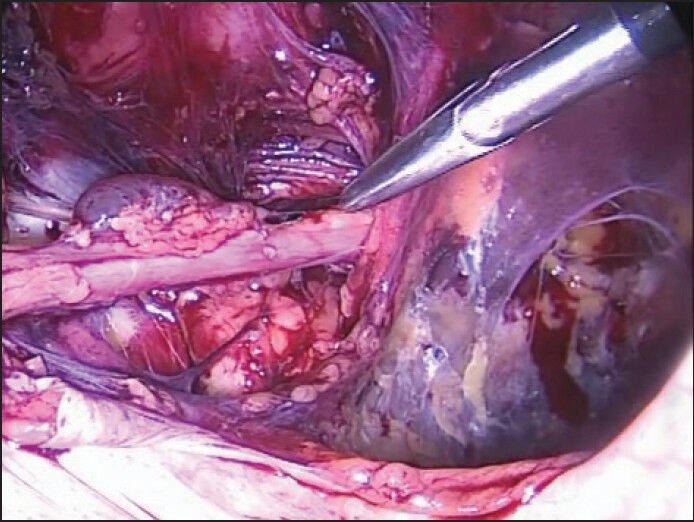
Intra-operative picture showing left round ligament with cyst of canal of Nuck
Figure 3.
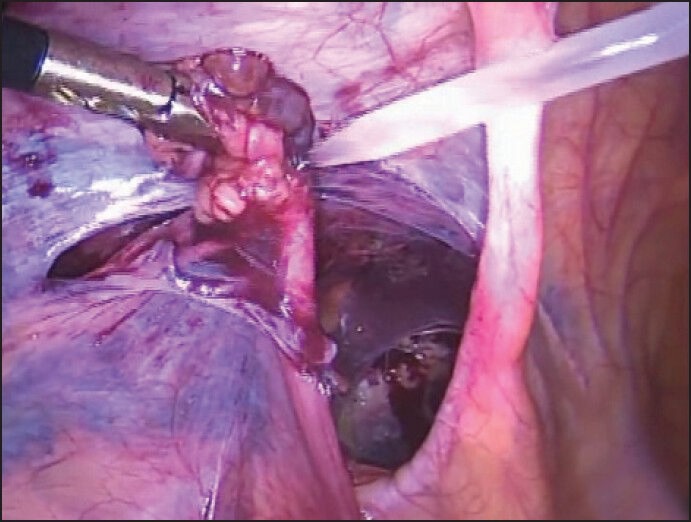
Endoloop being placed at proximal end for excision of cyst of canal of Nuck
Figure 4.
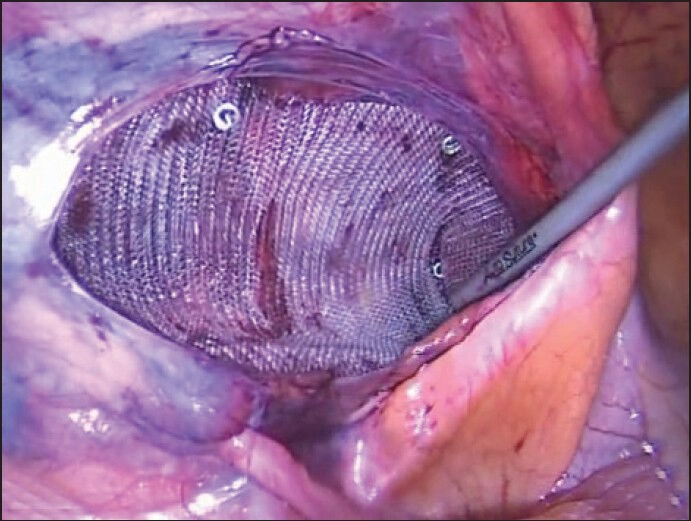
Polypropylene mesh placement for covering the left myopectineal orifice
DISCUSSION
Owing to its rarity and the unawareness among clinicians, due to the lack of literature in surgical and gynaecological textbooks, Hydrocele of the canal of Nuck is a seldom encountered entity in clinical practice and is commonly mistaken for inguinal hernia as one-third of the cases of the former are concomitantly present with the latter.[3]
The canal of Nuck was first described by the Dutch anatomist Anton Nuck in 1691. The processus vaginalis within the inguinal canal in women is, therefore, called the canal of Nuck. The Hydrocele of the canal of Nuck is a very rare condition and results from the failure of obliteration of the distal portion of the canal which forms a fluid containing sac. The Hydrocele of the canal of Nuck generally manifests as a painless swelling in the inguinal area and labium in adolescent age groups. Occasionally, it may present with dull aching pain. The size of the lesion is usually small, averaging about 3 cm in length and about 0.3-0.5 cm in diameter.[4]
Ultrasound is the preferred investigation due to the superficiality of the lesion and is well-visualised with a high frequency linear array transducer. The lesion is typically seen as a well-defined hypoechoic or anechoic, sausage- or comma-shaped mass lying superficially and medial to the pubic bone in the inguinal canal with enhanced posterior through translucency. It may show cystic in appearance as in our case, or with septations within the lesion.[4]
Magnetic Resonance Imaging can give more precise images including septation and a communication between cystic lesion and peritoneal cavity and information on the anatomical relation with adjacent structures. Therefore, MRI can help to diagnose in patients with inguinal cystic mass.[4]
The differential diagnosis of a cystic mass in the female groin region includes round ligament cysts, varicosities of the round ligament, inguinal herniation of the ovary, cystic lymphangiomas, epidermal inclusion cysts, abscesses and pseudoaneurysms.[1]
The final diagnosis is made during surgery and confirmed by pathological examination. Surgical resection of the hydrocele and ligation of the neck of the processus vaginalis should be considered as standard therapy.[1]
To the best of our knowledge, only open excision of the cyst of canal of Nuck has been reported in the literature, and this is the first case report of laparoscopic excision of cyst of canal of Nuck.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Choi YM, Lee GM, Yi JB, Yoon KL, Shim KS, Bae CW, et al. Two cases of female hydrocele of the canal of nuck. Korean J Pediatr. 2012;55:143–6. doi: 10.3345/kjp.2012.55.4.143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Park SJ, Lee HK, Hong HS, Kim HC, Kim DH, Park JS, et al. Hydrocele of the canal of Nuck in a girl: Ultrasound and MR appearance. Br J Radiol. 2004;77:243–4. doi: 10.1259/bjr/51474597. [DOI] [PubMed] [Google Scholar]
- 3.Jagdale R, Agrawal S, Chhabra S, Jewan SY. Hydrocele of the canal of Nuck: Value of radiological diagnosis. J Radiol Case Rep. 2012;6:18–22. doi: 10.3941/jrcr.v6i6.916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Manjunatha YC, Beeregowda YC, Bhaskaran A. Hydrocele of the canal of Nuck: Imaging findings. Acta Radiol Short Rep. 2012;1:12–5. doi: 10.1258/arsr.2012.110016. [DOI] [PMC free article] [PubMed] [Google Scholar]