

A 9-year-old, 16-kg (body surface area 0.7 m2) girl, 8 years post-transplant, was referred to our heart transplant clinic after a family relocation. She had developed renal insufficiency, which was attributed to calcineurin-induced nephrotoxicity. Multiple months prior to her presentation to our clinic, she was switched to a lower dose of tacrolimus, and sirolimus was added to her anti-rejection regimen. Despite these changes, her renal function worsened with a peak serum creatinine of 1.9 mg/dl, and she developed hematuria. Further evaluation included urine and serum BK viral polymerase chain reaction tests, which were positive at 1.22e10 copies/ml and 7.13e5 copies/ml, respectively (SmartCycler; Cepheid, Sunnyvale, CA). Creatinine clearance at that time was measured by a 24-hour urine collection to be 20 ml/min/1.73 m2. Subsequent renal biopsy performed showed BK virus nephropathy (Figure 1).
Figure 1.
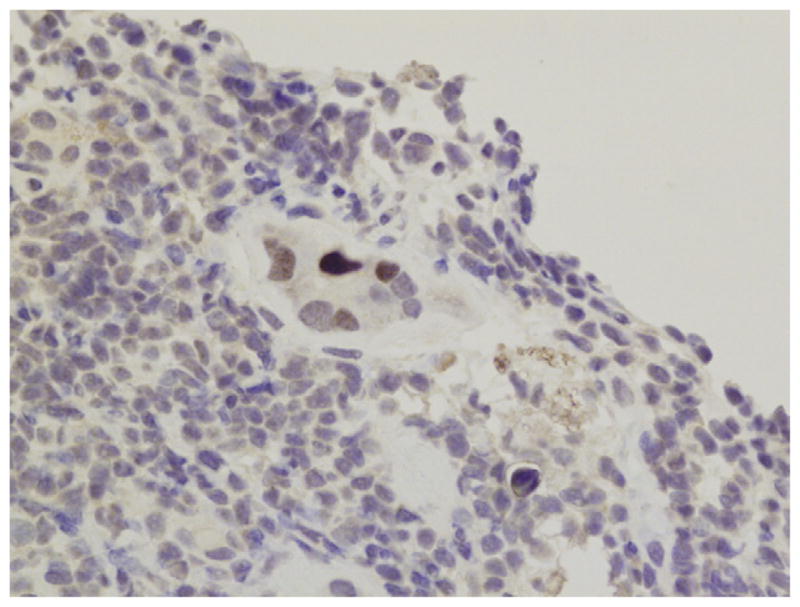
Immunohistochemical stain for big “T” antigen specific for polyoma virus replication. The tubule in the center of the figure is positive for big T antigen, as demonstrated by its dark brown color.
The patient was initiated on leflunomide (Arava; Sanofi Aventis, Bridgewater, NJ) to aggressively treat BK virus nephropathy and to decrease the risk of rejection. Leflunomide was started 2 weeks after stopping the sirolimus. The tacrolimus goal level while on leflunomide was 8 to 10 ng/ml. Her leflunomide regimen consisted of 40 mg/day for 2 days, and then maintenance therapy at 10 mg/day.1 Teriflunomide (Mayo Medical Laboratories, St. Paul, MN) levels were checked monthly, with goal of 30 to 60 μg/ml. Liver chemistries, electrolytes and complete blood counts were checked bi-weekly. She was maintained on leflunomide 10 mg/day for the vast majority of treatment (range 7.5 to 15 mg/day). Therapy was withheld twice during the course of treatment due to mild rise in transaminases. After 10 months of therapy, serum BK viral load decreased to 1,176 copies/ml and creatinine was 1.1 mg/dl (Figure 2). Leflunomide treatment was stopped based on improved kidney function and reduced BK viremia. She was maintained on tacrolimus alone until teriflunomide levels were undetectable, and then sirolimus was restarted. The patient has maintained a serum creatinine of 1.2 mg/dl at 5 months after stopping leflunomide.
Figure 2.
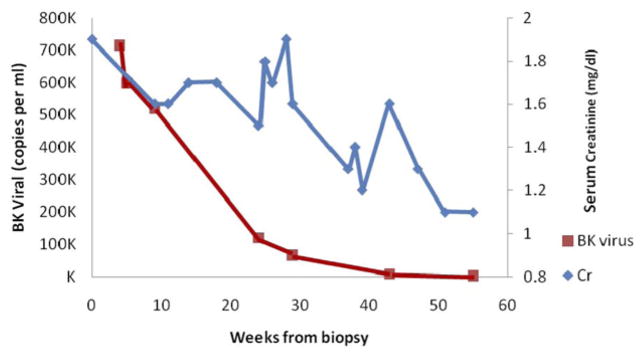
Serum creatinine and serum BK viral load over time, with Week 0 being the time of biopsy. Therapy was held from Weeks 18 to 22 (influenza) and Weeks 36 to 38 (teriflunomide level 81 μg/ml). Leflunomide began at Week 4.
Discussion
BK nephropathy is a significant cause of morbidity and mortality in kidney transplant patients. Its prevalence and involvement in renal pathology in heart transplant recipients is being increasingly recognized.2 Our case highlights the importance of BK nephropathy as part of the differential diagnosis of renal insufficiency post–cardiac transplantation, especially if combined with hematuria. It is difficult from this case to determine the exact contribution of BK virus to the patient’s renal insufficiency. It is possible that renal insufficiency from immunosuppressant medications was present and BK virus replication only augmented this process. When leflunomide treatment was withheld, renal function, as measured by serum creatinine, fluctuated despite a continued reduction in serum BK viral load. Calcineurin inhibitor exposure during these times may have been the reason for the fluctuation in renal function, indicating that calcineurin inhibitor–induced renal arteriole constriction was playing a significant role in the patient’s renal pathology.
Because this is a single case report, the effectiveness of leflunomide therapy versus changes in immunosuppression regimen on outcomes cannot be conclusively determined. At the time of this report, the patient had only 5 months of follow-up on sirolimus therapy. This may not have been a long enough time frame for recurrence of renal dysfunction with reinitiation of baseline immunosuppression or recurrence of BK viremia. A post-treatment renal biopsy would have been helpful in elucidating any pathologic changes after therapy.
Early diagnosis of BK nephropathy and even treatment of BK viremia has been associated with better outcomes in other transplanted organs.3 Leflunomide has the therapeutic effects of both immunosuppressive and anti-viral properties, making it an option for treating BK nephropathy. Our case highlights the need for further study of the incidence of BK nephropathy in non-kidney solid-organ transplant recipients, as well as a need for developing randomized clinical trials on different proposed treatment modalities.
Footnotes
Disclosure statement
The authors have no conflicts of interest to disclose. We thank Dr Geoffrey Forbus, Dr John Orak, Dr Sally Self and Amanda Forbus for their contributions.
References
- 1.Araya CE, Garin EH, Neiberger RE, et al. Leflunomide therapy for BK virus allograft nephropathy in pediatric and young adult kidney transplant recipients. Pediatr Transplant. 2010;14:145–50. doi: 10.1111/j.1399-3046.2009.01183.x. [DOI] [PubMed] [Google Scholar]
- 2.Loeches B, Valerio M, Palomo J, et al. BK virus in heart transplant recipients: a prospective study. J Heart Lung Transplant. 2011;30:109–11. doi: 10.1016/j.healun.2010.08.028. [DOI] [PubMed] [Google Scholar]
- 3.Ginevri F, Azzi A, Hirsch HH, et al. Prospective monitoring of polyomavirus BK replication and impact of pre-emptive intervention in pediatric kidney recipients. Am J Transplant. 2007;7:2727–35. doi: 10.1111/j.1600-6143.2007.01984.x. [DOI] [PubMed] [Google Scholar]